Dissertation on a Study to Assess the Effectiveness of Lower Back
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of Village Panchayats in Tamil Nadu District Code District Name
List of Village Panchayats in Tamil Nadu District Code District Name Block Code Block Name Village Code Village Panchayat Name 1 Kanchipuram 1 Kanchipuram 1 Angambakkam 2 Ariaperumbakkam 3 Arpakkam 4 Asoor 5 Avalur 6 Ayyengarkulam 7 Damal 8 Elayanarvelur 9 Kalakattoor 10 Kalur 11 Kambarajapuram 12 Karuppadithattadai 13 Kavanthandalam 14 Keelambi 15 Kilar 16 Keelkadirpur 17 Keelperamanallur 18 Kolivakkam 19 Konerikuppam 20 Kuram 21 Magaral 22 Melkadirpur 23 Melottivakkam 24 Musaravakkam 25 Muthavedu 26 Muttavakkam 27 Narapakkam 28 Nathapettai 29 Olakkolapattu 30 Orikkai 31 Perumbakkam 32 Punjarasanthangal 33 Putheri 34 Sirukaveripakkam 35 Sirunaiperugal 36 Thammanur 37 Thenambakkam 38 Thimmasamudram 39 Thilruparuthikundram 40 Thirupukuzhi List of Village Panchayats in Tamil Nadu District Code District Name Block Code Block Name Village Code Village Panchayat Name 41 Valathottam 42 Vippedu 43 Vishar 2 Walajabad 1 Agaram 2 Alapakkam 3 Ariyambakkam 4 Athivakkam 5 Attuputhur 6 Aymicheri 7 Ayyampettai 8 Devariyambakkam 9 Ekanampettai 10 Enadur 11 Govindavadi 12 Illuppapattu 13 Injambakkam 14 Kaliyanoor 15 Karai 16 Karur 17 Kattavakkam 18 Keelottivakkam 19 Kithiripettai 20 Kottavakkam 21 Kunnavakkam 22 Kuthirambakkam 23 Marutham 24 Muthyalpettai 25 Nathanallur 26 Nayakkenpettai 27 Nayakkenkuppam 28 Olaiyur 29 Paduneli 30 Palaiyaseevaram 31 Paranthur 32 Podavur 33 Poosivakkam 34 Pullalur 35 Puliyambakkam 36 Purisai List of Village Panchayats in Tamil Nadu District Code District Name Block Code Block Name Village Code Village Panchayat Name 37 -
Branch Libraries List
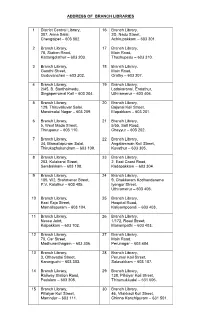
ADDRESS OF BRANCH LIBRARIES 1 District Central Library, 16 Branch Library, 307, Anna Salai, 2D, Nadu Street, Chengalpet – 603 002. Achirupakkam – 603 301. 2 Branch Library, 17 Branch Library, 78, Station Road, Main Road, Kattangolathur – 603 203. Thozhupedu – 603 310. 3 Branch Library, 18 Branch Library, Gandhi Street, Main Road, Guduvancheri – 603 202. Orathy – 603 307. 4 Branch Library, 19 Branch Library, 2/45, B. Santhaimedu, Ladakaranai, Endathur, Singaperrumal Koil – 603 204. Uthiramerur – 603 406. 5 Branch Library, 20 Branch Library, 129, Thiruvalluvar Salai, Bajanai Koil Street, Maraimalai Nagar – 603 209. Elapakkam – 603 201. 6 Branch Library, 21 Branch Library, 5, West Mada Street, 5/55, Salt Road, Thiruporur – 603 110. Cheyyur – 603 202. 7 Branch Library, 22 Branch Library, 34, Mamallapuram Salai, Angalamman Koil Street, Thirukazhukundram – 603 109. Kuvathur – 603 305. 8 Branch Library, 23 Branch Library, 203, Kulakarai Street, 2, East Coast Road, Sembakkam – 603 108. Kadapakkam – 603 304. 9 Branch Library, 24 Branch Library, 105, W2, Brahmanar Street, 9, Chakkaram Kodhandarama P.V. Kalathur – 603 405. Iyengar Street, Uthiramerur – 603 406. 