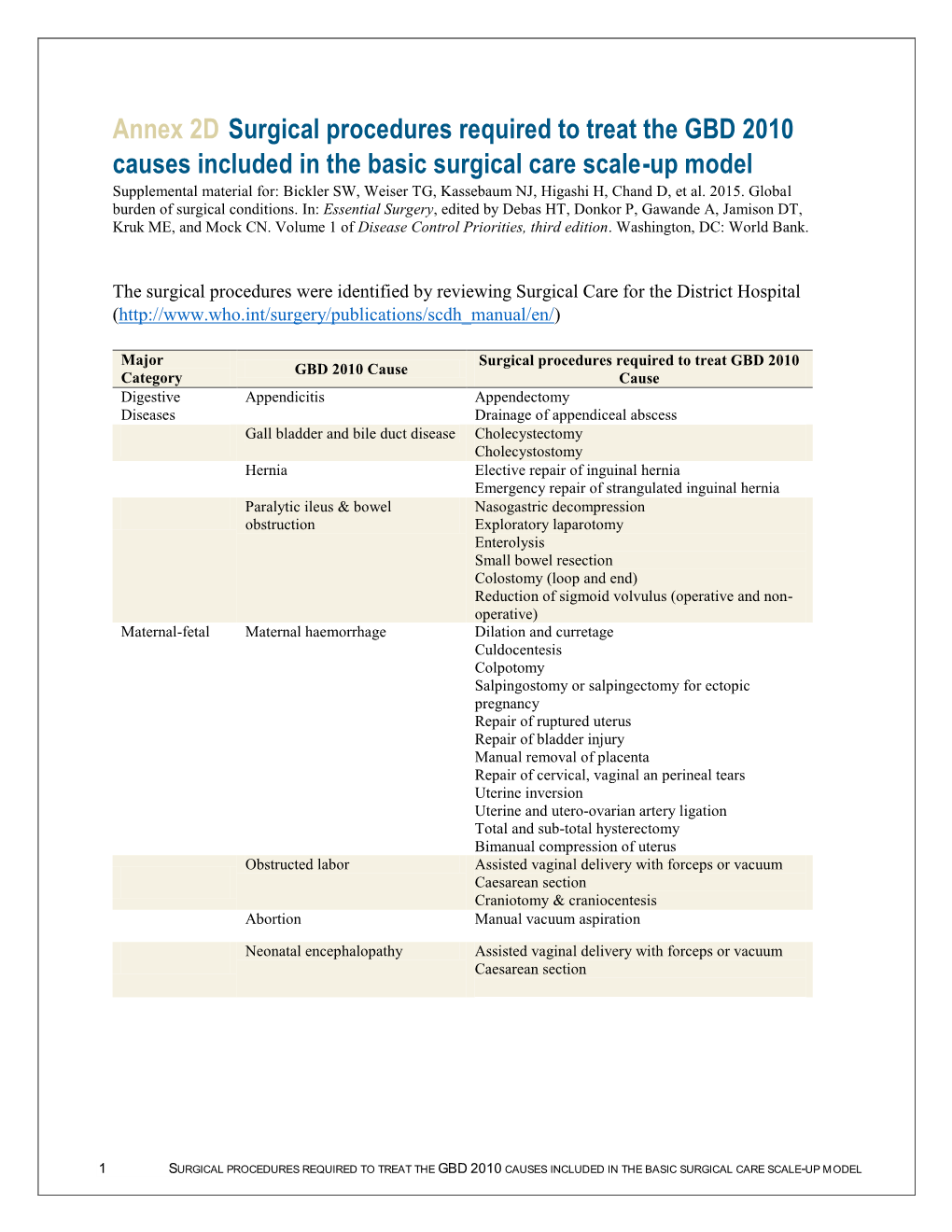
Surgical Procedures Required to Treat the GBD 2010 Causes Included In
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Canadian Surgery Forum Canadien De Chirurgie
Vol. 44, Suppl., August / août 2001 ISSN 0008-428X ABSTRACTS RÉSUMÉS of presentations to the des communications présentées Annual Meetings of the aux congrès annuels de la Canadian Society of Colon Société canadienne and Rectal Surgeons des chirurgiens du côlon et du rectum Canadian Association of General Surgeons Association canadienne des chirurgiens généraux Canadian Association of Thoracic Surgeons Association canadienne des chirurgiens thoraciques CANADIAN SURGERY FORUM CANADIEN DE CHIRURGIE Québec, QC September 6 to 9, 2001 Québec (QC) du 6 au 9 septembre 2001 Abstracts Résumés Canadian Surgery Forum canadien de chirurgie 2001 Canadian Society of Colon and Rectal Surgeons Société canadienne des chirurgiens du côlon et du rectum 1 2 ARTIFICIAL BOWEL SPHINCTER IMPLANTATION COMPARISON OF DELORME AND ALTEMEIER IN THE MANAGEMENT OF SEVERE FECAL IN- PROCEDURES FOR RECTAL PROLAPSE. E.C. McKe- CONTINENCE — EXPERIENCE FROM A SINGLE vitt, B.J. Sullivan, P.T. Phang. Department of Surgery, St. INSTITUTION. A.R. MacLean, G. Stewart, K. Sabr, M. Paul’s Hospital, University of British Columbia, Vancou- Burnstein. Department of Surgery, St Michael’s Hospital, ver, BC University of Toronto, Toronto, Ont. We wish to compare the outcomes of 2 perineal operations for The purpose of this study was to evaluate the safety and effi- rectal prolapse: rectal mucosectomy (Delorme’s operation) cacy of artificial bowel sphincter (ABS) implantation in the and perineal rectosigmoidectomy (Altemeier’s operation). management of severe fecal incontinence (FI). We reviewed all 34 patients who had a perineal repair of Ten patients (6 males), with a mean age of 40.6 years, un- rectal prolapse at our hospital from July 1997 to June 2000. -

The Efficacy of Preoperative Percutaneous Cholecystostomy for Acute Cholecystitis with Gallbladder Perforation 담낭천공을 동반한 급성담낭염 환자에서 수술 전 경피적담낭배액술의 효용성에 관한 연구
Original Article pISSN 1738-2637 / eISSN 2288-2928 J Korean Soc Radiol 2017;77(6):372-381 https://doi.org/10.3348/jksr.2017.77.6.372 The Efficacy of Preoperative Percutaneous Cholecystostomy for Acute Cholecystitis with Gallbladder Perforation 담낭천공을 동반한 급성담낭염 환자에서 수술 전 경피적담낭배액술의 효용성에 관한 연구 Bo Ra Kim, MD, Jeong-Hyun Jo, MD, Byeong-Ho Park, MD* Department of Radiology, Dong-A University Hospital, Dong-A University College of Medicine, Busan, Korea Purpose: Treatment of acute cholecystitis with gallbladder perforation remains Index terms controversial. We aimed to determine the feasibility of percutaneous cholecystosto- Cholecystostomy my (PC) in these patients. Cholecystitis, Acute Materials and Methods: We retrospectively reviewed patients who had acute Cholecystectomy cholecystitis with gallbladder perforation at a single institution. Group 1 (n = 27; M:F = 18:9; mean age, 69.9 years) consisted of patients who received PC followed Received May 12, 2017 by cholecystectomy, and group 2 (n = 16; M:F = 8:8; mean age 57.1 years) consisted Revised June 3, 2017 of patients who were treated with cholecystectomy only. Preoperative details, in- Accepted June 26, 2017 cluding sex, age, underlying medical history, signs of systemic inflammatory re- *Corresponding author: Byeong-Ho Park, MD Department of Radiology, Dong-A University Hospital, sponse syndrome (SIRS), laboratory findings, body mass index, presence of gallstone, Dong-A University College of Medicine, 26 Daesingong- and type of perforation; treatment-related variables, including laparoscopic or open won-ro, Seo-gu, Busan 49201, Korea. cholecystectomy, conversion to laparotomy, blood loss, surgical time and anesthesia Tel. 82-51-240-5371 Fax. -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

