Evaluation of Wheezing in the Nonasthmatic Patient
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Clinical Features of Acute Epiglottitis in Adults in the Emergency Department
대한응급의학회지 제 27 권 제 1 호 � 원저� Volume 27, Number 1, February, 2016 Eye, Ear, Nose & Oral Clinical Features of Acute Epiglottitis in Adults in the Emergency Department Department of Emergency Medicine, Seoul National University College of Medicine, Seoul, Dongguk University Ilsan Hospital, Goyang, Gyeonggi-do1, Korea Kyoung Min You, M.D., Woon Yong Kwon, M.D., Gil Joon Suh, M.D., Kyung Su Kim, M.D., Jae Seong Kim, M.D.1, Min Ji Park, M.D. Purpose: Acute epiglottitis is a potentially fatal condition Key Words: Epiglottitis, Emergency medical services, Fever, that can result in airway obstruction. The aim of this study is Intratracheal Intubation to examine the clinical features of adult patients who visited the emergency department (ED) with acute epiglottitis. Methods: This retrospective observational study was con- Article Summary ducted at a single tertiary hospital ED from November 2005 What is already known in the previous study to October 2015. We searched our electronic medical While the incidence of acute epiglottitis in children has records (EMR) system for a diagnosis of “acute epiglottitis” shown a marked decrease as a result of vaccination for and selected those patients who visited the ED. Haemophilus influenzae type b, the incidence of acute Results: A total of 28 patients were included. There was no epiglottitis in adults has increased. However, in Korea, few pediatric case with acute epiglottitis during the study period. studies concerning adult patients with acute epiglottitis The mean age of the patients was 58.0±14.8 years. The who present to the emergency department (ED) have been peak incidences were in the sixth (n=7, 25.0%) and eighth reported. -

Diagnosing Pulmonary Embolism M Riedel
309 Postgrad Med J: first published as 10.1136/pgmj.2003.007955 on 10 June 2004. Downloaded from REVIEW Diagnosing pulmonary embolism M Riedel ............................................................................................................................... Postgrad Med J 2004;80:309–319. doi: 10.1136/pgmj.2003.007955 Objective testing for pulmonary embolism is necessary, embolism have a low long term risk of subse- quent VTE.2 5–7 because clinical assessment alone is unreliable and the consequences of misdiagnosis are serious. No single test RISK FACTORS AND RISK has ideal properties (100% sensitivity and specificity, no STRATIFICATION risk, low cost). Pulmonary angiography is regarded as the The factors predisposing to VTE broadly fit Virchow’s triad of venous stasis, injury to the final arbiter but is ill suited for diagnosing a disease vein wall, and enhanced coagulability of the present in only a third of patients in whom it is suspected. blood (box 1). The identification of risk factors Some tests are good for confirmation and some for aids clinical diagnosis of VTE and guides decisions about repeat testing in borderline exclusion of embolism; others are able to do both but are cases. Primary ‘‘thrombophilic’’ abnormalities often non-diagnostic. For optimal efficiency, choice of the need to interact with acquired risk factors before initial test should be guided by clinical assessment of the thrombosis occurs; they are usually discovered after the thromboembolic event. Therefore, the likelihood of embolism and by patient characteristics that risk of VTE is best assessed by recognising the may influence test accuracy. Standardised clinical presence of known ‘‘clinical’’ risk factors. estimates can be used to give a pre-test probability to However, investigations for thrombophilic dis- orders at follow up should be considered in those assess, after appropriate objective testing, the post-test without another apparent explanation. -

