Exonic Deletions in AUTS2 Cause a Syndromic Form of Intellectual Disability and Suggest a Critical Role for the C Terminus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Fast-Evolving Gene Is Key Player in Brain Development
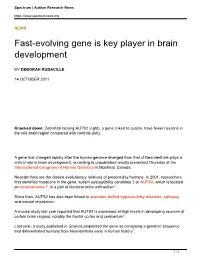
Spectrum | Autism Research News https://www.spectrumnews.org NEWS Fast-evolving gene is key player in brain development BY DEBORAH RUDACILLE 14 OCTOBER 2011 Knocked down: Zebrafish lacking AUTS2 (right), a gene linked to autism, have fewer neurons in the mid-brain region compared with controls (left). A gene that changed rapidly after the human genome diverged from that of Neanderthals plays a critical role in brain development, according to unpublished results presented Thursday at the International Congress of Human Genetics in Montreal, Canada. Neanderthals are the closest evolutionary relatives of present-day humans. In 2001, researchers first identified mutations in the gene, autism susceptibility candidate 2 or AUTS2, which is located on chromosome 7, in a pair of identical twins with autism1. Since then, AUTS2 has also been linked to attention deficit hyperactivity disorder, epilepsy and mental retardation. A mouse study last year reported that AUTS2 is expressed at high levels in developing neurons of certain brain regions, notably the frontal cortex and cerebellum2. Last year, a study published in Science pinpointed the gene as containing a genomic sequence that differentiated humans from Neanderthals early in human history3. 1 / 3 Spectrum | Autism Research News https://www.spectrumnews.org Still, the function of AUTS2 has remained elusive until now. Researchers at the University of California, San Francisco presented the first functional study of the gene, which they identified while searching for genes important in development. “We were looking for regions in the genome that have a lot of evolutionary conservation, which usually indicates an important developmental gene that needs tight regulation,” says lead investigator Nadav Ahituv, assistant professor of bioengineering and therapeutic sciences at the University of California, San Francisco. -

A Low‐Grade Astrocytoma in a Sixteen‐Year‐Old Boy with a 7Q11.22 Deletion
CASE REPORT A low-grade astrocytoma in a sixteen-year-old boy with a 7q11.22 deletion Francoise S. van Kampen1 , Marianne E. Doornbos1, Monique A. van Rijn2 & Yolande den Bever3 1Department of Paediatrics, Albert Schweitzer Hospital, Dordrecht, The Netherlands 2Department of Neurology, Albert Schweitzer Hospital, Dordrecht, The Netherlands 3Department of Clinical Genetics, Erasmus University Hospital, Rotterdam, The Netherlands Correspondence Key Clinical Message Franciscus Vlietland Group Vlietlandplein 2 Postbus 215 3100 AE Schiedam We report a patient with developmental delay due to germline AUTS2 muta- Tel: (0031)108939393 tion who developed a low-grade astrocytoma. While the contribution of this E-mail: [email protected] mutation to the pathogenesis of the tumor is not known at this time, a role of AUTS2 in deregulation of PRC1 can be a part in tumorigenesis of a brain tumor. Funding Information No sources of funding were declared for this study. Keywords AUTS2, brain tumor, neurologic, pediatric. Received: 29 October 2016; Revised: 26 October 2017; Accepted: 13 November 2017 Clinical Case Reports 2018; 6(2): 274–277 doi: 10.1002/ccr3.1312 Background drives the formation of most low-grade gliomas (LGG). The most common mechanism of a MAPK pathway acti- In this case report, we describe a first patient with a low- vation in LGG’s is a tandem duplication on chromosome grade astrocytoma and a deletion in the AUTS2 gene. 7q34. In addition, deletions in 7q34 are described [4]. Mutations in (parts of) the autism susceptibility candidate Astrocytomas are occasionally described in Noonan, 2 (AUTS2) are described in case reports and further Turner, Lynch syndrome, and neurofibromatosis. -
