Transcriptional Landscape of B Cell Precursor Acute Lymphoblastic Leukemia Based on an International Study of 1,223 Cases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Fast-Evolving Gene Is Key Player in Brain Development
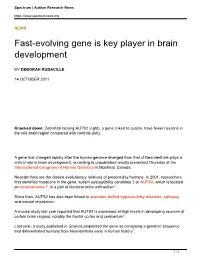
Spectrum | Autism Research News https://www.spectrumnews.org NEWS Fast-evolving gene is key player in brain development BY DEBORAH RUDACILLE 14 OCTOBER 2011 Knocked down: Zebrafish lacking AUTS2 (right), a gene linked to autism, have fewer neurons in the mid-brain region compared with controls (left). A gene that changed rapidly after the human genome diverged from that of Neanderthals plays a critical role in brain development, according to unpublished results presented Thursday at the International Congress of Human Genetics in Montreal, Canada. Neanderthals are the closest evolutionary relatives of present-day humans. In 2001, researchers first identified mutations in the gene, autism susceptibility candidate 2 or AUTS2, which is located on chromosome 7, in a pair of identical twins with autism1. Since then, AUTS2 has also been linked to attention deficit hyperactivity disorder, epilepsy and mental retardation. A mouse study last year reported that AUTS2 is expressed at high levels in developing neurons of certain brain regions, notably the frontal cortex and cerebellum2. Last year, a study published in Science pinpointed the gene as containing a genomic sequence that differentiated humans from Neanderthals early in human history3. 1 / 3 Spectrum | Autism Research News https://www.spectrumnews.org Still, the function of AUTS2 has remained elusive until now. Researchers at the University of California, San Francisco presented the first functional study of the gene, which they identified while searching for genes important in development. “We were looking for regions in the genome that have a lot of evolutionary conservation, which usually indicates an important developmental gene that needs tight regulation,” says lead investigator Nadav Ahituv, assistant professor of bioengineering and therapeutic sciences at the University of California, San Francisco. -

Aiolos Overexpression in Systemic Lupus Erythematosus B Cell
Aiolos Overexpression in Systemic Lupus Erythematosus B Cell Subtypes and BAFF-Induced Memory B Cell Differentiation Are Reduced by CC-220 This information is current as Modulation of Cereblon Activity of September 27, 2021. Yumi Nakayama, Jolanta Kosek, Lori Capone, Eun Mi Hur, Peter H. Schafer and Garth E. Ringheim J Immunol 2017; 199:2388-2407; Prepublished online 28 August 2017; Downloaded from doi: 10.4049/jimmunol.1601725 http://www.jimmunol.org/content/199/7/2388 http://www.jimmunol.org/ Supplementary http://www.jimmunol.org/content/suppl/2017/08/26/jimmunol.160172 Material 5.DCSupplemental References This article cites 131 articles, 45 of which you can access for free at: http://www.jimmunol.org/content/199/7/2388.full#ref-list-1 Why The JI? Submit online. by guest on September 27, 2021 • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Author Choice Freely available online through The Journal of Immunology Author Choice option Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2017 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. -

Detection of Pathogenic Isoforms of IKZF1 in Leukemic Cell
cancers Article Detection of Pathogenic Isoforms of IKZF1 in Leukemic Cell Lines and Acute Lymphoblastic Leukemia Samples: Identification of a Novel Truncated IKZF1 Transcript in SUP-B15 Weiqiang Zhao 1,*, Ying Li 2 , Chenjiao Yao 2 , Guojuan Zhang 1, Kevin Y. Zhao 1, Wei Chen 1, Peng Ru 1, Xiaokang Pan 1, Huolin Tu 1 and Daniel Jones 1 1 The James Comprehensive Cancer Center and Solove Research Institute, The Ohio State University, Columbus, OH 43210, USA; [email protected] (G.Z.); [email protected] (K.Y.Z.); [email protected] (W.C.); [email protected] (P.R.); [email protected] (X.P.); [email protected] (H.T.); [email protected] (D.J.) 2 The Department of Pediatrics and Department of Hematology, Xiang-Ya Third Hospital, Changsha 410013, China; [email protected] (Y.L.); [email protected] (C.Y.) * Correspondence: [email protected]; Tel.: +1-6142934210 Received: 27 August 2020; Accepted: 22 October 2020; Published: 28 October 2020 Simple Summary: Abnormal RNA splicing plays a fundamental role in leukemogenesis in acute lymphoblastic leukemia (ALL). Many cases of high-risk B-cell ALL cases, including BCR-ABL1+ and BCR-ABL1-like ALL, share a common molecular mechanism of aberrant fusion transcripts involving tyrosine kinase genes combined with dysregulation of the transcription factor and lymphocyte differentiation factor IKZF1. Dysfunction of IKZF1 in ALL is caused by mutation and gene deletion but also alternative splicing resulting in exon skipping with production of aberrant IKZF1 proteins. We report here an assay to detect aberrantly spliced isoforms of IKZF1 in ALL to assist in diagnosis, outcome prediction, and therapy selection in ALL and the identification of a novel altered IKZF1 product in a model ALL cell line. -

