2021 E/M Updates: What Will Happen to the Physician Note
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cardiovascular Assessment
Cardiovascular Assessment A Home study Course Offered by Nurses Research Publications P.O. Box 480 Hayward CA 94543-0480 Office: 510-888-9070 Fax: 510-537-3434 No unauthorized duplication photocopying of this course is permitted Editor: Nurses Research 1 HOW TO USE THIS COURSE Thank you for choosing Nurses Research Publication home study for your continuing education. This course may be completed as rapidly as you desire. However there is a one-year maximum time limit. If you have downloaded this course from our website you will need to log back on to pay and complete your test. After you submit your test for grading you will be asked to complete a course evaluation and then your certificate of completion will appear on your screen for you to print and keep for your records. Satisfactory completion of the examination requires a passing score of at least 70%. No part of this course may be copied or circulated under copyright law. Instructions: 1. Read the course objectives. 2. Read and study the course. 3. Log back onto our website to pay and take the test. If you have already paid for the course you will be asked to login using the username and password you selected when you registered for the course. 4. When you are satisfied that the answers are correct click grade test. 5. Complete the evaluation. 6. Print your certificate of completion. If you have a procedural question or “nursing” question regarding the materials, call (510) 888-9070 for assistance. Only instructors or our director may answer a nursing question about the test. -
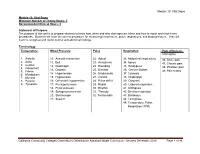
Module 10: Vital Signs
Module 10: Vital Signs Module 10: Vital Signs Minimum Number of Theory Hours: 3 Recommended Clinical Hours: 6 Statement of Purpose: The purpose of this unit is to prepare students to know how, when and why vital signs are taken and how to report and chart these procedures. Students will learn the correct procedure for measuring temperature, pulse, respirations, and blood pressure. They will learn to recognize and report normal and abnormal findings. Terminology: Temperature: Blood Pressure Pulse Respiration Pain (effects on Vital signs) 1. Afebrile 10. Aneroid manometer 22. Apical 33. Abdominal respirations 46. Acute pain 2. Axilla 11. Bell 23. Arrhythmia 34. Apnea 47. Chronic pain 3. Celsius 12. Diaphragm 24. Bounding 35. Bradypnea 4. Fahrenheit 48. Phantom pain 13. Diastolic 25. Brachial 36. Cheyne-Stokes 5. Febrile 49. Pain scales 6. Metabolism 14. Hypertension 26. Bradycardia 37. Cyanosis 7. Mucosa 15. Hypotension 27. Carotid 38. Diaphragm 8. Pyrexia 16. Orthostatic hypotension 28. Pulse deficit 39. Dyspnea 9. Tympanic 17. Pre-hypertension 29. Radial 40. Labored respiration 18. Pulse pressure 30. Rhythm 41. Orthopnea 19. Sphygmomanometer 31. Thready 42. Shallow respiration 20. Stethoscope 32. Tachycardia 43. Stertorous 21. Systolic 44. Tachypnea 45. Temperature, Pulse, Respiration (TPR) Patient, patient/resident, and client are synonymous terms Californiareferring to Community the person Colleges Chancellor’s Office Nurse Assistant Model Curriculum - Revised December 2018 Page 1 of 46 receiving care Module 10: Vital Signs Patient, resident, and client are synonymous terms referring to the person receiving care Performance Standards (Objectives): Upon completion of three (3) hours of class plus homework assignments and six (6) hours of clinical experience, the student will be able to: 1. -

