VI; Mogadi Hu.. VII, Middle Shabelli
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

OCHA SOMALIA Flash Update 4 Humanitarian Impact of Heavy Rains | 20 November 2015
OCHA SOMALIA Flash Update 4 Humanitarian impact of heavy rains | 20 November 2015 Situation overview During the past week, there has been a reduction in the amount of rainfall and floods in most areas of Juba and Shabelle basins inside Somalia as well as the Ethiopian highlands, according to the FAO-Managed Somalia Land and Water Information Network (SWALIM). However, the risk of flooding remains high should the rains continue. The recent floods led to the destruction of main supply roads. This has hampered the delivery of produce to the markets, leading to an escalation of commodity prices. According to the authorities, the main supply roads from Mogadishu to Baidoa, Mogadishu to Kismayo, and Mogadishu to Belet Weyne have been destroyed and are nearly impassable. The floods also rendered some airstrips unusable, hampering the delivery of humanitarian aid to some of the affected regions. Belet Weyne airstrip closed for few days due to floods but is now operational. There is need to urgently repair main lifeline roads, bridges and airstrips. This will ensure supplies can reach the markets to stabilize the escalating food prices and enable humanitarian partners and aid supplies to reach those most in need of assistance. Current rains, localized flash floods in some districts of Puntland and floods in parts of South Central Somalia, have resulted in a significant increase in Acute Watery Diarrhea (AWD) cases in multiple regions, according to WHO and the Health Cluster. With the riverine areas still at moderate and high risk of flooding, the number of people seeking treatment at health facilities for various illnesses is expected to increase and AWD cases could escalate. -

From the Bottom
Conflict Early Warning Early Response Unit From the bottom up: Southern Regions - Perspectives through conflict analysis and key political actors’ mapping of Gedo, Middle Juba, Lower Juba, and Lower Shabelle - SEPTEMBER 2013 With support from Conflict Dynamics International Conflict Early Warning Early Response Unit From the bottom up: Southern Regions - Perspectives through conflict analysis and key political actors’ mapping of Gedo, Middle Juba, Lower Juba, and Lower Shabelle Version 2 Re-Released Deceber 2013 with research finished June 2013 With support from Conflict Dynamics International Support to the project was made possible through generous contributions from the Government of Norway Ministry of Foreign Affairs and the Government of Switzerland Federal Department of Foreign Affairs. The views expressed in this paper do not necessarily reflect the official position of Conflict Dynamics International or of the Governments of Norway or Switzerland. CONTENTS Abbreviations 7 ACKNOWLEDGMENT 8 Conflict Early Warning Early Response Unit (CEWERU) 8 Objectives 8 Conflict Dynamics International (CDI) 8 From the Country Coordinator 9 I. OVERVIEW 10 Social Conflict 10 Cultural Conflict 10 Political Conflict 10 II. INTRODUCTION 11 Key Findings 11 Opportunities 12 III. GEDO 14 Conflict Map: Gedo 14 Clan Chart: Gedo 15 Introduction: Gedo 16 Key Findings: Gedo 16 History of Conflict: Gedo 16 Cross-Border Clan Conflicts 18 Key Political Actors: Gedo 19 Political Actor Mapping: Gedo 20 Clan Analysis: Gedo 21 Capacity of Current Government Administration: Gedo 21 Conflict Mapping and Analysis: Gedo 23 Conflict Profile: Gedo 23 Conflict Timeline: Gedo 25 Peace Initiative: Gedo 26 IV. MIDDLE JUBA 27 Conflict Map: Middle Juba 27 Clan Chart: Middle Juba 28 Introduction: Middle Juba 29 Key Findings: Middle Juba 29 History of Conflict : Middle Juba 29 Key Political Actors: Middle Juba 29 Political Actor Mapping: Middle Juba 30 Capacity of Current Government Administration: Middle Juba 31 Conflict Mapping and Analysis: Middle Juba 31 Conflict Profile: Middle Juba 31 V. -
Somalia from Resilience Towards Recovery and Development