A Low‐Grade Astrocytoma in a Sixteen‐Year‐Old Boy with a 7Q11.22 Deletion
CASE REPORT A low-grade astrocytoma in a sixteen-year-old boy with a 7q11.22 deletion Francoise S. van Kampen1 , Marianne E. Doornbos1, Monique A. van Rijn2 & Yolande den Bever3 1Department of Paediatrics, Albert Schweitzer Hospital, Dordrecht, The Netherlands 2Department of Neurology, Albert Schweitzer Hospital, Dordrecht, The Netherlands 3Department of Clinical Genetics, Erasmus University Hospital, Rotterdam, The Netherlands Correspondence Key Clinical Message Franciscus Vlietland Group Vlietlandplein 2 Postbus 215 3100 AE Schiedam We report a patient with developmental delay due to germline AUTS2 muta- Tel: (0031)108939393 tion who developed a low-grade astrocytoma. While the contribution of this E-mail: [email protected] mutation to the pathogenesis of the tumor is not known at this time, a role of AUTS2 in deregulation of PRC1 can be a part in tumorigenesis of a brain tumor. Funding Information No sources of funding were declared for this study. Keywords AUTS2, brain tumor, neurologic, pediatric. Received: 29 October 2016; Revised: 26 October 2017; Accepted: 13 November 2017 Clinical Case Reports 2018; 6(2): 274–277 doi: 10.1002/ccr3.1312 Background drives the formation of most low-grade gliomas (LGG). The most common mechanism of a MAPK pathway acti- In this case report, we describe a first patient with a low- vation in LGG’s is a tandem duplication on chromosome grade astrocytoma and a deletion in the AUTS2 gene. 7q34. In addition, deletions in 7q34 are described [4]. Mutations in (parts of) the autism susceptibility candidate Astrocytomas are occasionally described in Noonan, 2 (AUTS2) are described in case reports and further Turner, Lynch syndrome, and neurofibromatosis. -
Genomic Divergence and Brain Evolution: How Regulatory DNA Influences Development of the Cerebral Cortex
Prospects & Overviews Review essays Genomic divergence and brain evolution: How regulatory DNA influences development of the cerebral cortex Debra L. Silver1)2)3)4) The cerebral cortex controls our most distinguishing higher Introduction cognitive functions. Human-specific gene expression dif- ferences are abundant in the cerebral cortex, yet we have A large six-layered neocortex is a unique feature of only begun to understand how these variations impact brain mammalian brains. This specialized outer covering of the brain controls our higher cognitive functions including function. This review discusses the current evidence linking abstract thought and language, which together help uniquely non-coding regulatory DNA changes, including enhancers, define us as humans. Our distinguishing cognitive capacities with neocortical evolution. Functional interrogation using are specified within discrete cortical areas and are driven by animal models reveals converging roles for our genome in dynamic communication between neurons of the neocortex key aspects of cortical development including progenitor and other brain regions, as well as glial cell populations (including oligodendrocytes, microglia, and astrocytes). cell cycle and neuronal signaling. New technologies, Neurons are initially generated during human embryonic includingiPS cells and organoids, offerpotential alternatives and early fetal development, where they migrate to appropri- to modeling evolutionary modifications in a relevant species ate regions and begin establishing functional connections context. Several diseases rooted in the cerebral cortex during fetal and postnatal stages (Fig. 1). Disruptions to uniquely manifest in humans compared to other primates, cerebral cortex function arising during either development or thus highlighting the importance of understanding human adulthood, can result in neurodevelopmental and neurode- generative disorders. -

