Guidelines of Hypertension – 2020 Barroso Et Al
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Guidelines on Paediatric Urology S
Guidelines on Paediatric Urology S. Tekgül (Chair), H.S. Dogan, E. Erdem (Guidelines Associate), P. Hoebeke, R. Ko˘cvara, J.M. Nijman (Vice-chair), C. Radmayr, M.S. Silay (Guidelines Associate), R. Stein, S. Undre (Guidelines Associate) European Society for Paediatric Urology © European Association of Urology 2015 TABLE OF CONTENTS PAGE 1. INTRODUCTION 7 1.1 Aim 7 1.2 Publication history 7 2. METHODS 8 3. THE GUIDELINE 8 3A PHIMOSIS 8 3A.1 Epidemiology, aetiology and pathophysiology 8 3A.2 Classification systems 8 3A.3 Diagnostic evaluation 8 3A.4 Disease management 8 3A.5 Follow-up 9 3A.6 Conclusions and recommendations on phimosis 9 3B CRYPTORCHIDISM 9 3B.1 Epidemiology, aetiology and pathophysiology 9 3B.2 Classification systems 9 3B.3 Diagnostic evaluation 10 3B.4 Disease management 10 3B.4.1 Medical therapy 10 3B.4.2 Surgery 10 3B.5 Follow-up 11 3B.6 Recommendations for cryptorchidism 11 3C HYDROCELE 12 3C.1 Epidemiology, aetiology and pathophysiology 12 3C.2 Diagnostic evaluation 12 3C.3 Disease management 12 3C.4 Recommendations for the management of hydrocele 12 3D ACUTE SCROTUM IN CHILDREN 13 3D.1 Epidemiology, aetiology and pathophysiology 13 3D.2 Diagnostic evaluation 13 3D.3 Disease management 14 3D.3.1 Epididymitis 14 3D.3.2 Testicular torsion 14 3D.3.3 Surgical treatment 14 3D.4 Follow-up 14 3D.4.1 Fertility 14 3D.4.2 Subfertility 14 3D.4.3 Androgen levels 15 3D.4.4 Testicular cancer 15 3D.5 Recommendations for the treatment of acute scrotum in children 15 3E HYPOSPADIAS 15 3E.1 Epidemiology, aetiology and pathophysiology -

Summary of Product Characteristics
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT *IPERTEN/ARTEDIL/MANYPER 10mg tablets IPERTEN/ARTEDIL/MANYPER 20mg tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION IPERTEN/ARTEDIL/MANYPER 10 mg tablets Each tablet contains: Manidipine hydrochloride 10mg Excipient with known effect: 119,61 mg lactose monohydrate/tablet IPERTEN/ARTEDIL/MANYPER 20 mg tablets Each tablet contains: Manidipine hydrochloride 20mg Excipient with known effect: 131,80 mg lactose monohydrate/tablet For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Tablet IPERTEN/ARTEDIL/MANYPER 10mg: pale yellow, round, scored tablet; IPERTEN/ARTEDIL/MANYPER 20mg: yellow-orange, oblong, scored tablet. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Mild to moderate essential hypertension 4.2 Posology and method of administration The recommended starting dose is 10 mg once a day. Should the antihypertensive effect be still insufficient after 2-4 weeks of treatment, it is advisable to increase the dosage to the usual maintenance dose of 20 mg once a day. Elderly In view of the slowing down of metabolism in the elderly, the recommended dose is 10mg once daily. This dosage is sufficient in most elderly patients; the risk/benefit of any dose increase should be considered with caution on an individual basis. Renal impairment In patients with mild to moderate renal dysfunction care should be taken when increasing the dosage from 10 to 20mg once a day. Hepatic impairment Due to the extensive hepatic metabolisation of manidipine, patients with mild hepatic dysfunction should not exceed 10mg once a day (see also Section 4.3 Contraindications). Tablet must be swallowed in the morning after breakfast, without chewing it, with a few liquid. -