Table of Contents
viii Contents Chapter 1. Taking the Certification Examination . 1 General Suggestions for Preparing for the Exam About the Certification Exams Chapter 2. Developmental and Behavioral Sciences . 11 Mary Jo Gilmer, PhD, MBA, RN-BC, FAAN, and Paula Chiplis, PhD, RN, CPNP Psychosocial, Cognitive, and Ethical-Moral Development Behavior Modification Physical Development: Normal Growth Expectations and Developmental Milestones Family Concepts and Issues Family-Centered Care Cultural and Spiritual Diversity Chapter 3. Communication . 23 Mary Jo Gilmer, PhD, MBA, RN-BC, FAAN, and Karen Corlett, MSN, RN-BC, CPNP-AC/PC, PNP-BC Culturally Sensitive Communication Components of Therapeutic Communication Communication Barriers Modes of Communication Patient Confidentiality Written Communication in Nursing Practice Professional Communication Advocacy Chapter 4. The Nursing Process . 33 Clara J. Richardson, MSN, RN–BC Nursing Assessment Nursing Diagnosis and Treatment Chapter 5. Basic and Applied Sciences . 49 Mary Jo Gilmer, PhD, MBA, RN-BC, FAAN, and Paula Chiplis, PhD, RN, CPNP Trauma and Diseases Processes Common Genetic Disorders Common Childhood Diseases Traction Pharmacology Nutrition Chemistry Clinical Signs Associated With Isotonic Dehydration in Infants ix Chapter 6. Educational Principles and Strategies . 69 Mary Jo Gilmer, PhD, MBA, RN-BC, FAAN, and Karen Corlett, MSN, RN-BC, CPNP-AC/PC, PNP-BC Patient Education Chapter 7. Life Situations and Adaptive and Maladaptive Responses . 75 Mary Jo Gilmer, PhD, MBA, RN-BC, FAAN, and Karen Corlett, MSN, RN-BC, CPNP-AC/PC, PNP-BC Palliative Care End-of-Life Care Response to Crisis Chapter 8. Sensory Disorders . 87 Clara J. Richardson, MSN, RN–BC Developmental Characteristics of the Pediatric Sensory System Hearing Disorders Vision Disorders Conjunctivitis Otitis Media and Otitis Externa Retinoblastoma Trauma to the Eye Chapter 9. -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
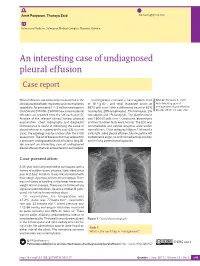
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Diagnosis of Chronic Thromboembolic Pulmonary Hypertension After Acute Pulmonary Embolism
Early View Review Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud, Marion Delcroix, Marc Humbert Please cite this article as: Klok FA, Couturaud F, Delcroix M, et al. Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.00189-2020). This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online. Copyright ©ERS 2020 Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud F2, Marion Delcroix M3, Marc Humbert4-6 1 Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, The Netherlands 2 Département de Médecine Interne et Pneumologie, Centre Hospitalo-Universitaire de Brest, Univ Brest, EA 3878, CIC INSERM1412, Brest, France 3 Department of Respiratory Diseases, University Hospitals and Respiratory Division, Department of Chronic Diseases, Metabolism & Aging, KU Leuven – University of Leuven, Leuven, Belgium 4 Université Paris-Saclay, Faculté de Médecine, Le Kremlin-Bicêtre, France 5 Service de Pneumologie et Soins Intensifs Respiratoires, Hôpital Bicêtre, AP-HP, Le Kremlin-Bicêtre, France 6 INSERM UMR S 999, Hôpital Marie Lannelongue, Le Plessis Robinson, France Corresponding author: Frederikus A. Klok, MD, FESC; Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, the Netherlands; Albinusdreef 2, 2300RC, Leiden, the Netherlands; Phone: +31- 715269111; E-mail: [email protected] Abstract Chronic thromboembolic pulmonary hypertension (CTEPH) is the most severe long-term complication of acute pulmonary embolism (PE). -

Risk of Acute Epiglottitis in Patients with Preexisting Diabetes Mellitus: a Population- Based Case–Control Study
RESEARCH ARTICLE Risk of acute epiglottitis in patients with preexisting diabetes mellitus: A population- based case±control study Yao-Te Tsai1,2, Ethan I. Huang1,2, Geng-He Chang1,2, Ming-Shao Tsai1,2, Cheng- Ming Hsu1,2, Yao-Hsu Yang3,4,5, Meng-Hung Lin6, Chia-Yen Liu6, Hsueh-Yu Li7* 1 Department of Otorhinolaryngology-Head and Neck Surgery, Chang Gung Memorial Hospital, Chiayi, Taiwan, 2 College of Medicine, Chang Gung University, Taoyuan, Taiwan, 3 Department of Traditional Chinese Medicine, Chang Gung Memorial Hospital, Chiayi, Taiwan, 4 Institute of Occupational Medicine and a1111111111 Industrial Hygiene, National Taiwan University College of Public Health, Taipei, Taiwan, 5 School of a1111111111 Traditional Chinese Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan, 6 Health a1111111111 Information and Epidemiology Laboratory, Chang Gung Memorial Hospital, Chiayi, Taiwan, 7 Department of a1111111111 Otolaryngology±Head and Neck Surgery, Linkou Chang Gung Memorial Hospital, Taoyuan, Taiwan a1111111111 * [email protected] Abstract OPEN ACCESS Citation: Tsai Y-T, Huang EI, Chang G-H, Tsai M-S, Hsu C-M, Yang Y-H, et al. (2018) Risk of acute Objective epiglottitis in patients with preexisting diabetes Studies have revealed that 3.5%±26.6% of patients with epiglottitis have comorbid diabetes mellitus: A population-based case±control study. PLoS ONE 13(6): e0199036. https://doi.org/ mellitus (DM). However, whether preexisting DM is a risk factor for acute epiglottitis remains 10.1371/journal.pone.0199036 unclear. In this study, our aim was to explore the relationship between preexisting DM and Editor: Yu Ru Kou, National Yang-Ming University, acute epiglottitis in different age and sex groups by using population-based data in Taiwan. -