Genomic Divergence and Brain Evolution: How Regulatory DNA Influences Development of the Cerebral Cortex
Prospects & Overviews Review essays Genomic divergence and brain evolution: How regulatory DNA influences development of the cerebral cortex Debra L. Silver1)2)3)4) The cerebral cortex controls our most distinguishing higher Introduction cognitive functions. Human-specific gene expression dif- ferences are abundant in the cerebral cortex, yet we have A large six-layered neocortex is a unique feature of only begun to understand how these variations impact brain mammalian brains. This specialized outer covering of the brain controls our higher cognitive functions including function. This review discusses the current evidence linking abstract thought and language, which together help uniquely non-coding regulatory DNA changes, including enhancers, define us as humans. Our distinguishing cognitive capacities with neocortical evolution. Functional interrogation using are specified within discrete cortical areas and are driven by animal models reveals converging roles for our genome in dynamic communication between neurons of the neocortex key aspects of cortical development including progenitor and other brain regions, as well as glial cell populations (including oligodendrocytes, microglia, and astrocytes). cell cycle and neuronal signaling. New technologies, Neurons are initially generated during human embryonic includingiPS cells and organoids, offerpotential alternatives and early fetal development, where they migrate to appropri- to modeling evolutionary modifications in a relevant species ate regions and begin establishing functional connections context. Several diseases rooted in the cerebral cortex during fetal and postnatal stages (Fig. 1). Disruptions to uniquely manifest in humans compared to other primates, cerebral cortex function arising during either development or thus highlighting the importance of understanding human adulthood, can result in neurodevelopmental and neurode- generative disorders. -

Shallow Whole Genome Sequencing On
Author Manuscript Published OnlineFirst on July 14, 2017; DOI: 10.1158/1078-0432.CCR-17-0675 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Shallow whole genome sequencing on circulating cell-free DNA allows reliable non- invasive copy number profiling in neuroblastoma patients Nadine Van Roy1,4, Malaïka Van Der Linden1,3, Björn Menten1, Annelies Dheedene1, Charlotte Vandeputte 1,4, Jo Van Dorpe3, Geneviève Laureys2,4, Marleen Renard5, Tom Sante1,Tim Lammens2,4, Bram De Wilde2,4, Frank Speleman1,4, Katleen De Preter1,4,* 1Center for Medical Genetics, Ghent University, Ghent, Belgium 2Department of Pediatric Hematology-Oncology and Stem Cell Transplantation, Ghent University Hospital, Ghent, Belgium 3Department of Pathology, Ghent University, Ghent, Belgium 4Cancer Research Institute Ghent, Ghent University, Ghent, Belgium 5Department of Pediatric Hematology-Oncology and Stem Cell Transplantation, Leuven University Hospital, Leuven, Belgium *Corresponding author Running title: non-invasive copy number profiling using shallow WGS Keywords: neuroblastoma, cell-free DNA, copy number profiling, shallow whole genome sequencing, non-invasive The authors would like to thank the following funding agencies: the Belgian Foundation against Cancer (project 2015-146) to FS, the Flemish liga against cancer (B/14651/01 and STIVLK2016000601), Ghent University (BOF16/GOA/23) to FS, the Belgian Program of Interuniversity Poles of Attraction (IUAP Phase VII - P7/03) to FS, the Fund for Scientific Research Flanders (Research project G021415N) to KDP and project 18B1716N to BDW, the European Union H2020 (OPTIMIZE-NB GOD9415N and TRANSCAN-ON THE TRAC GOD8815N) to FS. The Ghent University Hospital innovation project for molecular pathology (project number: KW/1694/PAN/001/001) to JVD and MVDL, vzw Kinderkankerfonds, a non-profit childhood cancer foundation under Belgian law to TL. -