Mod. 3 Vital Signs
Mod. 3 Vital Signs 1. What is most important to assess during secondary assessment? a. Airway b. Pulse c. Respiration d. Chief complaint 2. The first set of vital sign measurements obtained are often referred to as which of the following? a. Baseline vital signs b. Normal vital signs c. Standard vital signs d. None of the above 3. A patient with a pulse rate of 120 beats per minute is considered which of the following? a. Dyscardic b. Normocardic c. Tachycardic d. Bradycardic 4. Where do baseline vital signs fit into the sequence of patient assessment? a. Ongoing assessment b. At primary assessment c. At secondary assessment d. At the patient's side 5. In a conscious adult patient, which of the following pulses should be assessed initially? a. Brachial b. Radial c. Carotid d. Pedal 6. You are assessing a 55-year-old male complaining of chest pain and have determined that his radial pulse is barely palpable. You also determine that there were 20 pulsations over a span of 30 seconds. Based on this, how would you report this patient's pulse? a. Pulse 20, weak, and regular b. Pulse 20 and weak c. Pulse 40 and weak d. Pulse 40, weak, and irregular 7. Which of the following are the vital signs that need to be recorded? a. Pulse, respiration, skin color, skin temperature and condition b. Pulse, respiration, skin color, skin temperature and condition, pupils, blood pressure, and bowel sounds c. Pulse, respiration, skin color, skin temperature and condition, pupils, and blood pressure d. Pulse, respiration, skin color, skin temperature, pupils, and blood pressure 8. -

Coding Tips For: PROGRESS NOTE CONTENTS
Coding tips for: PROGRESS NOTE CONTENTS PREFERRED FORMAT, PER CMS, IS THE S.O.A.P. FORMAT: SUBJECTIVE: This section should be utilized to report subjective information of clinical significance. The chief complaint of the patient belongs in this section. OBJECTIVE: This section is where you will report the measurable and observable information that you obtain during the visit. Review of systems, physical examination, any test results, outside communications with specialists should be noted in this section. ASSESSMENT: List all diagnoses and conditions assessed during the visit. Include any conditions for which prescriptions were given/renewed, tests were ordered, referrals were given. Also include any conditions in which affected decision-making for treatment. PLAN: The final section of your SOAP notes is where you outline the course of treatment, after considering the information you gathered during the visit. e text box anywhere in the document. Use the Text Box Tools tab to change the formatting of the pull quote text box.] Coding tips for: ASSURE PROGRESS NOTE COMPLIANCE The physician’s signature must be on all progress notes If the physician does not include his/her credentials as part of their signature, the full name and credentials must be printed clearly on the note The patient’s name, date of birth and DOS must be on each page of the patient’s progress note/chart Electronic Medical Records must clearly be “authenticated", “digitally signed”, “electronically signed by” the provider The medical record must be legible/complete Only standard medical abbreviations should be used Late entries can be made to clarify confirmed diagnoses. -