The Repurposing Drugs in Oncology Database
ReDO_DB: the repurposing drugs in oncology database Pan Pantziarka1,2, Ciska Verbaanderd1,3, Vidula Sukhatme4, Rica Capistrano I1, Sergio Crispino1, Bishal Gyawali1,5, Ilse Rooman1,6, An MT Van Nuffel1, Lydie Meheus1, Vikas P Sukhatme4,7 and Gauthier Bouche1 1The Anticancer Fund, Brussels, 1853 Strombeek-Bever, Belgium 2The George Pantziarka TP53 Trust, London, UK 3Clinical Pharmacology and Pharmacotherapy, Department of Pharmaceutical and Pharmacological Sciences, KU Leuven, Leuven, Belgium 4GlobalCures Inc., Newton, MA 02459 USA 5Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA 02115 USA 6Oncology Research Centre, Vrije Universiteit Brussel, Brussels, Belgium 7Emory University School of Medicine, Atlanta, GA 30322 USA Correspondence to: Pan Pantziarka. Email: [email protected] Abstract Repurposing is a drug development strategy that seeks to use existing medications for new indications. In oncology, there is an increased level of activity looking at the use of non-cancer drugs as possible cancer treatments. The Repurposing Drugs in Oncology (ReDO) project has used a literature-based approach to identify licensed non-cancer drugs with published evidence of anticancer activity. Data from 268 drugs have been included in a database (ReDO_DB) developed by the ReDO project. Summary results are outlined and an assessment Research of clinical trial activity also described. The database has been made available as an online open-access resource (http://www.redo-project. org/db/). Keywords: drug repurposing, repositioning, ReDO project, cancer drugs, online database Published: 06/12/2018 Received: 27/09/2018 ecancer 2018, 12:886 https://doi.org/10.3332/ecancer.2018.886 Copyright: © the authors; licensee ecancermedicalscience. -

IPEG's 25Th Annual Congress Forendosurgery in Children
IPEG’s 25th Annual Congress for Endosurgery in Children Held in conjunction with JSPS, AAPS, and WOFAPS May 24-28, 2016 Fukuoka, Japan HELD AT THE HILTON FUKUOKA SEA HAWK FINAL PROGRAM 2016 LY 3m ON m s ® s e d’ a rl le o r W YOU ASKED… JustRight Surgical delivered W r o e r l ld p ’s ta O s NL mm Y classic 5 IPEG…. Now it’s your turn RIGHT Come try these instruments in the Hands-On Lab: SIZE. High Fidelity Neonatal Course RIGHT for the Advanced Learner Tuesday May 24, 2016 FIT. 2:00pm - 6:00pm RIGHT 357 S. McCaslin, #120 | Louisville, CO 80027 CHOICE. 720-287-7130 | 866-683-1743 | www.justrightsurgical.com th IPEG’s 25 Annual Congress Welcome Message for Endosurgery in Children Dear Colleagues, May 24-28, 2016 Fukuoka, Japan On behalf of our IPEG family, I have the privilege to welcome you all to the 25th Congress of the THE HILTON FUKUOKA SEA HAWK International Pediatric Endosurgery Group (IPEG) in 810-8650, Fukuoka-shi, 2-2-3 Jigyohama, Fukuoka, Japan in May of 2016. Chuo-ku, Japan T: +81-92-844 8111 F: +81-92-844 7887 This will be a special Congress for IPEG. We have paired up with the Pacific Association of Pediatric Surgeons International Pediatric Endosurgery Group (IPEG) and the Japanese Society of Pediatric Surgeons to hold 11300 W. Olympic Blvd, Suite 600 a combined meeting that will add to our always-exciting Los Angeles, CA 90064 IPEG sessions a fantastic opportunity to interact and T: +1 310.437.0553 F: +1 310.437.0585 learn from the members of those two surgical societies. -

Ovid MEDLINE(R)
Supplementary material BMJ Open Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations and Daily <1946 to September 16, 2019> # Searches Results 1 exp Hypertension/ 247434 2 hypertens*.tw,kf. 420857 3 ((high* or elevat* or greater* or control*) adj4 (blood or systolic or diastolic) adj4 68657 pressure*).tw,kf. 4 1 or 2 or 3 501365 5 Sex Characteristics/ 52287 6 Sex/ 7632 7 Sex ratio/ 9049 8 Sex Factors/ 254781 9 ((sex* or gender* or man or men or male* or woman or women or female*) adj3 336361 (difference* or different or characteristic* or ratio* or factor* or imbalanc* or issue* or specific* or disparit* or dependen* or dimorphism* or gap or gaps or influenc* or discrepan* or distribut* or composition*)).tw,kf. 10 or/5-9 559186 11 4 and 10 24653 12 exp Antihypertensive Agents/ 254343 13 (antihypertensiv* or anti-hypertensiv* or ((anti?hyperten* or anti-hyperten*) adj5 52111 (therap* or treat* or effective*))).tw,kf. 14 Calcium Channel Blockers/ 36287 15 (calcium adj2 (channel* or exogenous*) adj2 (block* or inhibitor* or 20534 antagonist*)).tw,kf. 16 (agatoxin or amlodipine or anipamil or aranidipine or atagabalin or azelnidipine or 86627 azidodiltiazem or azidopamil or azidopine or belfosdil or benidipine or bepridil or brinazarone or calciseptine or caroverine or cilnidipine or clentiazem or clevidipine or columbianadin or conotoxin or cronidipine or darodipine or deacetyl n nordiltiazem or deacetyl n o dinordiltiazem or deacetyl o nordiltiazem or deacetyldiltiazem or dealkylnorverapamil or dealkylverapamil -