Problems in Family Practice
problems in Family Practice Coughing in Childhood Hyman Sh ran d , M D Cambridge, M assachusetts Coughing in childhood is a common complaint involving a wide spectrum of underlying causes which require a thorough and rational approach by the physician. Most children who cough have relatively simple self-limiting viral infections, but some may have serious disease. A dry environment, allergic factors, cystic fibrosis, and other major illnesses must always be excluded. A simple clinical approach, and the sensible use of appropriate investigations, is most likely to succeed in finding the cause, which can allow precise management. The cough reflex as part of the defense mechanism of the respiratory tract is initiated by mucosal changes, secretions or foreign material in the pharynx, larynx, tracheobronchial Table 1. Persistent Cough — Causes in Childhood* tree, pleura, or ear. Acting as the “watchdog of the lungs,” the “good” cough prevents harmful agents from Common Uncommon Rare entering the respiratory tract; it also helps bring up irritant material from Environmental Overheating with low humidity the airway. The “bad” cough, on the Allergens other hand, serves no useful purpose Pollution Tobacco smoke and, if persistent, causes fatigue, keeps Upper Respiratory Tract the child (and parents) awake, inter Recurrent viral URI Pertussis Laryngeal stridor feres with feeding, and induces vomit Rhinitis, Pharyngitis Echo 12 Vocal cord palsy Allergic rhinitis Nasal polyp Vascular ring ing. It is best suppressed. Coughs and Prolonged use of nose drops Wax in ear colds constitute almost three quarters Sinusitis of all illness in young children. The Lower Respiratory Tract Asthma Cystic fibrosis Rt. -

COVID-19 Pneumonia: the Great Radiological Mimicker
Duzgun et al. Insights Imaging (2020) 11:118 https://doi.org/10.1186/s13244-020-00933-z Insights into Imaging EDUCATIONAL REVIEW Open Access COVID-19 pneumonia: the great radiological mimicker Selin Ardali Duzgun* , Gamze Durhan, Figen Basaran Demirkazik, Meltem Gulsun Akpinar and Orhan Macit Ariyurek Abstract Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has rapidly spread worldwide since December 2019. Although the reference diagnostic test is a real-time reverse transcription-polymerase chain reaction (RT-PCR), chest-computed tomography (CT) has been frequently used in diagnosis because of the low sensitivity rates of RT-PCR. CT fndings of COVID-19 are well described in the literature and include predominantly peripheral, bilateral ground-glass opacities (GGOs), combination of GGOs with consolida- tions, and/or septal thickening creating a “crazy-paving” pattern. Longitudinal changes of typical CT fndings and less reported fndings (air bronchograms, CT halo sign, and reverse halo sign) may mimic a wide range of lung patholo- gies radiologically. Moreover, accompanying and underlying lung abnormalities may interfere with the CT fndings of COVID-19 pneumonia. The diseases that COVID-19 pneumonia may mimic can be broadly classifed as infectious or non-infectious diseases (pulmonary edema, hemorrhage, neoplasms, organizing pneumonia, pulmonary alveolar proteinosis, sarcoidosis, pulmonary infarction, interstitial lung diseases, and aspiration pneumonia). We summarize the imaging fndings of COVID-19 and the aforementioned lung pathologies that COVID-19 pneumonia may mimic. We also discuss the features that may aid in the diferential diagnosis, as the disease continues to spread and will be one of our main diferential diagnoses some time more. -