Medical Terminology Information Sheet
Medical Terminology Information Sheet: Medical Chart Organization: • Demographics and insurance • Flow sheets • Physician Orders Medical History Terms: • Visit notes • CC Chief Complaint of Patient • Laboratory results • HPI History of Present Illness • Radiology results • ROS Review of Systems • Consultant notes • PMHx Past Medical History • Other communications • PSHx Past Surgical History • SHx & FHx Social & Family History Types of Patient Encounter Notes: • Medications and medication allergies • History and Physical • NKDA = no known drug allergies o PE Physical Exam o Lab Laboratory Studies Physical Examination Terms: o Radiology • PE= Physical Exam y x-rays • (+) = present y CT and MRI scans • (-) = Ф = negative or absent y ultrasounds • nl = normal o Assessment- Dx (diagnosis) or • wnl = within normal limits DDx (differential diagnosis) if diagnosis is unclear o R/O = rule out (if diagnosis is Laboratory Terminology: unclear) • CBC = complete blood count o Plan- Further tests, • Chem 7 (or Chem 8, 14, 20) = consultations, treatment, chemistry panels of 7,8,14,or 20 recommendations chemistry tests • The “SOAP” Note • BMP = basic Metabolic Panel o S = Subjective (what the • CMP = complete Metabolic Panel patient tells you) • LFTs = liver function tests o O = Objective (info from PE, • ABG = arterial blood gas labs, radiology) • UA = urine analysis o A = Assessment (Dx and DDx) • HbA1C= diabetes blood test o P = Plan (treatment, further tests, etc.) • Discharge Summary o Narrative in format o Summarizes the events of a hospital stay -
The AOA Guide
The AOA Guide: How to Succeed in the Third-Year Clerkships Example Notes for the MSIII 2014 Preface This guide was created as a way of assisting you as you start your clinical training. For the rest of your professional life you will write various notes, and although they eventually become second nature to you, it is often challenging at first to figure out what information is pertinent to a particular specialty/rotation.This book is designed to help you through that process. In this book you will find samples of SOAP notes for each specialty and a complete History and Physical. Each of these notes represents very typical patients you will see on the rotation. Look at the way the notes are phrased and the information they contain. We have included an abbreviations page at the end of this book so that you can refer to it for the short-forms with which you are not yet familiar. Pretty soon you will be using these abbreviations without a problem! These notes can be used as a template from which you can adjust the information to apply to your patient. It is important to remember that these notes are not all inclusive, of course, and other physicians will give suggestions that you should heed. If you are having trouble, remember there is usually a fourth year medical student on the rotation somewhere, too. We are always willing to help! Table of Contents Internal Medicine Progress Note (SOAP) ............................................................3 Neurology Progress Note (SOAP) ....................................................................... 5 Surgery ................................................................................................................. 7 Progress Note (SOAP) .................................................................................... 7 Pre-Operative Note ........................................................................................ -

EHR Go Guide: the Notes Tab
EHR Go Guide: The Notes Tab Introduction The Notes tab in the EHR contains narrative information about a patient’s current and past medical history. It is where all members of the health care team communicate about the patient during a hospital visit or while receiving outpatient care. Notes are documented on regular intervals about clinical events related to the diagnoses and treatment of the patient. There are many types of notes in the EHR including: admission notes, assessments, SOAP notes, exams, reports, screening tools, progress notes, evaluations, and more. Notes are sometimes referred to as “Flow Sheets.” Most note options are templated, meaning specific fields or questions are built in to the note for the clinician to answer, while other notes allow for free-text narrative entry. Case patients in EHR Go have existing notes in their chart. You may review these notes to gather detailed information about the patient’s condition. It is often helpful to review the patient’s notes first, to learn about the patient, before reviewing the information in the other EHR tabs. In some activities, you’ll need to write a new note. This guide explains how to access and review existing notes, edit notes, and create new notes. Additional resources Please refer to the Student Guide to EHR Go for information on logging in to Go and launching the EHR for an activity. FAQs about notes 1. Can I edit a note after I have finished it? a. Yes. In EHR Go, you may edit any existing note as often as needed. See Editing a Note section. -

History & Physical Format
History & Physical Format SUBJECTIVE (History) Identification name, address, tel.#, DOB, informant, referring provider CC (chief complaint) list of symptoms & duration. reason for seeking care HPI (history of present illness) - PQRST Provocative/palliative - precipitating/relieving Quality/quantity - character Region - location/radiation Severity - constant/intermittent Timing - onset/frequency/duration PMH (past medical /surgical history) general health, weight loss, hepatitis, rheumatic fever, mono, flu, arthritis, Ca, gout, asthma/COPD, pneumonia, thyroid dx, blood dyscrasias, ASCVD, HTN, UTIs, DM, seizures, operations, injuries, PUD/GERD, hospitalizations, psych hx Allergies Meds (Rx & OTC) SH (social history) birthplace, residence, education, occupation, marital status, ETOH, smoking, drugs, etc., sexual activity - MEN, WOMEN or BOTH CAGE Review Ever Feel Need to CUT DOWN Ever Felt ANNOYED by criticism of drinking Ever Had GUILTY Feelings Ever Taken Morning EYE OPENER FH (family history) age & cause of death of relatives' family diseases (CAD, CA, DM, psych) SUBJECTIVE (Review of Systems) skin, hair, nails - lesions, rashes, pruritis, changes in moles; change in distribution; lymph nodes - enlargement, pain bones , joints muscles - fractures, pain, stiffness, weakness, atrophy blood - anemia, bruising head - H/A, trauma, vertigo, syncope, seizures, memory eyes- visual loss, diplopia, trauma, inflammation glasses ears - deafness, tinnitis, discharge, pain nose - discharge, obstruction, epistaxis mouth - sores, gingival bleeding, teeth, -