Report No.34356-SO Report No. 34356-SO Somalia From Resilience Towards Recovery and Development Public Disclosure Authorized Public Disclosure Authorized A Country Economic Memorandum for Somalia January 11, 2006 Poverty Reduction and Economic Management 2 Country Department for Somalia Africa Region Somalia and Development Recovery Towards Resilience From Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Document of the World Bank GFATM Global Fund to Fight Aids, Tuberculosis and Malaria ICAO International Civil Aviation Organization ICRC International Committee ofthe Red Cross IDA International Development Association IDP Internally Displaced People IFAD International Fund for Agriculture Development IFC International Finance Corporation IMF International Monetary Fund ITCZ Inter-Tropical Convergence Zone ITU International Telecommunication Union JNA Joint Needs Assessment KPHIS Kenya Plant Health Inspectorate Service KSA Kingdom of Saudi Arabia LDC Least Developed Country LICUS Low Income Countries under Stress MCH Maternal and Child Health MDG MillenniumDevelopment Goal MDRP Multi-Country Demobilization and Reintegration Program MDTF Multi-Donor Trust Fund MICS Multi Indicators Cluster Survey NGO NonGovernmental Organization ODA Official Development Assistance OECD Organization of Economic Cooperation and Development PHC Primary Health Care RRA Rahanweyn Residtance Army PRS Poverty Reduction Strategy SACB Somalia -
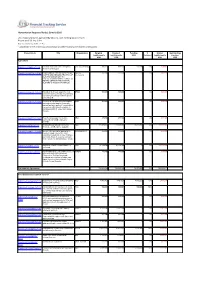
With Funding Status of Each Report As
Humanitarian Response Plan(s): Somalia 2016 List of appeal projects (grouped by Cluster), with funding status of each Report as of 23-Sep-2021 http://fts.unocha.org (Table ref: R3) Compiled by OCHA on the basis of information provided by donors and recipient organizations. Project Code Title Organization Original Revised Funding % Unmet Outstanding requirements requirements USD Covered requirements pledges USD USD USD USD Agriculture SOM-16/A/84942/5110 Puntland and Lower Juba Emergency VSF (Switzerland) 998,222 998,222 588,380 59% 409,842 0 Animal Health Support SOM-16/A/86501/15092 PROVISION OF FISHING INPUTS FOR SAFUK- 352,409 352,409 0 0% 352,409 0 YOUTHS AND MEN AND TRAINING OF International MEN AND WOMEN ON FISH PRODUCTION AND MAINTENANCE OF FISHING GEARS IN THE COASTAL REGIONS OF MUDUG IN SOMALIA. SOM-16/A/86701/14592 Integrated livelihoods support to most BRDO 500,000 500,000 0 0% 500,000 0 vulnerable conflict affected 2850 farming and fishing households in Marka district Lower Shabelle. SOM-16/A/86746/14852 Provision of essential livelihood support HOD 500,000 500,000 0 0% 500,000 0 and resilience building for Vulnerable pastoral and agro pastoral households in emergency, crisis and stress phase in Kismaayo district of Lower Juba region, Somalia SOM-16/A/86775/17412 Food Security support for destitute NRO 499,900 499,900 0 0% 499,900 0 communities in Middle and Lower Shabelle SOM-16/A/87833/123 Building Household and Community FAO 111,805,090 111,805,090 15,981,708 14% 95,823,382 0 Resilience and Response Capacity SOM-16/A/88141/17597 Access to live-saving for population in SHARDO Relief 494,554 494,554 0 0% 494,554 0 emergency and crises of the most vulnerable households in lower Shabelle and middle Shabelle regions, and build their resilience to withstand future shocks. -

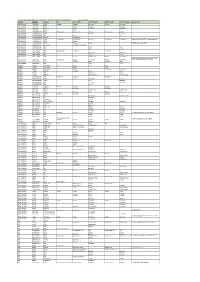
S.No Region Districts 1 Awdal Region Baki
S.No Region Districts 1 Awdal Region Baki District 2 Awdal Region Borama District 3 Awdal Region Lughaya District 4 Awdal Region Zeila District 5 Bakool Region El Barde District 6 Bakool Region Hudur District 7 Bakool Region Rabdhure District 8 Bakool Region Tiyeglow District 9 Bakool Region Wajid District 10 Banaadir Region Abdiaziz District 11 Banaadir Region Bondhere District 12 Banaadir Region Daynile District 13 Banaadir Region Dharkenley District 14 Banaadir Region Hamar Jajab District 15 Banaadir Region Hamar Weyne District 16 Banaadir Region Hodan District 17 Banaadir Region Hawle Wadag District 18 Banaadir Region Huriwa District 19 Banaadir Region Karan District 20 Banaadir Region Shibis District 21 Banaadir Region Shangani District 22 Banaadir Region Waberi District 23 Banaadir Region Wadajir District 24 Banaadir Region Wardhigley District 