1 Annex 2. AHRQ ICD-9 Procedure Codes 0044 PROC-VESSEL
Annex 2. AHRQ ICD-9 Procedure Codes 0044 PROC-VESSEL BIFURCATION OCT06- 0201 LINEAR CRANIECTOMY 0050 IMPL CRT PACEMAKER SYS 0202 ELEVATE SKULL FX FRAGMNT 0051 IMPL CRT DEFIBRILLAT SYS 0203 SKULL FLAP FORMATION 0052 IMP/REP LEAD LF VEN SYS 0204 BONE GRAFT TO SKULL 0053 IMP/REP CRT PACEMAKR GEN 0205 SKULL PLATE INSERTION 0054 IMP/REP CRT DEFIB GENAT 0206 CRANIAL OSTEOPLASTY NEC 0056 INS/REP IMPL SENSOR LEAD OCT06- 0207 SKULL PLATE REMOVAL 0057 IMP/REP SUBCUE CARD DEV OCT06- 0211 SIMPLE SUTURE OF DURA 0061 PERC ANGIO PRECEREB VES (OCT 04) 0212 BRAIN MENINGE REPAIR NEC 0062 PERC ANGIO INTRACRAN VES (OCT 04) 0213 MENINGE VESSEL LIGATION 0066 PTCA OR CORONARY ATHER OCT05- 0214 CHOROID PLEXECTOMY 0070 REV HIP REPL-ACETAB/FEM OCT05- 022 VENTRICULOSTOMY 0071 REV HIP REPL-ACETAB COMP OCT05- 0231 VENTRICL SHUNT-HEAD/NECK 0072 REV HIP REPL-FEM COMP OCT05- 0232 VENTRI SHUNT-CIRCULA SYS 0073 REV HIP REPL-LINER/HEAD OCT05- 0233 VENTRICL SHUNT-THORAX 0074 HIP REPL SURF-METAL/POLY OCT05- 0234 VENTRICL SHUNT-ABDOMEN 0075 HIP REP SURF-METAL/METAL OCT05- 0235 VENTRI SHUNT-UNINARY SYS 0076 HIP REP SURF-CERMC/CERMC OCT05- 0239 OTHER VENTRICULAR SHUNT 0077 HIP REPL SURF-CERMC/POLY OCT06- 0242 REPLACE VENTRICLE SHUNT 0080 REV KNEE REPLACEMT-TOTAL OCT05- 0243 REMOVE VENTRICLE SHUNT 0081 REV KNEE REPL-TIBIA COMP OCT05- 0291 LYSIS CORTICAL ADHESION 0082 REV KNEE REPL-FEMUR COMP OCT05- 0292 BRAIN REPAIR 0083 REV KNEE REPLACE-PATELLA OCT05- 0293 IMPLANT BRAIN STIMULATOR 0084 REV KNEE REPL-TIBIA LIN OCT05- 0294 INSERT/REPLAC SKULL TONG 0085 RESRF HIPTOTAL-ACET/FEM -

COMPLICATIONS of Bile Duct Recon
Biliary Tract Complications in Liver Transplantation Under Cyclosporin-Steroid Therapy S. Iwatsuki, B. W. Shaw, Jr., and T. E. Starzl OMPLICATIONS of bile duct recon tube (usually infant feeding tube) was used as a stent. one C struction in liver transplantation are end passing through the papilla of Vater into the duode num (choledocho-choledochostomy with straight tube more frequent than those of vascular anasto stent. C-C-S), moses.I. 2 In earlier times, unrecognized bile End-to-side choledocho-jejunostomy in Roux-en-Y duct obstruction was frequently mistaken for with a straight tube stent (C-J-S) became the first choice graft rejection, and unwise decisions to when the recipient's bile duct was absent (in biliary increase immunosuppression often resulted in atresia) or diseased (in sclerosing cholangitis. bile duct cancer. or secondary biliary cirrhosis). When the donor's fatal septic complications. In other cases, bil common bile duct was used for bile duct reconstruction. iary leakage and peritonitis in the early post the gallbladder was always removed, operative period limited the adequate use of Cholecysto-jejunostomy in Roux-en-Y (Cy-J). tube immunosuppression, resulting in acute graft cholecystostomy. or tube choledochostomy were used only rejection superimposed on serious septic bil when the operation was so difficult and the patient was so unstable that better bile duct reconstruction could not be iary peritonitis. performed. The problems caused by biliary complica tions under conventional immunosuppression Case Materials have been reported in our series I and in the During the 29 months between March 1980 and July Cambridge series.2 These, directly or indirect 1982.78 patients received 90 orthotopic liver transplanta ly, caused death in many cases. -