10 Branch Library, 25 Branch Library, East Raja Street, Hospital Road, Mamallapuram – 603 104. Kaliyampoondi – 603 403. 11 Branch Library, 26 Branch Library, Nesco Joint, 1/172, Road Street, Kalpakkam – 603 102. Manampathi – 603 403. 12 Branch Library, 27 Branch Library, 70, Car Street, Main Road, Madhuranthagam – 603 306. Perunagar – 603 404. 13 Branch Library, 28 Branch Library, 3, Othavadai Street, Perumal Koil Street, Karunguzhi – 603 303. Salavakkam – 603 107. 14 Branch Library, 29 Branch Library, Railway Station Road, 138, Pillaiyar Koil Street, Padalam – 603 308. -

The Chennai Comprehensive Transportation Study (CCTS)
ACKNOWLEDGEMENT The consultants are grateful to Tmt. Susan Mathew, I.A.S., Addl. Chief Secretary to Govt. & Vice-Chairperson, CMDA and Thiru Dayanand Kataria, I.A.S., Member - Secretary, CMDA for the valuable support and encouragement extended to the Study. Our thanks are also due to the former Vice-Chairman, Thiru T.R. Srinivasan, I.A.S., (Retd.) and former Member-Secretary Thiru Md. Nasimuddin, I.A.S. for having given an opportunity to undertake the Chennai Comprehensive Transportation Study. The consultants also thank Thiru.Vikram Kapur, I.A.S. for the guidance and encouragement given in taking the Study forward. We place our record of sincere gratitude to the Project Management Unit of TNUDP-III in CMDA, comprising Thiru K. Kumar, Chief Planner, Thiru M. Sivashanmugam, Senior Planner, & Tmt. R. Meena, Assistant Planner for their unstinted and valuable contribution throughout the assignment. We thank Thiru C. Palanivelu, Member-Chief Planner for the guidance and support extended. The comments and suggestions of the World Bank on the stage reports are duly acknowledged. The consultants are thankful to the Steering Committee comprising the Secretaries to Govt., and Heads of Departments concerned with urban transport, chaired by Vice- Chairperson, CMDA and the Technical Committee chaired by the Chief Planner, CMDA and represented by Department of Highways, Southern Railways, Metropolitan Transport Corporation, Chennai Municipal Corporation, Chennai Port Trust, Chennai Traffic Police, Chennai Sub-urban Police, Commissionerate of Municipal Administration, IIT-Madras and the representatives of NGOs. The consultants place on record the support and cooperation extended by the officers and staff of CMDA and various project implementing organizations and the residents of Chennai, without whom the study would not have been successful. -

SNO APP.No Name Contact Address Reason 1 AP-1 K