174-Atypical Antipsychotics and Sleepwalkingsleep-Related Eating
Atypical antipsychotics and sleepwalking/sleep-related eating disorder CONFIDENTIAL Medicines Adverse Reactions Committee Meeting date 3 July 2018 Agenda item 3.2.2 Title Atypical antipsychotics and sleepwalking/sleep-related eating disorder Medsafe For advice Submitted by Paper type Pharmacovigilance Team Active constituent Medicine Sponsors Amisulpride Solian Sanofi-Aventis Sulprix Mylan Aripiprazole Abilify Pharmacy Retailing Aripiprazole Sandoz Novartis Clozapine Clopine Douglas Pharmaceuticals Clozaril Mylan Olanzapine Olanzapine DRLA Dr Reddy’s Zypine Mylan Zyprexa Eli Lilly Paliperidone Invega Janssen-Cilag Quetiapine Auro-Quetiapine Aurobindo Pharma DP-Quetiapine Douglas Pharmaceuticals Quetapel Mylan Quetiapine DRLA Dr Reddy’s Seroquel AstraZeneca Risperidone Ridal Douglas Pharmaceuticals Risperdal Janssen-Cilag Risperidone DRLA Dr Reddy’s Risperidone (Teva) Teva Pharma Risperon Mylan Ziprasidone Zeldox Pfizer Zusdone Douglas Pharmaceuticals Funding All of the above active constituents have a funded brand with the exception of paliperidone. The special authority criteria for aripiprazole was removed on 1 June 2018. Previous MARC Atypical antipsychotics and sleepwalking/sleep-related eating disorder has meetings not been discussed previously. International action Health Canada − In September 2017, Health Canada issued a safety review on the potential risk of sleepwalking and sleep-related eating disorder associated with atypical antipsychotics. Based on this review, Health Canada has recommended updating the product safety information -

Ultrasonographic and Radiographic Diagnosis of Ectopic Ureter in a Dog
Acta Scientiae Veterinariae, 2021. 49(Suppl 1): 613. CASE REPORT ISSN 1679-9216 Pub. 613 Ultrasonographic and Radiographic Diagnosis of Ectopic Ureter in a Dog Carmen Vládia Soares de Sousa, Caroline Coelho Rocha, Roberto Sávio Bessa da Silva, Araceli Alves Dutra, Brizza Zorayd Luz Lopes Rocha, Thays Ribeiro Pacó & João Marcelo Azevedo de Paula Antunes ABSTRACT Background: Ureteral ectopia (or ectopic ureter) is a congenital anomaly of the urinary system in which the ureter inserts anywhere other than the vesical trigone. This anatomical change may have unilateral or bilateral involvement. The most evident clinical sign, occurring mostly in females, is urinary incontinence, however in some cases the condition may progress to nephritis and dilation of the renal pelvis. The diagnosis is established through imaging, and definitive treatment requires surgical approach. The present study reports a case of ureteral ectopia in a dog which was diagnosed by ultrasound and contrast radiography (excretory urography) and successfully treated by neoureterostomy. Case: A 10-month-old female American Pit Bull Terrier was attended at the Veterinary Hospital of the Federal Rural Uni- versity of the Semi-Arid (UFERSA), in Mossoró, RN. Her owner reported incontinence of dark, malodorous urine since birth as the chief complaint. After clinical examination, cystitis was suspected, and a complete blood count, urinalysis, and abdominal ultrasound was requested. The blood count and creatinine were within the reference values. The presence of struvite crystals were found on urinalysis. Ultrasound examination revealed a tortuous, dilated right ureter from the renal pelvis to the urinary bladder; no uroliths were identified as a cause of potential obstruction, but the ipsilateral kidney showed increased cortical echogenicity, loss of corticomedullary definition, and moderate pelvic dilation. -