Diapositivo 1
Silvia Serafim*; Barbara Marques*; Filomena Brito*; Sonia Pedro*; Cristina Ferreira*; Catarina Ventura*; Isabel Gaspar**; Hildeberto Correia* *Unidade de Citogenetica, Instituto Nacional de Saude Doutor Ricardo Jorge, I.P., Lisboa, Portugal **Consulta de Genetica Medica, Hospital Egas Moniz, Centro Hospitalar de Lisboa Ocidental EPE, Lisboa, Portugal Introduction Chromosome Microarray Analysis is a powerful diagnostic tool and is being used as a first-line approach to detect chromosome imbalances associated with intellectual disability, dysmorphic features and congenital anomalies. This test enables the identification of new copy number variants (CNVs) and their association with new microdeletion/microduplication syndromes in patients previously studied by conventional cytogenetics analysis. Here we report the case of a female with severe intellectual disability, absence of speech, microcephaly and congenital abnormalities with a previous normal karyotype performed at a younger age. Microarray analysis was performed at 17 years of age, in order to assess if a genome unbalance could explain the patient’s undiagnosed phenotype. A small deletion was found in autism susceptibility candidate 2 (AUTS2) gene . The AUTS2 gene has been recently implicated in autosomal dominant mental retardation with variable syndromic phenotype (OMIM *607270, #615834). Common clinical features described in patients with deletions in AUTS2 gene include autism, intellectual disability, speech delay and microcephaly, among others (1,2,3,4,5,6). We compare our patient with similar reported cases, adding additional value to the phenotype-genotype correlation of CNVs in this region. Method Microarray analysis was carried out in DNA extracted from peripheral blood using Affymetrix CytoScan HD chromosome microarray platform according to the manufacturer’s recommendations. -

Transcriptional Landscape of B Cell Precursor Acute Lymphoblastic Leukemia Based on an International Study of 1,223 Cases
Transcriptional landscape of B cell precursor acute lymphoblastic leukemia based on an international study of 1,223 cases Jian-Feng Lia,1, Yu-Ting Daia,1, Henrik Lilljebjörnb,1, Shu-Hong Shenc, Bo-Wen Cuia, Ling Baia, Yuan-Fang Liua, Mao-Xiang Qiand, Yasuo Kubotae, Hitoshi Kiyoif, Itaru Matsumurag, Yasushi Miyazakih, Linda Olssonb, Ah Moy Tani, Hany Ariffinj, Jing Chenc, Junko Takitak, Takahiko Yasudal, Hiroyuki Manom, Bertil Johanssonb,n, Jun J. Yangd,o, Allen Eng-Juh Yeohp, Fumihiko Hayakawaq, Zhu Chena,r,s,2, Ching-Hon Puio,2, Thoas Fioretosb,n,2, Sai-Juan Chena,r,s,2, and Jin-Yan Huanga,s,2 aState Key Laboratory of Medical Genomics, Shanghai Institute of Hematology, National Research Center for Translational Medicine, Rui-Jin Hospital, Shanghai Jiao Tong University School of Medicine and School of Life Sciences and Biotechnology, Shanghai Jiao Tong University, 200025 Shanghai, China; bDepartment of Laboratory Medicine, Division of Clinical Genetics, Lund University, 22184 Lund, Sweden; cKey Laboratory of Pediatric Hematology and Oncology, Ministry of Health, Department of Hematology and Oncology, Shanghai Children’s Medical Center, Shanghai Jiao Tong University School of Medicine, 200127 Shanghai, China; dDepartment of Pharmaceutical Sciences, St. Jude Children’s Research Hospital, Memphis, TN 38105; eDepartment of Pediatrics, Graduate School of Medicine, The University of Tokyo, 1138654 Tokyo, Japan; fDepartment of Hematology and Oncology, Nagoya University Graduate School of Medicine, 4668550 Nagoya, Japan; gDivision of Hematology -