SNO APP.No Name Contact Address Reason 1 AP-1 K. Pandeeswaran No.2/545, Then Colony, Vilampatti Post, Intercaste Marriage certificate not enclosed Sivakasi, Virudhunagar – 626 124 2 AP-2 P. Karthigai Selvi No.2/545, Then Colony, Vilampatti Post, Only one ID proof attached. Sivakasi, Virudhunagar – 626 124 3 AP-8 N. Esakkiappan No.37/45E, Nandhagopalapuram, Above age Thoothukudi – 628 002. 4 AP-25 M. Dinesh No.4/133, Kothamalai Road,Vadaku Only one ID proof attached. Street,Vadugam Post,Rasipuram Taluk, Namakkal – 637 407. 5 AP-26 K. Venkatesh No.4/47, Kettupatti, Only one ID proof attached. Dokkupodhanahalli, Dharmapuri – 636 807. 6 AP-28 P. Manipandi 1stStreet, 24thWard, Self attestation not found in the enclosures Sivaji Nagar, and photo Theni – 625 531. 7 AP-49 K. Sobanbabu No.10/4, T.K.Garden, 3rdStreet, Korukkupet, Self attestation not found in the enclosures Chennai – 600 021. and photo 8 AP-58 S. Barkavi No.168, Sivaji Nagar, Veerampattinam, Community Certificate Wrongly enclosed Pondicherry – 605 007. 9 AP-60 V.A.Kishor Kumar No.19, Thilagar nagar, Ist st, Kaladipet, Only one ID proof attached. Thiruvottiyur, Chennai -600 019 10 AP-61 D.Anbalagan No.8/171, Church Street, Only one ID proof attached. Komathimuthupuram Post, Panaiyoor(via) Changarankovil Taluk, Tirunelveli, 627 761. 11 AP-64 S. Arun kannan No. 15D, Poonga Nagar, Kaladipet, Only one ID proof attached. Thiruvottiyur, Ch – 600 019 12 AP-69 K. Lavanya Priyadharshini No, 35, A Block, Nochi Nagar, Mylapore, Only one ID proof attached. Chennai – 600 004 13 AP-70 G. -

51337-001: Tamil Nadu Industrial Connectivity Project
Resettlement Plan Document Stage: Draft January 2021 IND: Tamil Nadu Industrial Connectivity Project Chengalpattu to Kanchipuram Road (SH58) Part-I Prepared by the Project Implementation Unit (PIU), Chennai Kanyakumari Industrial Corridor, Highways Department, Government of Tamil Nadu for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 7 January 2021) Currency unit – Indian rupee/s (₹) ₹1.00 = $0. 01367 $1.00 = ₹73.1347 ABBREVIATIONS ADB – Asian Development Bank AH – Affected Household AP – Affected Person BPL – Below Poverty Line CKICP – Chennai Kanyakumari Industrial Corridor Project DC – District Collector DE – Divisional Engineer (Highways) DH – Displaced Household DP – Displaced Person SDRO – Special District Revenue Officer (Competent Authority for Land Acquisition) GOI – Government of India GRC – Grievance Redressal Committee IAY – Indira Awaas Yojana LA – Land Acquisition LARRU – Land Acquisition, Rehabilitation and Resettlement Unit LARRIC – Land Acquisition Rehabilitation & Resettlement Implementation Consultant LARRMC – Land Acquisition Rehabilitation & Resettlement Monitoring Consultant PIU – Project implementation Unit PRoW – Proposed Right-of-Way RFCTLARR – The Right to Fair Compensation and Transparency in Land Acquisition, Rehabilitation and Resettlement Act, 2013 R&R – Rehabilitation and Resettlement RF – Resettlement Framework RSO – Resettlement Officer RoW – Right-of-Way RP – Resettlement Plan SC – Scheduled Caste SH – State Highway SPS – Safeguard Policy Statement SoR – Schedule of Rate ST – Scheduled Tribe NOTE (i) The fiscal year (FY) of the Government of India ends on 31 March. FY before a calendar year denotes the year in which the fiscal year ends, e.g., FY2021 ends on 31 March 2021. (ii) In this report, "$" refers to US dollars. This draft resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. -