Specialist Clinic Referral Guidelines UROLOGY
Specialist Clinic Referral Guidelines UROLOGY Please fax referrals to The Alfred Specialist Clinics on 9076 6938. The Alfred Specialist Clinics Referral Form is available to print and fax. Where appropriate and available, the referral may be directed to an alternative specialist clinic or service. Advice regarding referral for specific conditions to the Alfred Urology Service can be found here. The clinical information provided in the referral will determine the triage category. The triage category will affect the timeframe in which the patient is offered an appointment. Notification will be sent when the referral is received. The referral may be declined if it does not contain essential information required for triage, if the condition is not appropriate for referral to a public hospital, or is a condition not routinely seen at Alfred Health. Referral to Victorian public hospitals is not appropriate for: Mild to moderate lower urinary tract symptoms that have not been treated Lower urinary tract symptoms that have responded to medical management Simple renal cysts Asymptomatic epididymal cyst not identified through ultrasound Patients who have not yet tried, or failed, conservative treatment for urinary incontinence Cosmetic surgery including circumcision, penile enhancements & penile implants (see Victorian DHHS Aesthetic procedures and indications for surgery in Victorian public health services.) The following conditions are not routinely seen at Alfred Health: Patients who are being treated for the same condition at another Victorian public hospital Children under 18 years of age Vasectomy reversal Erectile dysfunction unrelated to previous surgery, trauma or radiation therapy Infertility Surgery Please refer to the Department of Health and Human Services (DHHS) Statewide Referral Criteria for Specialist Clinics for further information when referring to Urology specialist clinics in public hospitals. -
Exploring Inflammatory Status in Febrile Seizures Associated With
brain sciences Article Exploring Inflammatory Status in Febrile Seizures Associated with Urinary Tract Infections: A Two-Step Cluster Approach Raluca Maria Costea 1,2,3,* , Ionela Maniu 1,4 , Luminita Dobrota 3, Rubén Pérez-Elvira 5 , Maria Agudo 5, Javier Oltra-Cucarella 6 , Andrei Dragomir 7 , Ciprian Bacilă 3, Adela Banciu 8, Daniel Dumitru Banciu 8, 3 3 1,3,9, Călin Remus Cipăian , Roxana Cris, an and Bogdan Neamtu * 1 Pediatric Research Department, Pediatric Clinical Hospital Sibiu, 550166 Sibiu, Romania; [email protected] 2 Pediatric Neurology Department, Pediatric Clinical Hospital Sibiu, 550166 Sibiu, Romania 3 Faculty of Medicine, Lucian Blaga University of Sibiu, 550024 Sibiu, Romania; [email protected] (L.D.); [email protected] (C.B.); [email protected] (C.R.C.); [email protected] (R.C.) 4 Research Center in Informatics and Information Technology, Mathematics and Informatics Department, Faculty of Sciences, Lucian Blaga University of Sibiu, 550024 Sibiu, Romania 5 Neuropsychophysiology Laboratory, NEPSA Rehabilitación Neurológica, 37003 Salamanca, Spain; [email protected] (R.P.-E.); [email protected] (M.A.) 6 Department of Health Psychology, Universidad Miguel Hernández de Elche, 03202 Elche, Spain; [email protected] 7 N.1 Institute for Health, National University of Singapore, Singapore 117575, Singapore; [email protected] 8 Department of Bioengineering and Biotechnology, Faculty of Medical Engineering, Citation: Costea, R.M.; Maniu, I.; Politechnic University of Bucharest, 011061 Bucharest, Romania; [email protected] (A.B.); Dobrota, L.; Pérez-Elvira, R.; Agudo, [email protected] (D.D.B.) 9 Computer and Electrical Engineering Department, Faculty of Engineering, Lucian Blaga University of Sibiu, M.; Oltra-Cucarella, J.; Dragomir, A.; 550024 Sibiu, Romania Bacil˘a,C.; Banciu, A.; Banciu, D.D.; * Correspondence: [email protected] (R.M.C.); [email protected] (B.N.); et al. -