Investigation of the Underlying Hub Genes and Molexular Pathogensis in Gastric Cancer by Integrated Bioinformatic Analyses
bioRxiv preprint doi: https://doi.org/10.1101/2020.12.20.423656; this version posted December 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Investigation of the underlying hub genes and molexular pathogensis in gastric cancer by integrated bioinformatic analyses Basavaraj Vastrad1, Chanabasayya Vastrad*2 1. Department of Biochemistry, Basaveshwar College of Pharmacy, Gadag, Karnataka 582103, India. 2. Biostatistics and Bioinformatics, Chanabasava Nilaya, Bharthinagar, Dharwad 580001, Karanataka, India. * Chanabasayya Vastrad [email protected] Ph: +919480073398 Chanabasava Nilaya, Bharthinagar, Dharwad 580001 , Karanataka, India bioRxiv preprint doi: https://doi.org/10.1101/2020.12.20.423656; this version posted December 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Abstract The high mortality rate of gastric cancer (GC) is in part due to the absence of initial disclosure of its biomarkers. The recognition of important genes associated in GC is therefore recommended to advance clinical prognosis, diagnosis and and treatment outcomes. The current investigation used the microarray dataset GSE113255 RNA seq data from the Gene Expression Omnibus database to diagnose differentially expressed genes (DEGs). Pathway and gene ontology enrichment analyses were performed, and a proteinprotein interaction network, modules, target genes - miRNA regulatory network and target genes - TF regulatory network were constructed and analyzed. Finally, validation of hub genes was performed. The 1008 DEGs identified consisted of 505 up regulated genes and 503 down regulated genes. -

Shallow Whole Genome Sequencing On
Author Manuscript Published OnlineFirst on July 14, 2017; DOI: 10.1158/1078-0432.CCR-17-0675 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Shallow whole genome sequencing on circulating cell-free DNA allows reliable non- invasive copy number profiling in neuroblastoma patients Nadine Van Roy1,4, Malaïka Van Der Linden1,3, Björn Menten1, Annelies Dheedene1, Charlotte Vandeputte 1,4, Jo Van Dorpe3, Geneviève Laureys2,4, Marleen Renard5, Tom Sante1,Tim Lammens2,4, Bram De Wilde2,4, Frank Speleman1,4, Katleen De Preter1,4,* 1Center for Medical Genetics, Ghent University, Ghent, Belgium 2Department of Pediatric Hematology-Oncology and Stem Cell Transplantation, Ghent University Hospital, Ghent, Belgium 3Department of Pathology, Ghent University, Ghent, Belgium 4Cancer Research Institute Ghent, Ghent University, Ghent, Belgium 5Department of Pediatric Hematology-Oncology and Stem Cell Transplantation, Leuven University Hospital, Leuven, Belgium *Corresponding author Running title: non-invasive copy number profiling using shallow WGS Keywords: neuroblastoma, cell-free DNA, copy number profiling, shallow whole genome sequencing, non-invasive The authors would like to thank the following funding agencies: the Belgian Foundation against Cancer (project 2015-146) to FS, the Flemish liga against cancer (B/14651/01 and STIVLK2016000601), Ghent University (BOF16/GOA/23) to FS, the Belgian Program of Interuniversity Poles of Attraction (IUAP Phase VII - P7/03) to FS, the Fund for Scientific Research Flanders (Research project G021415N) to KDP and project 18B1716N to BDW, the European Union H2020 (OPTIMIZE-NB GOD9415N and TRANSCAN-ON THE TRAC GOD8815N) to FS. The Ghent University Hospital innovation project for molecular pathology (project number: KW/1694/PAN/001/001) to JVD and MVDL, vzw Kinderkankerfonds, a non-profit childhood cancer foundation under Belgian law to TL. -