List of Town Panchayats Name in Tamil Nadu Page 1 District Code
List of Town Panchayats Name in Tamil Nadu Sl. No. District Code District Name Town Panchayat Name 1 1 KANCHEEPURAM ACHARAPAKKAM 2 1 KANCHEEPURAM CHITLAPAKKAM 3 1 KANCHEEPURAM EDAKALINADU 4 1 KANCHEEPURAM KARUNGUZHI 5 1 KANCHEEPURAM KUNDRATHUR 6 1 KANCHEEPURAM MADAMBAKKAM 7 1 KANCHEEPURAM MAMALLAPURAM 8 1 KANCHEEPURAM MANGADU 9 1 KANCHEEPURAM MEENAMBAKKAM 10 1 KANCHEEPURAM NANDAMBAKKAM 11 1 KANCHEEPURAM NANDIVARAM - GUDUVANCHERI 12 1 KANCHEEPURAM PALLIKARANAI 13 1 KANCHEEPURAM PEERKANKARANAI 14 1 KANCHEEPURAM PERUNGALATHUR 15 1 KANCHEEPURAM PERUNGUDI 16 1 KANCHEEPURAM SEMBAKKAM 17 1 KANCHEEPURAM SEVILIMEDU 18 1 KANCHEEPURAM SHOLINGANALLUR 19 1 KANCHEEPURAM SRIPERUMBUDUR 20 1 KANCHEEPURAM THIRUNEERMALAI 21 1 KANCHEEPURAM THIRUPORUR 22 1 KANCHEEPURAM TIRUKALUKUNDRAM 23 1 KANCHEEPURAM UTHIRAMERUR 24 1 KANCHEEPURAM WALAJABAD 25 2 TIRUVALLUR ARANI 26 2 TIRUVALLUR CHINNASEKKADU 27 2 TIRUVALLUR GUMMIDIPOONDI 28 2 TIRUVALLUR MINJUR 29 2 TIRUVALLUR NARAVARIKUPPAM 30 2 TIRUVALLUR PALLIPATTU 31 2 TIRUVALLUR PONNERI 32 2 TIRUVALLUR PORUR 33 2 TIRUVALLUR POTHATTURPETTAI 34 2 TIRUVALLUR PUZHAL 35 2 TIRUVALLUR THIRUMAZHISAI 36 2 TIRUVALLUR THIRUNINDRAVUR 37 2 TIRUVALLUR UTHUKKOTTAI Page 1 List of Town Panchayats Name in Tamil Nadu Sl. No. District Code District Name Town Panchayat Name 38 3 CUDDALORE ANNAMALAI NAGAR 39 3 CUDDALORE BHUVANAGIRI 40 3 CUDDALORE GANGAIKONDAN 41 3 CUDDALORE KATTUMANNARKOIL 42 3 CUDDALORE KILLAI 43 3 CUDDALORE KURINJIPADI 44 3 CUDDALORE LALPET 45 3 CUDDALORE MANGALAMPET 46 3 CUDDALORE MELPATTAMPAKKAM 47 3 CUDDALORE PARANGIPETTAI -
Telephone Directory
KANCHEEPURAM DISTRICT TELEPHONE DIRECTORY 2020 C THIRU.P.PONNIAH, I.A.S., DISS TRICT COLLECTOR KANCHEEPURAM KANCHEEPURAM DISTRICT HANDBOOK2020 INDEX S.NO DEPARTMENT PAGE NO 1 DISTRICT ADMINISTRATION 2 2 REVENUE DEPARTMENT 2 3 RURAL DEVELOPMENT 8 4 TOWN PANCHAYAT 10 5 MUNICIPALITY 11 6 PUBLIC WORKS DEPARTMENT 12 7 HIGHWAYS DEPARTMENT 13 8 FIRE AND RESCUE 14 9 POLICE DEPARTMENT 14 10 HEALTH DEPARTMENT 16 11 FISHERIES 20 12 ELECTRICITY DEPARTMENT 21 13 ANIMAL HUSBANDRY 22 AGRICULTURE AND ALIED 14 DEPARTMENTS 23 1 | Page KANCHEEPURAM DISTRICT HANDBOOK2020 DISTRICT ADMINISTRATION THIRU.P.PONNIAH I.A.S., 044-27238477 9444134000 DISTRICT COLLECTOR 044-27238478 SUPERINTENDENT OF POLICE 044-27237720 9443122666 044-27237424 DISTRICT REVENUE OFFICER 9445000903 044-27238955 PROJECT DIRECTOR 044-27237153 RURAL DEVELOPMENT 7373704201 044-27238651 AGENCY(DRDA) PERSONAL ASSISTANT 044-27237424 (GENERAL) 9445008138 DISTRICT LEVEL OFFICERS REVENUE DEPARTMENT REVENUE DIVISIONAL OFFICERS S.NO NAME (THIRU / TMT) DESIGNATION OFFICE-044 