A Clinical Study of Intestinal Stomas in Emergency Laparotomies
Crimson Publishers Research Article Wings to the Research A Clinical Study of Intestinal Stomas in Emergency Laparotomies Rovena Bode1*, Virna Zyka2, Lorenc Bode2 and Hysni Dede2 1Department of Surgery, Albania 2Faculty of Medicine, Albania Abstract ISSN: 2578-0093 Background: Intestinal stomas are used to divert the fecal stream away from distal bowel in order to allow a distal anastomosis to heal as well as to relieve obstruction in emergency situation. The aim of the present study was to identify indications for emergency laparotomy, commonly performed intestinal stomas and to study complications related to it. Methods: This is a retrospective study and was carried out in the surgical unit of Mother Teresa University Hospital Center, from January 2017 to August 2018. All patients were admitted through emergency and underwent surgery for various reasons and were followed up to note any complication which resulted in theResults: creation The of most intestinal common stomas, indication and who for fit stoma in to inclusionformation criteria. was colorectal carcinoma (n=77) followed by sigmoid volvulus (n=16), perforated sigmoid diverticula (n=12), recto-sigmoid perforation by corpus alienum (n=6). A total of 106 patients underwent colostomy formation, of which 85 were end colostomy and 21 were Baguette colostomy. Thirty-one (31) patients underwent ileostomy formation, of which 9 were loop ileostomy and 10 were temporary end ileostomy, one was double barrel ileostomy. Nine (9) *Corresponding author: Rovena Bode, cases were treated with jejunostomy and 5 cases with duodenostomy. Department of Surgery, Albania Conclusion: Fecal/intestinal diversion remains an effective option to treat a variety of gastrointestinal Submission: August 02, 2019 and abdominal conditions. -

Effective Use of Percutaneous Cholecystostomy in High-Risk Surgical Patients Techniques, Tube Management, and Results
PAPER Effective Use of Percutaneous Cholecystostomy in High-Risk Surgical Patients Techniques, Tube Management, and Results Clark A. Davis, MD; Jeffrey Landercasper, MD; Lincoln H. Gundersen, MD; Pamela J. Lambert, RN Hypothesis: Percutaneous cholecystostomy (PC) is an cal findings. All patients received antibiotics prior to PC effective, safe treatment in patients with suspected acute for 24 or more hours. Thirty-day mortality was 36% (8 cholecystitis and severe concomitant comorbidity. patients), reflecting severity of concomitant disease. Mi- nor complications occurred in 3 of 22 patients. Clinical Design: Retrospective medical record review from March improvement occurred in 18 (82%) of 22 patients—15 1989 to March 1998. (68%) within 48 hours. Follow-up of fourteen 30-day sur- vivors is as follows: 7 (50%) had drains removed be- Setting: Referral community teaching hospital (450 beds) cause the gallbladder was stone free, 4 (29%) had drains in rural Wisconsin. remaining due to persistent stones, 2 (14%) underwent cholecystectomy, and 