Drugs for Primary Prevention of Atherosclerotic Cardiovascular Disease: an Overview of Systematic Reviews
Supplementary Online Content Karmali KN, Lloyd-Jones DM, Berendsen MA, et al. Drugs for primary prevention of atherosclerotic cardiovascular disease: an overview of systematic reviews. JAMA Cardiol. Published online April 27, 2016. doi:10.1001/jamacardio.2016.0218. eAppendix 1. Search Documentation Details eAppendix 2. Background, Methods, and Results of Systematic Review of Combination Drug Therapy to Evaluate for Potential Interaction of Effects eAppendix 3. PRISMA Flow Charts for Each Drug Class and Detailed Systematic Review Characteristics and Summary of Included Systematic Reviews and Meta-analyses eAppendix 4. List of Excluded Studies and Reasons for Exclusion This supplementary material has been provided by the authors to give readers additional information about their work. © 2016 American Medical Association. All rights reserved. 1 Downloaded From: https://jamanetwork.com/ on 09/28/2021 eAppendix 1. Search Documentation Details. Database Organizing body Purpose Pros Cons Cochrane Cochrane Library in Database of all available -Curated by the Cochrane -Content is limited to Database of the United Kingdom systematic reviews and Collaboration reviews completed Systematic (UK) protocols published by by the Cochrane Reviews the Cochrane -Only systematic reviews Collaboration Collaboration and systematic review protocols Database of National Health Collection of structured -Curated by Centre for -Only provides Abstracts of Services (NHS) abstracts and Reviews and Dissemination structured abstracts Reviews of Centre for Reviews bibliographic -
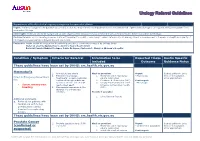
Urology Referral Guidelines
Urology Referral Guidelines Department of Health clinical urgency categories for specialist clinics Urgent: A referral is urgent if the patient has a condition that has major functional impairment and/or moderate risk of permanent damage to an organ/bone/tissue/system if not seen within 30 days. Semi Urgent: Referrals should be categorised as Semi Urgent where the patient has a condition that has the potential to deteriorate within 30-90 days. Routine: Referrals should be categorised as routine if the patient’s condition is unlikely to deteriorate quickly or have significant consequences for the person’s health and quality of life if specialist assessment is delayed beyond one month. Exclusions: Austin Health do not perform the following procedures commonly conducted by Urology Units: Refer all erectile dysfunction to Austin’s Men’s Health Clinic Refer all female Bladder Prolapse, Pelvic Prolapse, Cystocele to Mercy or Women’s Hospital Condition / Symptom Criteria for Referral Information to be Expected Triage Austin Specific included Outcome Guidance Notes These guidelines have been set by DHHS: src.health.vic.gov.au Haematuria 1. Any visible haematuria Must be provided: Urgent Instruct patient to bring 2. Persistent microscopic 1. Midstream urine microscopy - Macroscopic films to the Specialist Direct to Emergency Department haematuria: at least 2 episodes culture sensitivities Clinic appointment for: confirmed through midstream 2. Creatinine & Electrolytes (U&E) Semi-urgent specimen of urine collected at 3. Urinary Tract Ultrasound or CT - Microscopic Severe urinary tract least a week apart. Intravenous Pyelogram results bleeding 3. Macroscopic haematuria in the (IVP) absence of a urinary tract infection. -

Interactions Between Antihypertensive Drugs and Food B
11. INTERACTIONS:01. Interacción 29/11/12 14:38 Página 1866 Nutr Hosp. 2012;27(5):1866-1875 ISSN 0212-1611 • CODEN NUHOEQ S.V.R. 318 Revisión Interactions between antihypertensive drugs and food B. Jáuregui-Garrido1 and I. Jáuregui-Lobera2 1Department of Cardiology. University Hospital Virgen del Rocío. Seville. Spain. 2Bromatology and Nutrition. Pablo de Olavide University. Seville. Spain. Abstract INTERACCIONES ENTRE FÁRMACOS ANTIHIPERTENSIVOS Y ALIMENTOS Objective: A drug interaction is defined as any alter- ation, pharmacokinetics and/or pharmacodynamics, Resumen produced by different substances, other drug treatments, dietary factors and habits such as drinking and smoking. Objetivo: la interacción de medicamentos se define como These interactions can affect the antihypertensive drugs, cualquier alteración, farmacocinética y/o farmacodiná- altering their therapeutic efficacy and causing toxic mica, producida por diferentes sustancias, otros tratamien- effects. The aim of this study was to conduct a review of tos, factores dietéticos y hábitos como beber y fumar. Estas available data about interactions between antihyperten- interacciones pueden afectar a los fármacos antihipertensi- sive agents and food. vos, alterando su eficacia terapéutica y causando efectos Methods: The purpose of this review was to report an tóxicos. El objetivo de este estudio fue realizar una revisión update of main findings with respect to the interactions de los datos disponibles acerca de las interacciones entre los between food and antihypertensive drugs