MOBILE 1 S.SARAVANAN, IAS., SUB COLLECTOR, 27237081 9445000413 KANCHEEPURAM 2 K.R,DIVYASHRI RDO, SRIPERUMBUDUR 27162230 9444964899 REVENUE TAHSILDARS S.NO NAME (THIRU / TMT) TALUK NAME OFFICE-044 MOBILE 1 B.BHAVANI KANCHEEPURAM - 9445000497 2 T.NIRMALA SRIPERUMBUDUR 27162231 9445000499 3 P.EGAMBARAM UTHIRAMERUR 27272230 9445000498 4 MITRA DEVI WALAJABAD 27256090 9384094643 5 D.MUTHU KUNDRATHUR 24780449 9444279499 2 | Page KANCHEEPURAM DISTRICT HANDBOOK2020 RURAL DEVELOPMENT S.NO NAME (THIRU / TMT) DESIGNATION OFFICE-044 MOBILE -

List of Polling Stations for 32 CHENGALPATTU Assembly Constituency Within the 6 KANCHIPURAM (SC) Parlimentry Constituency
List of Polling Stations for 32 CHENGALPATTU Assembly Constituency within the 6 KANCHIPURAM (SC) Parlimentry Constituency Whether for Sl No of Location and Name of the Building in which all voters or Polling Polling Area Polling station is located men only or Station women only 1. Mannivakkam (P) and Mannivakkam (RV), Ward1 East Mada St, 2. Mannivakkam (P) and Mannivakkam (RV), Ward 1 West Mada Veethi, Govt High School,Mannivakkam West Face, 1 3. Mannivakkam (P) and Mannivakkam (RV), Ward 1 North Mada St, 4. Mannivakkam (P) and Mannivakkam (RV), Ward 1 South Mada St, All Voters New Building South Part 999. OVERSEAS ELECTORS 1. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Karaipoondiyamman Koil St, 2. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Govt High School,Mannivakkam West Face, Kalaivanar St, 3. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Eswaran Koil St, 4. Mannivakkam (P) and Mannivakkam (RV), Ward1 2 All Voters New building North Part Rasathi Kalaignar Kumaran St, 5. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Sindhu Nagar, 6. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Loganathan Nagar, 7. Mannivakkam (P) and Mannivakkam (RV), Ward 1 White field, 999. OVERSEAS ELECTORS 1. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Karunanidhi KK Nagar, 2. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Indhirani PUPS,Mannivakkam South Face, Centre 3 Nagar, 3. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Ambedkar Nagar, 4. Mannivakkam (P) and Mannivakkam (RV), Ward 1 All Voters Building East Part Singaram Nagar, 999. OVERSEAS ELECTORS 1. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Kumaran Nagar, 2. Mannivakkam (P) and Mannivakkam (RV), Ward 1 Kalaignar Karunanidhi St, 3. -

Kancheepuram District Map
KANCHEEPURAM DISTRICT MAP TIRUVALLUR THIRUVALLUR KONDAVAKKAM CHENNAI AYYAPANTHANGAL DISTRICT KANDAMANGALAM CHENNAI THELLIARAGARAM CHENNAI MEVALURCUPPAM MANGADU SRINIVASAPURAM MANGADU T.P KOLATHUVANJERI SENGADU MANNUR KOZHIMANIVAKKAM CHENNAI CHINNA- MOWLIVAKKAM DISTRICT SIVABURAM MALAYAMBAKKAMPANICHERI PARANIPUTHUR VALARPURAM PERIA- ORAGADAMAHADEVINANGALAM PANICHER CHEMBARAMBAKKAM TANK SIKKARAYAPURAM KOVUR GERUGAMBAKKAM KAPPANKOTTUR THANDALAM KOLACHERY KUNNATHUR bit2 