1 (7%) awaits scheduled surgery. Patients: Twenty-two consecutive patients underwent Only 1 (12.5%) of 8 patients developed biliary compli- PC tube placement over a 10-year period. Twenty pro- cations after drain removal, requiring endoscopic retro- cedures were for acute cholecystitis (14 calculous, 6 acal- grade cholangiopancreatography 9 months after drain re- culous) and 2 were for diagnostic dilemmas. Nineteen moval. One patient required urgent cholecystectomy after (86%) of 22 patients were American Society of Anesthe- failure to respond to PC. This patient died of a periop- siologists class 4; 3 (14%) were class 3. erative myocardial infarction. Interventions: Pigtail catheters (8F-10F) placed by Conclusions: Percutaneous cholecystostomy is an ef- means of ultrasound or computed tomographic localiza- fective, safe treatment in patients with suspected acute tion, with or without fluoroscopic adjunct. -

Physician Service Fee Schedule
REPORT: RS04328‐R1328 NORTH CAROLINA DEPARTMENT OF HEALTH AND HUMAN SERVICES PHYSICIAN FEE SCHEDULE AS OF:9/19/2019 Physician Fee Schedule Provider Specialty 001 Fee Schedule Updated on: 9/19/2019 ***The Agency's fee schedule rates below were set as of January 1, 2014 unless otherwise noted*** Rate changes after January 1, 2014 are based on the January 1st RVU of the year in which the service was initally established The inclusion of a rate on this table does not guarantee that a service is covered. Please refer to the Medicaid Billing Guide and the Medicaid and Health Choice Clinical Policies on the DHB Web Site. Providers should always bill their usual and customary charges. Please use the monthly NC Medicaid Bulletins for additions, changes and deletion to this schedule. Medicaid Maximum Allowable NON-FACILITY Effective Date PROCEDURE CODE MODIFIER PROCEDURE DESCRIPTION FACILITY RATE RATE of Rate 10004 FNA BX W/O IMG GDN EA ADDL $ 36.98 $ 43.90 2019-01-01 10005 FNA BX W/US GDN 1ST LES $ 62.62 $ 105.61 2019-01-01 10006 FNA BX W/US GDN EA ADDL $ 42.67 $ 50.75 2019-01-01 10007 FNA BX W/FLUOR GDN 1ST LES $ 80.39 $ 235.92 2019-01-01 10008 FNA BX W/FLUOR GDN EA ADDL $ 52.43 $ 133.22 2019-01-01 10009 FNA BX W/CT GDN 1ST LES $ 97.58 $ 385.27 2019-01-01 10010 FNA BX W/CT GDN EA ADDL $ 71.32 $ 232.62 2019-01-01 11102 TANGNTL BX SKIN SINGLE LES $ 33.65 $ 81.55 2019-01-01 11103 TANGNTL BX SKIN EA SEP/ADDL $ 19.49 $ 44.02 2019-01-01 11104 PUNCH BX SKIN SINGLE LESION $ 42.23 $ 102.54 2019-01-01 Printed 9/19/2019 Page 1 of 330 REPORT: RS04328‐R1328 -

General Surgery
Database of questions for the Medical Final Examination (LEK) General surgery Question nr 1 Which of the following operations can be performed in the case of adenocarcinoma localized in the sigmoid colon? A. laparoscopic sigmoid resection. B. Hartmann’s procedure by means of laparotomy. C. sigmoid resection by means of laparotomy. D. laparoscopic Hartmann operation. E. all the above. Question nr 2 The patient in poor general condition was transported to the hospital admission room. He reports a retrosternal pain and high fever. On the physical examination the crackling of the skin was palpable around the neck. The patient had been diagnosed with advanced oesophageal cancer. The chest CT showed the presence of air in the mediastinum, contrast leakage in the thoracic section of the esophagus and fluid effusion in the right pleural cavity. Indicate the optimal surgical procedures in this case: A. a gastric