Function and Regulation of AUTS2, a Gene Implicated in Autism and Human Evolution
Function and Regulation of AUTS2, a Gene Implicated in Autism and Human Evolution Nir Oksenberg1,2, Laurie Stevison2, Jeffrey D. Wall2,3, Nadav Ahituv1,2* 1 Department of Bioengineering and Therapeutic Sciences, University of California San Francisco, San Francisco, California, United States of America, 2 Institute for Human Genetics, University of California San Francisco, San Francisco, California, United States of America, 3 Department of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California, United States of America Abstract Nucleotide changes in the AUTS2 locus, some of which affect only noncoding regions, are associated with autism and other neurological disorders, including attention deficit hyperactivity disorder, epilepsy, dyslexia, motor delay, language delay, visual impairment, microcephaly, and alcohol consumption. In addition, AUTS2 contains the most significantly accelerated genomic region differentiating humans from Neanderthals, which is primarily composed of noncoding variants. However, the function and regulation of this gene remain largely unknown. To characterize auts2 function, we knocked it down in zebrafish, leading to a smaller head size, neuronal reduction, and decreased mobility. To characterize AUTS2 regulatory elements, we tested sequences for enhancer activity in zebrafish and mice. We identified 23 functional zebrafish enhancers, 10 of which were active in the brain. Our mouse enhancer assays characterized three mouse brain enhancers that overlap an ASD–associated deletion and four mouse enhancers that reside in regions implicated in human evolution, two of which are active in the brain. Combined, our results show that AUTS2 is important for neurodevelopment and expose candidate enhancer sequences in which nucleotide variation could lead to neurological disease and human-specific traits. -

Whole Exome Sequencing Reveals a Novel AUTS2 In-Frame Deletion in a Boy with Global Developmental Delay, Absent Speech, Dysmorphic Features, and Cerebral Anomalies
G C A T T A C G G C A T genes Case Report Whole Exome Sequencing Reveals a Novel AUTS2 In-Frame Deletion in a Boy with Global Developmental Delay, Absent Speech, Dysmorphic Features, and Cerebral Anomalies Pietro Palumbo 1 , Ester Di Muro 1, Maria Accadia 2, Mario Benvenuto 1, Marilena Carmela Di Giacomo 3, Stefano Castellana 4, Tommaso Mazza 4 , Marco Castori 1, Orazio Palumbo 1,* and Massimo Carella 1 1 Division of Medical Genetics, Fondazione IRCCS-Casa Sollievo della Sofferenza, 71013 San Giovanni Rotondo (Foggia), Italy; [email protected] (P.P.); [email protected] (E.D.M.); [email protected] (M.B.); [email protected] (M.C.); [email protected] (M.C.) 2 Medical Genetics Service, Hospital “Cardinale G. Panico”, 73039 Tricase (Lecce), Italy; [email protected] 3 U.O.C di Anatomia Patologica, AOR Ospedale “San Carlo”, 85100 Potenza, Italy; [email protected] 4 Unit of Bioinformatics, Fondazione IRCCS Casa Sollievo della Sofferenza, 71013 San Giovanni Rotondo (Foggia), Italy; [email protected] (S.C.); [email protected] (T.M.) * Correspondence: [email protected] Abstract: Neurodevelopmental disorders (NDDs) are a group of highly prevalent, clinically and genetically heterogeneous pediatric disorders comprising, according to the Diagnostic and Statisti- Citation: Palumbo, P.; Di Muro, E.; cal Manual of Mental Disorders 5th edition (DSM-V), intellectual disability, developmental delay, Accadia, M.; Benvenuto, M.; Di autism spectrum disorders, and other neurological and cognitive disorders manifesting in the de- Giacomo, M.C.; Castellana, S.; Mazza, velopmental age. To date, more than 1000 genes have been implicated in the etiopathogenesis of T.; Castori, M.; Palumbo, O.; Carella, NNDs. -