KOLAPAKKAM MOONRAM- PICHIVAKKAM THANDALAM KOLAPAKKAM THIRUNAGESWARAM KATTALAI NEMEMLI THANDALAM UDUPPAIR KANDIVAKKAM ELIMIANKDTTUR R.F SIRUKALATHUR KAVANUR RENDANKATTALAI VENKATEPURAM IRUNGATTUKOTTAI THARAPPAKKAM KOTTUR MANANJERI THOLASAPURAM THARVUR KILOY AYAKOLATHUR KUNDRATHUR PURISAI EDAYARPAKKAM KATTRAMBAKKAM GUNAGARABAKKAM ETTIKUTHIMEDU NANDAMBAKKAM KUNDRATHUR PENNALUR SIRUKILOY KANAGAMBAKKAM THANDALAM AKKAMAPURAM MAHADEVIMANGALAM PUDUPPAIR PADICHERY SRIPERUMBUDUR KANNANTHANGAL POONTHANDALAM THIRUMUDIVAKKAM PULLALORE PALLAMBAKKAM SRIPERUMBUDUR AMARAMBEDU R.F ARAKONAM VALATHUR EKANAPURAM PALANTHANDALAM RANIPET NALLUR SINGLEPADI VADAMANGALAM VENGADU NALLUR PADUNALLI PONDAVAKKAM MADURAMANGALAM R.F MOOLAPATTU MADURAMANGALM IRUNBEDU DISTRICT ERUMAYUR KOTTAVAKKAM KODAMANALLUR KANDUR PILLAIPPAKKAM PUDUCHERI SOMANGALAM SOGANDI NAVALUR GOVINDAVADI MANIYATCHI IRUNGULAM KOLATHUR NADUVEERAPPATTU PARANDUR KARUNAGARACHRI PUTHERI THANDALAM MELMADURAMAGALAM MOLASUR NELVOY THIRUMANGALAM KUNDRATHUR UVERI KEERANALLUR NANDIMEDU GOVINDAVADI PARANDUR SIVANKUDAL MAMBAKKAM PONDUR MALAIPPATTU -

Vulnerable Areas - 2018 Abstract
Vulnerable Areas - 2018 Abstract Areas (Rural & Urban) Very High High Medium Low Total Rural - Taluk Firka Level 44 66 119 54 283 Urban - Municipality 15 44 39 36 134 Urban - Town Panchayat 25 39 8 26 98 Total 84 149 166 116 515 Name of the District :KANCHEEPURAM Rural Development Name of the Source of S.No Name of the Taluk Name of the Firka Vulnerable Areas Latitude Longitude Relife Center Panchayat Vulnerable Panchayat Union 1 madurantagam orathi Acharapakkam Low Kalathur 12.40352 79.81567 Primary School, Kalathur Panchayat Union 2 madurantagam orathi Acharapakkam Low Vadamanipakkam 12.35885 79.68494 Primary School, Ettipattu Panchayat Union 3 madurantagam orathi Acharapakkam High Veliampakkam 12.40352 79.81567 Primary School, Veliampakkam Panchayat Union 4 madurantagam orathi Acharapakkam Low Sirudamur 12.40352 79.81567 Primary School, Sirudamur Panchayat Union 5 madurantagam Acharapakkam Acharapakkam Medium Seetapuram 12.40352 79.81567 Primary School, Seetapuram Panchayat Union 6 madurantagam Acharapakkam Acharapakkam Medium Elapakkam (R.C. Nagar) 12.40352 79.81567 Primary School, Elapakkam Venkatesapuram 7 madurantagam Acharapakkam Acharapakkam Medium Pallipettai 12.43125 79.83370 Middle School Community Hall, 8 madurantagam Acharapakkam Acharapakkam Medium Minnalkilminal 12.40352 79.81567 Killpattu Higher Secondary 9 madurantagam L.Endathur Acharapakkam Medium L.Endathur 12.51932 79.77223 School, L-Endathur Panchayat Union 10 madurantagam L.Endathur Acharapakkam Medium Pappanallur Colony, 12.40352 79.81567 Primary School, Pappanallur -
Chennai Sl.No