probe, a ban on oral nutrition, antibiotic therapy. B. stitching the oesophagus with an access via right-sided thoracotomy. C. exclusion of the oesophagus through the emergence of oesophagostomy on the neck, mediastinal drainage, occlusion of the gastric gullet, further nutrition by nutritional gastrostomy. D. oesophageal resection with gastroesophageal anastomosis in the cage chest. E. implantation of a self-expanding stent with optional drainage of the right pleural cavity. Question nr 3 Which of the following can be classified as the grade II according to Hinchey classification of complications caused by diverticulitis? A. diverticulitis with para-colonic abscess. B. diverticulitis with pelvic abscess. C. diverticulitis with purulent peritonitis. D. diverticulitis with feculent peritonitis. E. Hinchey classification is not related to diverticulitis. -

General Rate Provisions 16.04: Maximum Allowable Fees - Anesthesia Services 16.05: Maximum Allowable Fees - Surgical Services 16.06 Severability
Adopted Regulation August 31, 2012 114.3 CMR: DIVISION OF HEALTH CARE FINANCE AND POLICY AMBULATORY CARE 114.3 CMR 16.00: SURGERY AND ANESTHESIA SERVICES Section 16.01: General Provisions 16.02: General Definitions 16.03: General Rate Provisions 16.04: Maximum Allowable Fees - Anesthesia Services 16.05: Maximum Allowable Fees - Surgical Services 16.06 Severability 16.01: General Provisions (1) Scope, Purpose and Effective Date. (a) 114.3 CMR 16.00 governs the payment rates used by all governmental units for surgery and anesthesia services provided to publicly aided patients. 114.3 CMR 16.00 is effective July 1, 2012. Rates for services provided to individuals covered by M.G.L. c. 152 (the Workers' Compensation Act) are set forth at 114.3 CMR 40.00. (b) The following laboratory services have a professional and technical component. These are codes: 83020, 83912, 84165, 84166, 84181, 84182, 85390, 85576, 86255, 86256, 86320, 86325, 86327, 86334, 86335, 87164, 87207, 88371, 88372 and 89060. The professional component is contained herein. The technical component for these codes is contained in 114.3 CMR 20.00 Clinical Laboratory Services. (2) Coverage. The payment rates in 114.3 CMR 16.00 are used to pay for: (a) Surgical and anesthesia services rendered to registered bed patients in a licensed health care facility by an eligible provider who is not under contractual arrangement with the licensed health care facility for medical services and who bills separately and apart from the health care facility for medical services rendered. (b) Surgical and anesthesia services rendered to ambulatory patients in a private medical office, freestanding ambulatory surgical center, licensed clinic facility, hospital outpatient department, independent diagnostic testing facility, or other appropriate setting by an eligible provider who bills for the medical services rendered and receives no other compensation for medical services rendered. -

Percutaneous Cholecystostomy-Tube for High-Risk Patients with Acute Cholecystitis: Current Practice and Implications for Future Research