25 Banaadir Region Yaqshid District 26 Bari Region Bayla District 27 Bari Region Bosaso District 28 Bari Region Alula District 29 Bari Region Iskushuban District 30 Bari Region Qandala District 31 Bari Region Ufayn District 32 Bari Region Qardho District 33 Bay Region Baidoa District 34 Bay Region Burhakaba District 35 Bay Region Dinsoor District 36 Bay Region Qasahdhere District 37 Galguduud Region Abudwaq District 38 Galguduud Region Adado District 39 Galguduud Region Dhusa Mareb District 40 Galguduud Region El Buur District 41 Galguduud Region El Dher District 42 Gedo Region Bardera District 43 Gedo Region Beled Hawo District www.downloadexcelfiles.com 44 Gedo Region El Wak District 45 Gedo -

Somalia Floods Update 7 May 2018
SOMALIA FLOODS UPDATE 7 MAY 2018 TAKEAWAY MESSAGE In the 21st Century, Somalia has experienced drought and floods during 17 out of 18 years. “Normal rains” are no longer the norm. Somalia’s damaged and degrading infrastructure (since civil war in early 1990s) is compounding the situation. 1960s 1970s 1980s 1990s 2000s 2010s Flood Drought Data source: CRED Database Well-functioning and managed water infrastructure would have significantly reduced the impacts of both the recent 2016/17 drought and ongoing flood emergency, in human and financial terms. This requires concerted, small and large-scale investments. Example: A recent DFID project funded machinery works to repair and strengthen 22 000+ metres of the Shabelle River’s embankments to prepare for floods this season. To date, no flooding is reported in 47 out of the 48 surrounding villages that benefitted. FAO calls on partners to scale up investment in the water infrastructure and management systems that Somalia needs to build back better from the drought and ongoing flood emergency. KEY MESSAGES IN RURAL AREAS An estimated 630 000 people are affected by flash and river floods in and around Somalia’s breadbasket during Gu 2018 – the main agricultural season. The Gu cropping season (April-June) is not lost, but delayed in flooded areas until waters recede. Along the Juba and Shabelle, up to 50 000 hectares are under water: ≈70% is yet to be cultivated; 30% was cropped early and damaged. Livestock risk disease, including vector-borne diseases that can also impact human health. As rains continue over the next 3-4 weeks, this is expected to compound the impact of floods in affected and at risk areas. -

Health Cluster Bulletin August 2017 (Issued September
August 2017 (Issued September 29) Health Cluster Bulletin 260 Sentinel Sites 1.1m Internally Displaced Since start of 2017, basic health services provided to > 2.08 million Somalis. 6.2m People Affected 5.5m in Need of Health Services AWD/Cholera Outbreak Jan– August 2017 Highlights On the 13th of August, a national event was held by the government in Mogadishu to celebrate 3-years Polio Free Somalia. The President of the Federal Government of Somalia, Cabinet ministers, WHO Regional Director, DSRSG/UNRC/HC and others attended this national celebration of this event. The month of August has seen a sustained decline in the number of cases of cholera reported from across Somalia. The 917 cases recorded in August 2017 now approximate to the averaged monthly figures recorded in 2015 of 440 cases and during 2016 of 1,300 cases/month. The focus now moves towards cholera preparedness in advance of the forthcoming October rains. The numbers of cases of measles remain at epidemic levels with more than 1491 cases being recorded in August. A nationwide campaign to vaccinate all 4.2 million children in the country between the ages of 6 months and 10 years will begin in November/December 2017. During August, the Somalia Humanitarian Fund committed $1 million to financing of the campaign. (Left) HE The President of Somalia Mohamed Abdullahi presenting an award to WHO Regional Director Dr. Mahmoud- Fikri in gratitude to WHO’s effort and support. Photo courtesy of WHO 1 Summary of Humanitarian Situation Cholera Updates cont... Somalia is in its second year of widespread drought. -
Region District Partner SC OTP Static OTP Mobile TSFP Static TSFP