Epigenetic Regulator Genes Direct Lineage Switching in MLL-AF4
bioRxiv preprint doi: https://doi.org/10.1101/2021.07.16.452676; this version posted August 19, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Tirtakusuma et al. Lineage switching in MLL-AF4 leukaemias 1 Epigenetic regulator genes direct lineage switching in MLL-AF4 2 leukaemia 3 Ricky Tirtakusuma1, Katarzyna Szoltysek1,2,3, Paul Milne4, Vasily V Grinev5, Anetta 4 Ptasinska6, Claus Meyer7, Sirintra Nakjang1, Jayne Y Hehir-Kwa2, Daniel Williamson1, Pierre 5 Cauchy6, Salam A Assi6, Maria R Imperato6, Fotini Vogiatzi9, Shan Lin10, Mark Wunderlich10, 6 Janine Stutterheim2, Alexander Komkov8, Elena Zerkalenkova8, Paul Evans11, Hesta 7 McNeill1, Alex Elder1, Natalia Martinez-Soria1, Sarah E Fordham1, Yuzhe Shi1, Lisa J 8 Russell1, Deepali Pal1, Alex Smith12, Zoya Kingsbury13, Jennifer Becq13, Cornelia Eckert14, 9 Oskar A Haas15, Peter Carey16, Simon Bailey1,16, Roderick Skinner1,16, Natalia Miakova8, 10 Matthew Collin4, Venetia Bigley4, Muzlifah Haniffa17,18,19, Rolf Marschalek7, Christine J 11 Harrison1, Catherine A Cargo11, Denis Schewe9, Yulia Olshanskaya8, Michael J Thirman20, 12 Peter N Cockerill6, James C Mulloy10, Helen J Blair1, Josef Vormoor1,2, James M Allan1, 13 Constanze Bonifer6*, Olaf Heidenreich1,2*†, Simon Bomken1,16*† 14 Author Affiliations 15 1Wolfson Childhood Cancer Research Centre, Centre for Cancer, Translational and Clinical 16 Research Institute, Newcastle University, Newcastle upon Tyne, UK 17 2Princess Maxima Center for Pediatric Oncology, Utrecht, The Netherlands 18 3Maria Sklodowska-Curie Institute - Oncology Center, Gliwice Branch, Gliwice, Poland 19 4Translational and Clinical Research Institute, Newcastle University, Framlington Place, 20 Newcastle upon Tyne, UK 21 5Department of Genetics, the Faculty of Biology, Belarusian State University, 220030 Minsk, 22 Republic of Belarus. -

AUTS2 Controls Neuronal Lineage Choice Through a Novel PRC1-Independent Complex And
bioRxiv preprint doi: https://doi.org/10.1101/2021.06.29.450402; this version posted June 29, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. AUTS2 controls neuronal lineage choice through a novel PRC1-independent complex and BMP inhibition Zhuangzhuang Geng1, Qiang Wang1, Weili Miao2, Trevor Wolf3, Jessenia Chavez1, Emily Giddings3, Ryan Hobbs4, David J. DeGraff5,6, Yinsheng Wang2, James Stafford3, Zhonghua Gao1,6,7,# 1, Departments of Biochemistry and Molecular Biology, Penn State College of Medicine, Hershey, PA 17033, USA 2, Department of Chemistry, University of California at Riverside, Riverside, CA 92521, USA 3, Department of Neurological Sciences, Larner College of Medicine, University of Vermont, Burlington, VT 05405, USA 4, Department of Dermatology, Penn State College of Medicine, Hershey, PA 17033, USA 5, Department of Pathology and Laboratory Medicine, Penn State College of Medicine, Hershey, PA 17033, USA 6, Penn State Hershey Cancer Institute, Hershey, PA 17033, USA 7, The Stem Cell and Regenerative Biology Program, Penn State College of Medicine, Hershey, PA 17033, USA #, correspondence author, [email protected] bioRxiv preprint doi: https://doi.org/10.1101/2021.06.29.450402; this version posted June 29, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Summary Despite a prominent risk factor for Neurodevelopmental disorders (NDD), it remains unclear how Autism Susceptibility Candidate 2 (AUTS2) controls the neurodevelopmental program. Our studies investigated the role of AUTS2 in neuronal differentiation and discovered that AUTS2, together with WDR68 and SKI, forms a novel protein complex (AWS) specifically in neuronal progenitors and promotes neuronal differentiation through inhibiting BMP signaling. -