CHENNAI SL.NO. APPLICATION NO. NAME AND ADDRESS NIXON ANTONY RAJ. J NO;17/1098, 12TH STREET, 1 5001 POOMBUKAR NAGAR, CHENNAI 600099 MAHENDRA. V NO.9/71, 5TH STREET, 2 5002 KAMARAJ NAGAR, KORUKKUPET, CHENNAI 600021 HEMABALA. J NO.4/34, 6TH STREET, 3 5003 RAJIV GANDHI NAGAR, CRPF, AVADI, CHENNAI 600065 KAMALA KANNAN. M S/O MOORTHY . M NO.750, L.I.G.I., 4 5004 T.N.H.B. AYYAPPAKKAM , TIRUVALLUR DST. CHENNAI 600077 SETHURAMAN.N NO.6/7A,17TH STREET, 5 5005 JAI NAGAR, ARUMBAKKAM, CHENNAI 600106 ANANDHA KUMAR.B NO.11, 11TH ST, 6 5006 MOONGIL EARI, PALLAVARAM, CHENNAI 600043 VELMUTHU.A NO.7, NETHAJI NAGAR, NCTPS POST, 7 5007 A.R.S.CROSS ROAD, MINJUR SPL, CHENNAI 600120 JOTHI. H 11A, MUGUNTHA RAMANUIAM STREET, 8 5008 MADUMANAGAR, PERAMBUR, CHENNAI 600011 DEEPAN. T NO.1/5A, VINAYAGAPURAM, 9 5009 VADAPERUM PAKKAM, THIRUVALLUR 600060 Page 1 KAVITHA. R D/O RAJAPPA. S.J NO.2/11, 10 5010 SRINIVASA IYANGAR, IST STREET, WEST MAMBALAM, CHENNAI 600033 PANDIAN. S S/O WAMIDASS.S NO.29, OLD NO.13, 11 5011 37TH STREET, PUNITHA ANTHONIYAR STREET, GKM COLONY, CHENNAI 600082 KARTHIKEYAN. M.A S/O ARUMUGAM. M UVAPARTMENT SECOND FLOOR- 3, 12 5012 NO.7, SRINIVASAN , LIC COLONY EXTN, PAMMAL, CHENNAI 600075 RAMA KRISHNAN .R S/O RAJAMANICKAM NO.16, KASTHURI NAGAR, 13 5013 ACHARAPAAKKAM & POST, MADURANTAHKAM(TALUK), KANCHIPURAM 603301 SAKTHI.M D/O MUTHAN 4/821 A, VENKETESHPURAM, 14 5014 AJANTHA AVENUE, KOTTAIVAKKAM, CHENNAI 600041 DILLI.L S/O LAKSHMANAN. E NO.20/23,VINAYAGAR KOIL ST, 15 5015 KORATTUR, THIRUVALLUR, CHENNAI 600080 AROKIYA SAMY. -

Club Health Assessment MBR0087
Club Health Assessment for District 324A1 through April 2021 Status Membership Reports Finance LCIF Current YTD YTD YTD YTD Member Avg. length Months Yrs. Since Months Donations Member Members Members Net Net Count 12 of service Since Last President Vice Since Last for current Club Club Charter Count Added Dropped Growth Growth% Months for dropped Last Officer Rotation President Activity Account Fiscal Number Name Date Ago members MMR *** Report Reported Report *** Balance Year **** Number of times If below If net loss If no When Number Notes the If no report on status quo 15 is greater report in 3 more than of officers thatin 12 months within last members than 20% months one year repeat do not haveappears in two years appears appears appears in appears in terms an active red Clubs less than two years old 139250 Chennai Aram Seiyya Virumbu 07/22/2019 Active 33 10 4 6 22.22% 27 1 0 N T,SC 1 143813 Chennai Dynamics 12/07/2020 Active 26 26 0 26 100.00% 0 0 N M 0 $1,000.86 142068 Chennai Golden Hands 07/07/2020 Active 27 28 1 27 100.00% 0 0 0 N S,M 0 $256.89 139930 Chennai Gopalapuram 09/29/2019 Active 16 0 0 0 0.00% 23 10 M,VP,MC,SC N/R $1,009.86 143654 Chennai Green Fields 11/19/2020 Active 22 22 0 22 100.00% 0 5 N VP N/R 144902 Chennai Motherland Friends 01/18/2021 Active 35 35 0 35 100.00% 0 0 N N/R $0.82 142088 Chennai Power House 07/07/2020 Active 26 26 0 26 100.00% 0 1 N 1 141534 Chennai Reinforce 05/29/2020 Active 58 38 5 33 132.00% 0 5 1 2 N M 2 90+ Days 144987 Chennai Rockers 02/11/2021 Newly 45 45 0 45 100.00% 0 0 N 1 Chartered