Novel Gene Targets Detected by Genomic Profiling in a Consecutive Series of 126 Adults with Acute Lymphoblastic Leukemia
Acute Lymphoblastic Leukemia ARTICLES Novel gene targets detected by genomic profiling in a consecutive series of 126 adults with acute lymphoblastic leukemia Setareh Safavi,1 Markus Hansson,2 Karin Karlsson,2 Andrea Biloglav,1 Bertil Johansson,1,3 and Kajsa Paulsson1 1Division of Clinical Genetics, Department of Laboratory Medicine, Lund University; 2Division of Hematology, Skåne University Hospital, Lund University; and 3Department of Clinical Genetics, University and Regional Laboratories, Region Skåne, Lund, Sweden ABSTRACT In contrast to acute lymphoblastic leukemia in children, adult cases of this disease are associated with a very poor prognosis. In order to ascertain whether the frequencies and patterns of submicroscopic changes, identifiable with single nucleotide polymorphism array analysis, differ between childhood and adult acute lymphoblastic leukemia, we performed single nucleotide polymorphism array analyses of 126 adult cases, the largest series to date, includ- ing 18 paired diagnostic and relapse samples. Apart from identifying characteristic microdeletions of the CDKN2A, EBF1, ETV6, IKZF1, PAX5 and RB1 genes, the present study uncovered novel, focal deletions of the BCAT1, BTLA, NR3C1, PIK3AP1 and SERP2 genes in 2-6% of the adult cases. IKZF1 deletions were associated with B-cell pre- cursor acute lymphoblastic leukemia (P=0.036), BCR-ABL1-positive acute lymphoblastic leukemia (P<0.001), and higher white blood cell counts (P=0.005). In addition, recurrent deletions of RASSF3 and TOX were seen in relapse samples. Comparing paired diagnostic/relapse samples revealed identical changes at diagnosis and relapse in 27%, clonal evolution in 22%, and relapses evolving from ancestral clones in 50%, akin to what has previously been reported in pediatric acute lymphoblastic leukemia and indicating that the mechanisms of relapse may be similar in adult and childhood cases. -

Immunogenic Dendritic Cell Generation from Pluripotent Stem Cells by Ectopic Expression of Runx3
Immunogenic Dendritic Cell Generation from Pluripotent Stem Cells by Ectopic Expression of Runx3 This information is current as Erika Takacs, Pal Boto, Emilia Simo, Tamas I. Csuth, of September 25, 2021. Bianka M. Toth, Hadas Raveh-Amit, Attila Pap, Elek G. Kovács, Julianna Kobolak, Szilvia Benkö, Andras Dinnyes and Istvan Szatmari J Immunol published online 16 November 2016 http://www.jimmunol.org/content/early/2016/11/15/jimmun Downloaded from ol.1600034 Supplementary http://www.jimmunol.org/content/suppl/2016/11/15/jimmunol.160003 Material 4.DCSupplemental http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 25, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2016 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Published November 16, 2016, doi:10.4049/jimmunol.1600034 The Journal of Immunology Immunogenic Dendritic Cell Generation from Pluripotent Stem Cells by Ectopic Expression of Runx3 Erika Takacs,*,1 Pal Boto,*,1 Emilia Simo,* Tamas I. Csuth,* Bianka M. -

Dual Targeting of MTOR As a Novel Therapeutic Approach for High-Risk B-Cell Acute Lymphoblastic Leukemia
Leukemia (2021) 35:1267–1278 https://doi.org/10.1038/s41375-021-01132-5 ARTICLE ACUTE LYMPHOBLASTIC LEUKEMIA Dual targeting of MTOR as a novel therapeutic approach for high-risk B-cell acute lymphoblastic leukemia 1,2 1,3 1 1 1 1 Zheng Ge ● Chunhua Song ● Yali Ding ● Bi-Hua Tan ● Dhimant Desai ● Arati Sharma ● 1 1 1 1 1,4 Raghavendra Gowda ● Feng Yue ● Suming Huang ● Vladimir Spiegelman ● Jonathon L. Payne ● 4 1 1 1 1 Mark E. Reeves ● Soumya Iyer ● Pavan Kumar Dhanyamraju ● Yuka Imamura ● Daniel Bogush ● 1 3 1 1 1 1 Yevgeniya Bamme ● Yiping Yang ● Mario Soliman ● Shriya Kane ● Elanora Dovat ● Joseph Schramm ● 1 1 1 4 1 1 Tommy Hu ● Mary McGrath ● Zissis C. Chroneos ● Kimberly J. Payne ● Chandrika Gowda ● Sinisa Dovat Received: 26 September 2020 / Revised: 28 November 2020 / Accepted: 7 January 2021 / Published online: 2 February 2021 © The Author(s) 2021. This article is published with open access Abstract Children of Hispanic/Latino ancestry have increased incidence of high-risk B-cell acute lymphoblastic leukemia (HR B-ALL) with poor prognosis. This leukemia is characterized by a single-copy deletion of the IKZF1 (IKAROS) tumor suppressor and increased activation of the PI3K/AKT/mTOR pathway. This identifies mTOR as an attractive therapeutic target in HR B-ALL. ’ 1234567890();,: 1234567890();,: Here, we report that IKAROS represses MTOR transcription and IKAROS ability to repress MTOR in leukemia is impaired by oncogenic CK2 kinase. Treatment with the CK2 inhibitor, CX-4945, enhances IKAROS activity as a repressor of MTOR, resulting in reduced expression of MTOR in HR B-ALL. -