NUTRITION CLUSTER SOUTH CENTRAL ZONE RATIONALIZATION PLAN 15 April, 2014 Region District Partner SC OTP Static OTP Mobile TSFP Static TSFP Mobile Comments GALGADUUD CADAADO HRDO Cadaado Cadaado Biyogadud Cadaado Biyogadud GALGADUUD CADAADO HRDO Baxado Docole Docoley GALGADUUD CADAADO Observer Galinsor Gondinlabe Gondinlabe GALGADUUD CADAADO Observer Adado Baxado GALGADUUD DHUSAMAREEB TUOS Dhusamareeb Dhusamareeb Gadoon Dhusamareeb Gadoon GALGADUUD DHUSAMAREEB TUOS El -Dheere El -Dheere GALGADUUD DHUSAMAREEB WCI Guri-el Guri-el GALGADUUD DHUSAMAREEB Observer Dhusamareeb GALGADUUD CAABUDWAAQ HDOS Caabudwaaq Caabudwaaq Bangeele Caabudwaaq Caabudwaaq I static and 1 mobile TSFP in Cabduwaaq town GALGADUUD CAABUDWAAQ HDOS Baltaag GALGADUUD CAABUDWAAQ HOPEL Balanbale Balanbale Balanbale will be semi-static GALGADUUD CAABUDWAAQ Mercy USA Cabudwaaq Town West GALGADUUD CAABUDWAAQ HDO Xerale Xerale GALGADUUD CAABUDWAAQ SCI Dhabat Dhabat GALGADUUD CEEL DHEER CISP CEEL DHEER Ceel Dheer Ceel Dheer GALGADUUD CEEL DHEER SRC Hul Caduur Hul Caduur GALGADUUD CEEL DHEER SRC Oswein Oswein GALGADUUD CEEL DHEER Merlin Galcad Mesagaweyn Galcad Mesagaweyn DEH to inform on discussion with Merlin or else GALGADUUD CEEL BUUR Merlin CEEL BUUR Elgaras Ceel Qooxle Elgaras Ceel Qooxle Merlin will manage Ceel buur SC&OTP GALGADUUD CEEL BUUR Merlin Ceel Buur Jacar Ceel Buur Jacar GALGADUUD CEEL BUUR DEH Xindhere Xindhere MUDUG HOBYO Mercy USA Wisil Hobyo Wisil Hobyo MUDUG HOBYO Mercy USA El dibir El dibir MUDUG HOBYO Mercy USA Gawan Ceelguula Ceelguula MUDUG HOBYO GMPHCC -

Narratives of Famine – Somalia 2011
January 2016 Strengthening the humanity and dignity of people in crisis through knowledge and practice NARRATIVES OF FAMI N E Somalia 2011 Nisar Majid, Guhad Adan, Khalif Abdirahman, Jeeyon Janet Kim, Daniel Maxwell Cover Image by Nisar Majid. Acknowledgements: We gratefully acknowledge the support of the Bill and Melinda Gates Foundation and the USAID Office of Foreign Disaster Assistance for the research on which this paper is based and support from the Norwegian Ministry of Foreign Affairs for the analysis and compilation of the narratives. We would like to thank Dyan Mazurana for her insightful review of this paper and Joyce Maxwell for editing and formatting the report. ©2016 Feinstein International Center. All Rights Reserved. Fair use of this copyrighted material includes its use for non-commercial educational purposes, such as teaching, scholarship, research, criticism, commentary, and news reporting. Unless otherwise noted, those who wish to reproduce text and image files from this publication for such uses may do so without the Feinstein International Center’s express permission. However, all commercial use of this material and/or reproduction that alters its meaning or intent, without the express permission of the Feinstein International Center, is prohibited. Feinstein International Center Tufts University 114 Curtis Street Somerville, MA 02144 USA tel: +1 617.627.3423 fax: +1 617.627.3428 fic.tufts.edu Contents Acronyms 4 Terminology 4 Executive Summary 5 Introduction 5 Social structures, hierarchies and networks in Somalia -
Voluntary Repatriation of Somali Refugees from Kenya
©UNHCR / A. Nasrullah ©UNHCR VOLUNTARY REPATRIATION OF SOMALI REFUGEES FROM KENYA OPERATIONS PLAN JULY 2015 - DECEMBER 2019 This operations plan is guided by the operations strategy endorsed by the Tripartite Commission for the voluntary repatriation of Somali refugees from Kenya. It is based on the positive evaluation of the pilot phase concluded on 30 June 2015, which supported the launch of the enhanced phase of the repatriation exercise from July 2015. It constitutes an operational guide for UNHCR and its partners in Kenya and Somalia to strengthen the voluntary repatriation process to support returns of Somali refugees from Kenya and their reintegration in Somalia. General reference is made to the UNHCR Regional Strategy “Enhancing the Search of Durable Solutions for Somali Refugees” of May 2013 and the Voluntary Return Strategy for Somali Refugees from Kenya to Somalia of July 2015. Table of Contents 1. Context................................................................................................................... 