Surgical Endoscopy (2019) 33:3396–3403 and Other Interventional Techniques https://doi.org/10.1007/s00464-018-06634-5 Percutaneous cholecystostomy-tube for high-risk patients with acute cholecystitis: current practice and implications for future research Ravi B. Pavurala1 · Daniel Li1 · Kyle Porter2 · Sara A. Mansfield3 · Darwin L. Conwell4 · Somashekar G. Krishna4 Received: 13 June 2018 / Accepted: 19 December 2018 / Published online: 2 January 2019 © Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Background While cholecystectomy (CCY) is the standard of care for gallstone-related acute cholecystitis, percutaneous cholecystostomy-tube (CCYT-tube) is an alternative option in patients with significant comorbid conditions. We sought to identify immediate and longitudinal hospital outcomes of patients who underwent CCYT-tube placement and determine predictors of CCYT-tube placement and eventual CCY on a national level in the US. Methods We identified all adults (age ≥ 18 years) with a primary diagnosis of acute calculous cholecystitis from January to November 2013 in the Nationwide Readmissions Database (NRD). The NRD allows longitudinal follow-up of a patient for one calendar year. Outcomes of patients undergoing CCY and CCYT-tube were compared. Separate univariable and multivariable regression analyses were performed to identify predictors of CCYT-tube placement and failure to undergo subsequent CCY. Results A total of 181,262 patients had an index hospitalization with acute cholecystitis where 178,095 (98.3%) patients underwent only CCY and 3167 (1.7%) patients were managed with CCYT-tubes. Among patients with CCYT-tube, 1196 (37.8%) underwent eventual CCY in 2013, while 1971 (62.2%) did not. -

Hemorrhagic Cholecystitis in a Patient with Cirrhosis and Rectal Cancer
Open Access Case Report DOI: 10.7759/cureus.7882 Hemorrhagic Cholecystitis in a Patient with Cirrhosis and Rectal Cancer Rony Shah 1 , Linda C. Klumpp 1 , James Craig 1 , Parth Patel 2 , Jeffrey Jordan 1 1. Internal Medicine, Citrus Memorial Hospital, Inverness, USA 2. Surgery, Citrus Memorial Hospital, Inverness, USA Corresponding author: Rony Shah, [email protected] Abstract Hemorrhagic cholecystitis is a rare presentation of acute calculous cholecystitis which presents with abdominal pain, jaundice, and gastrointestinal bleeding. It is a challenging diagnosis to make because it present similar to other common disorders such as calculous cholecystitis. We present a unique case of hemorrhagic cholecystitis in a patient with cirrhosis and rectal cancer. A 66-year-old male with a history of rectal cancer, alcohol-induced cirrhosis, esophageal varices, stroke, paroxysmal atrial fibrillation, and hypertension presented to the emergency department with complaints of abdominal pain. Patient’s computed tomography (CT) scan revealed bleeding from the gallbladder with hemoperitoneum and thickening of the ascending colon. The patient underwent emergent surgery for hemorrhagic cholecystitis. Hemorrhagic cholecystitis is associated with risk factors, including trauma, malignancy, renal failure, cirrhosis, and anticoagulation therapy. Imaging is not always reliable, but ultrasound and CT scan are the preferred options. Treatment options are surgical or nonsurgical approach depending on patient’s hemodynamic stability. Categories: Internal Medicine, Gastroenterology, General Surgery Keywords: cholecystitis, hemorrhagic cholecystitis, hemoperitoneum, cirrhosis, rectal cancer Introduction Hemorrhagic cholecystitis is a life-threatening complication of acute calculous cholecystitis. A hemorrhage within the gallbladder can occur for a variety of reasons, such as obstructive cholecystitis, biliary neoplasm, biliary parasites, bleeding disorder, percutaneous intervention, and trauma [1].