Diapositivo 1
Silvia Serafim*; Barbara Marques*; Filomena Brito*; Sonia Pedro*; Cristina Ferreira*; Catarina Ventura*; Isabel Gaspar**; Hildeberto Correia* *Unidade de Citogenetica, Instituto Nacional de Saude Doutor Ricardo Jorge, I.P., Lisboa, Portugal **Consulta de Genetica Medica, Hospital Egas Moniz, Centro Hospitalar de Lisboa Ocidental EPE, Lisboa, Portugal Introduction Chromosome Microarray Analysis is a powerful diagnostic tool and is being used as a first-line approach to detect chromosome imbalances associated with intellectual disability, dysmorphic features and congenital anomalies. This test enables the identification of new copy number variants (CNVs) and their association with new microdeletion/microduplication syndromes in patients previously studied by conventional cytogenetics analysis. Here we report the case of a female with severe intellectual disability, absence of speech, microcephaly and congenital abnormalities with a previous normal karyotype performed at a younger age. Microarray analysis was performed at 17 years of age, in order to assess if a genome unbalance could explain the patient’s undiagnosed phenotype. A small deletion was found in autism susceptibility candidate 2 (AUTS2) gene . The AUTS2 gene has been recently implicated in autosomal dominant mental retardation with variable syndromic phenotype (OMIM *607270, #615834). Common clinical features described in patients with deletions in AUTS2 gene include autism, intellectual disability, speech delay and microcephaly, among others (1,2,3,4,5,6). We compare our patient with similar reported cases, adding additional value to the phenotype-genotype correlation of CNVs in this region. Method Microarray analysis was carried out in DNA extracted from peripheral blood using Affymetrix CytoScan HD chromosome microarray platform according to the manufacturer’s recommendations. -

A KMT2A-AFF1 Gene Regulatory Network Highlights the Role of Core Transcription Factors and Reveals the Regulatory Logic of Key Downstream Target Genes
Downloaded from genome.cshlp.org on October 7, 2021 - Published by Cold Spring Harbor Laboratory Press Research A KMT2A-AFF1 gene regulatory network highlights the role of core transcription factors and reveals the regulatory logic of key downstream target genes Joe R. Harman,1,7 Ross Thorne,1,7 Max Jamilly,2 Marta Tapia,1,8 Nicholas T. Crump,1 Siobhan Rice,1,3 Ryan Beveridge,1,4 Edward Morrissey,5 Marella F.T.R. de Bruijn,1 Irene Roberts,3,6 Anindita Roy,3,6 Tudor A. Fulga,2,9 and Thomas A. Milne1,6 1MRC Molecular Haematology Unit, MRC Weatherall Institute of Molecular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, OX3 9DS, United Kingdom; 2MRC Weatherall Institute of Molecular Medicine, Radcliffe Department of Medicine, University of Oxford, Oxford, OX3 9DS, United Kingdom; 3MRC Molecular Haematology Unit, MRC Weatherall Institute of Molecular Medicine, Department of Paediatrics, University of Oxford, Oxford, OX3 9DS, United Kingdom; 4Virus Screening Facility, MRC Weatherall Institute of Molecular Medicine, John Radcliffe Hospital, University of Oxford, Oxford, OX3 9DS, United Kingdom; 5Center for Computational Biology, Weatherall Institute of Molecular Medicine, University of Oxford, John Radcliffe Hospital, Oxford OX3 9DS, United Kingdom; 6NIHR Oxford Biomedical Research Centre Haematology Theme, University of Oxford, Oxford, OX3 9DS, United Kingdom Regulatory interactions mediated by transcription factors (TFs) make up complex networks that control cellular behavior. Fully understanding these gene regulatory networks (GRNs) offers greater insight into the consequences of disease-causing perturbations than can be achieved by studying single TF binding events in isolation. Chromosomal translocations of the lysine methyltransferase 2A (KMT2A) gene produce KMT2A fusion proteins such as KMT2A-AFF1 (previously MLL-AF4), caus- ing poor prognosis acute lymphoblastic leukemias (ALLs) that sometimes relapse as acute myeloid leukemias (AMLs).