5 2. Geographical coverage and Action Plan ............................................................... 7 2.1 Reception and assistance .................................................................................................................................. 7 3. Implementation modalities ................................................................................... 9 3.1 Definitions of target groups: ........................................................................................................................... -
SOMALIA Post-Deyr 2012 Food Security and Nutrition Outlook January to June 2013
SOMALIA Post-Deyr 2012 Food Security and Nutrition Outlook January to June 2013 Despite improvements, more than one million likely to remain in Crisis through June 2013 KEY MESSAGES Figure 1. Current rural food security outcomes, January 2013 • As a result of positive impact of the good Deyr rains on livestock and crop performance and continued humanitarian assistance, the number of people in Crisis and Emergency (IPC Phases 3 and 4) has halved to 1.05 million since August. Even so, malnutrition rates in Somalia remain among the highest in the world, according to surveys conducted from October to December 2012. Humanitarian assistance to protect livelihoods, reduce acute malnutrition, and help the most food insecure populations meet their food needs is still necessary. • With the onset of the January to March Jilaal dry season, livestock productivity will decrease, but no major changes in food security classification are expected between now and June. However, livelihoods in Somalia remain at risk to a wide variety of hazards such as limited water access. • Early forecasts are that the April to June Gu rains will be normal to below normal in terms of total rainfall. However, if total seasonal rainfall is well below average or very poorly distributed unlike in the early forecast, the food insecure population is likely to increase. The primary areas affected would likely be maize-growing, agropastoral areas of the South. Source: FSNAU, FEWS NET Somalia, and partners Graphic: FSNAU This map represents acute food insecurity outcomes relevant for emergency decision-making. It does not necessarily reflect chronic food insecurity. -
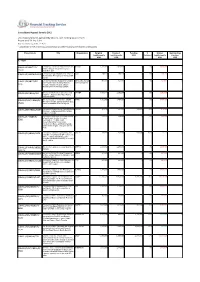
Somalia, Grouped by Priority
Consolidated Appeal: Somalia 2012 List of appeal projects (grouped by Cluster), with funding status of each Report as of 29-Sep-2021 http://fts.unocha.org (Table ref: R33) Compiled by OCHA on the basis of information provided by donors and recipient organizations. Project Code Title Organization Original Revised Funding % Unmet Outstanding requirements requirements USD Covered requirements pledges USD USD USD USD A - HIGH SOM-12/E/48177/R/ Emergency Education Response for IDPs AYUUB 1,274,921 1,070,918 0 0% 1,070,918 0 children through Integration in Lower 15231 Shabelle region SOM-12/F/48178/14852 Emergency Food Assistance for Those in HOD 299,223 299,223 0 0% 299,223 0 Humanitarian Emergency in Kismayo IDP Camps SOM-12/H/48255/R/ Emergency Nutrition Support for Children Mercy-USA for Aid 914,374 457,187 0 0% 457,187 0 and Pregnant and Lactating Mothers and Development 8396 through A Quality, Integrated Basic Nutrition Services Package (BNSP) SOM-12/H/48256/124 Emergency Outbreak preparedness and UNICEF 3,512,116 2,202,595 0 0% 2,202,595 0 response - Measles and Acute Watery Diarhoea (AWD) SOM-12/S-NF/48260/R/ Emergency project to distribute 25,000 SYPD 1,962,951 1,407,606 0 0% 1,407,606 0 NFI kits to drought- uprooted IDPs in Bay, 15101 Bakool and Middle Shabelle regions. SOM-12/ER/48261/8384 Emergency Response and Early Recovery PASOS 801,750 801,750 385,410 48% 416,340 0 Assistance in Burhakaba District of Bay Region of Somalia SOM-12/F/48264/R/ Emergency Response to increase access JCC 875,391 500,000 0 0% 500,000 0 to food in order to save lives and 8380 livelihoods of , 21,000( 3,500 households)facing humanitarian emergency in Bu'ale and Sakow/salagle, Middle Jubba Region, through Cash for Work.