Six Novel Susceptibility Loci for Early-Onset Androgenetic Alopecia and Their Unexpected Association with Common Diseases
Six Novel Susceptibility Loci for Early-Onset Androgenetic Alopecia and Their Unexpected Association with Common Diseases Rui Li1., Felix F. Brockschmidt2,3., Amy K. Kiefer4., Hreinn Stefansson5., Dale R. Nyholt6., Kijoung Song7., Sita H. Vermeulen8,9., Stavroula Kanoni10., Daniel Glass11, Sarah E. Medland6, Maria Dimitriou12, Dawn Waterworth7, Joyce Y. Tung4, Frank Geller13, Stefanie Heilmann2,3, Axel M. Hillmer14, Veronique Bataille11, Sibylle Eigelshoven15, Sandra Hanneken15, Susanne Moebus16, Christine Herold17, Martin den Heijer18, Grant W. Montgomery6, Panos Deloukas10, Nicholas Eriksson4, Andrew C. Heath19, Tim Becker17,20, Patrick Sulem5, Massimo Mangino11, Peter Vollenweider21, Tim D. Spector11, George Dedoussis12", Nicholas G. Martin6", Lambertus A. Kiemeney8,22,23", Vincent Mooser7", Kari Stefansson5", David A. Hinds4", Markus M. No¨ then2,3,17", J. Brent Richards1,11"* 1 Departments of Medicine, Human Genetics, Epidemiology, and Biostatistics, Lady Davis Institute, Jewish General Hospital, McGill University, Montreal, Quebec, Canada, 2 Institute of Human Genetics, University of Bonn, Bonn, Germany, 3 Department of Genomics, Life and Brain Center, University of Bonn, Bonn, Germany, 4 23andMe, Mountain View, California, United States of America, 5 deCODE genetics, Reykjavı´k, Iceland, 6 Queensland Institute of Medical Research, Brisbane, Australia, 7 Genetics Division, GlaxoSmithKline, King of Prussia, Pennsylvania, United States of America, 8 Department of Epidemiology, Biostatistics, and HTA, Radboud University Nijmegen Medical -

Exploring the Genesis and Functions of Human Accelerated Regions
Available online at www.sciencedirect.com ScienceDirect Exploring the genesis and functions of Human Accelerated Regions sheds light on their role in human evolution 1 2 Melissa J Hubisz and Katherine S Pollard Human accelerated regions (HARs) are DNA sequences that divergent molecular or organism traits [7,8 ,9 ]. These changed very little throughout mammalian evolution, but then comparative genomic studies differ in their methodologi- experienced a burst of changes in humans since divergence cal details and the data sets employed, but they have a from chimpanzees. This unexpected evolutionary signature is common goal: to identify Human Accelerated Regions suggestive of deeply conserved function that was lost or (HARs), DNA sequences with dramatically increased changed on the human lineage. Since their discovery, the substitution rates in the human lineage. This lineage actual roles of HARs in human evolution have remained has generally been taken as the 6 million years since somewhat elusive, due to their being almost exclusively non- humans diverged from our closest living relatives, the coding sequences with no annotation. Ongoing research is chimpanzees and bonobos, although tests for accelerated beginning to crack this problem by leveraging new genome evolution have also been used to study older events [4 ] sequences, functional genomics data, computational and events in other lineages [10], as well as HARs that approaches, and genetic assays to reveal that many HARs are arose after divergence from archaic hominids [11,12,13 ]. developmental gene regulatory elements and RNA genes, most In this paper, we review the discovery of HARs, discuss of which evolved their uniquely human mutations through the evolutionary forces that may have shaped these fast- positive selection before divergence of archaic hominins and evolving sequences, and summarize what is known about diversification of modern humans.