Pathology of Allergic Bronchopulmonary Aspergillosis
[Frontiers in Bioscience 8, e110-114, January 1, 2003] PATHOLOGY OF ALLERGIC BRONCHOPULMONARY ASPERGILLOSIS Anne Chetty Department of Pediatrics, Floating Hospital for Children, New England Medical Center, Boston, MA TABLE OF CONTENTS 1. Abstract 2. Introduction 3. Immunopathogenesis 4. Pathologic Findings 4.1. Plastic bronchitis 4.2. Allergic fungal sinusitis 4.3. ABPA in cystic fibrosis 5. Acknowledgement 6. References 1. ABSTRACT Allergic bronchopulmonary aspergillosis (ABPA) individuals with episodic obstructive lung diseases such as occurs in patients with asthma and cystic fibrosis when asthma and cystic fibrosis that produce thick, tenacious Aspergillus fumigatus spores are inhaled and grow in sputum. bronchial mucus as hyphae. Chronic colonization of Aspergillus fumigatus and host’s genetically determined Decomposing organic matter serves as a substrate immunological response lead to ABPA. In most cases, for the growth of Aspergillus species. Because biologic lung biopsy is not necessary because the diagnosis is made heating produces temperatures as high as 65° to 70° C, on clinical, serologic, and roentgenographic findings. Some Aspergillus spores will not be recovered in the latter stages patients who have had lung biopsies or partial resections of composting. Aspergillus species have been recovered for atelectasis or infiltrates will have histologic diagnoses. from potting soil, mulches, decaying vegetation, and A number of different histologic diagnoses can be found sewage treatment facilities, as well as in outdoor air and even in the same patient. In the early stages the bronchial Aspergillus spores grow in excreta from birds (1) wall is infiltrated with mononuclear cells and eosinophils. Mucoid impaction and eosinophilic pneumonia are seen Allergic fungal pulmonary disease is manifested subsequently. -

Acute Pulmonary Embolism in Patients with and Without COVID-19
Journal of Clinical Medicine Article Acute Pulmonary Embolism in Patients with and without COVID-19 Antonin Trimaille 1,2 , Anaïs Curtiaud 1, Kensuke Matsushita 1,2 , Benjamin Marchandot 1 , Jean-Jacques Von Hunolstein 1 , Chisato Sato 1,2, Ian Leonard-Lorant 3, Laurent Sattler 4 , Lelia Grunebaum 4, Mickaël Ohana 3 , Patrick Ohlmann 1 , Laurence Jesel 1,2 and Olivier Morel 1,2,* 1 Division of Cardiovascular Medicine, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (A.T.); [email protected] (A.C.); [email protected] (K.M.); [email protected] (B.M.); [email protected] (J.-J.V.H.); [email protected] (C.S.); [email protected] (P.O.); [email protected] (L.J.) 2 INSERM (French National Institute of Health and Medical Research), UMR 1260, Regenerative Nanomedicine, FMTS, 67000 Strasbourg, France 3 Radiology Department, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (I.L.-L.); [email protected] (M.O.) 4 Haematology and Haemostasis Laboratory, Centre for Thrombosis and Haemostasis, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (L.S.); [email protected] (L.G.) * Correspondence: [email protected] Abstract: Introduction. Acute pulmonary embolism (APE) is a frequent condition in patients with Citation: Trimaille, A.; Curtiaud, A.; COVID-19 and is associated with worse outcomes. Previous studies suggested an immunothrombosis Matsushita, K.; Marchandot, B.; instead of a thrombus embolism, but the precise mechanisms remain unknown. -

COVID-19 Associated Pulmonary Embolism in Pediatric Patients
Prepublication Release A N O F F I C I A L J O U R N A L O F T H E A M E R I C A N A C A D E M Y O F P E D I A T R I C S COVID-19 Associated Pulmonary Embolism in Pediatric Patients Melissa Chima, Duane Williams, Neal J. Thomas, Conrad Krawiec DOI: 10.1542/hpeds.2021-005866 Journal: Hospital Pediatrics Article Type: Original Article Citation: Chima M, et al. COVID-19 Associated Pulmonary Embolism in Pediatric Patients. Hosp Pediatr. 2021; doi: 10.1542/hpeds.2021-005866 This is a prepublication version of an article that has undergone peer review and been accepted for publication but is not the final version of record. This paper may be cited using the DOI and date of access. This paper may contain information that has errors in facts, figures, and statements, and will be corrected in the final published version. The journal is providing an early version of this article to expedite access to this information. The American Academy of Pediatrics, the editors, and authors are not responsible for inaccurate information and data described in this version. Downloaded©202 from1 www.aappublications.org/news American Academy byof guest Pediatrics on October 1, 2021 Prepublication Release COVID-19 Associated Pulmonary Embolism in Pediatric Patients Melissa Chima, BS1, Duane Williams, MD2, Neal J. Thomas, MD2,3, Conrad Krawiec, MD2 Authors’ Affiliations and Addresses: 1Penn State College of Medicine, 500 University Drive, P.O. Box 850, Hershey, PA, USA 17033-0850, Tel: (717)-531-5337, Fax: (717)-531-8985.