Progress Notes and Psychotherapy Notes
Progress Notes and Psychotherapy Notes This Appendix covers two kinds of notes written about psychotherapy—progress notes and psychotherapy notes—and highlights the practical value of this important distinction. Progress notes are part of the client record or file, as noted below. Psychotherapy notes are not part of the file. After an overview of the client file or record, the difference between these two kinds of notes is discussed along with guides for writing progress notes. The Client File or Record The record or file of a client’s treatment at the Clinic consists of: Contact information Informed consent for treatment (including notification of rights) An intake report and/or, A written treatment plan or case formulation based on an initial assessment (i.e. interview information, formal assessment if used, and any other information collected from other sources) Progress notes documenting treatment, filed in reverse chronological order on the Clinic form Progress Note A termination note when work is concluded Other materials such as releases of information, test protocols, information obtained from other sources and so forth. The file or record does not contain psychotherapy notes (see below). Another way of saying this is that if it’s in the file, it’s not a psychotherapy note. As context for progress notes versus psychotherapy notes, please also refer to the form in Appendix D Brief Summary of Client Rights to Privacy and Access to Records and Consent to Behavioral Health Treatment and to the document in that appendix entitled Protecting the Privacy of Your Behavioral Health Information. A general intake outline is contained in Appendix C-4 Intake Outline and Report which can serve to organize information and begin treatment planning. -

Setting up a Progress Note in Ecw 11 for Medical Assistants
Setting Up a Progress Note in ECW 11 In this document, I will explain how to set up a progress note in ECW 11. When the visit is first opened, ECW asks if the medications should be carried into the note – the answer is always “Yes”. If there are any errors in the medication list from prior encounters, they will be pulled into this note as well, which is why reconciling medications is one of the most important steps in setting up a note properly. We start with the basic framework of a SOAP note. The chief complaint is pulled from the schedule - when this appointment was made, someone entered a reason, and this is pulled in as the chief complaint. The next step in most offices is to add a template to the note. At the bottom of the progress note is a panel of options. Clicking on the “Template” button opens the template screen. The current filter in the template screen is “Generic” and “All”. Once you set up your favorites, it will be much easier to quickly locate the template you wish to use by selecting “My Favorites” rather than “All” as a filter. When you find a template you like, click on “Add As Favorite” and this template will be added to your template favorites. Clicking on the magnifying glass will open a view of the template, allowing you to see what you are importing into the note. The panel at the right shows you which sections of the template will be added to the note. -
PAOD Testing in Diabetic Patients
This Just In Susan Simmons Holcomb, PhD, ARNP, BC This Just In Editor PAOD Testing in Diabetic Patients Diabetes mellitus is a major risk factor for lower extremity amputa- identify the disease and initiate factor for the development of car- tion and yet, to date, there are no treatment quickly. diovascular disease, including pe- guidelines for the prevention, identi- ripheral arterial occlusive disease fication, and treatment of PAOD in ■ Identifying PAOD (PAOD) or peripheral arterial dis- diabetic patients. Twenty percent of In the past, identification of PAOD ease. Approximately 20% of the 12 diabetic patients older than 40 years was done by clinically analyzing re- million Americans identified in the of age have PAOD and 29% of dia- ported symptoms of claudication or Framingham Heart Study as having betic patients over 50 years of age absence of palpable peripheral symptomatic PAOD were diabetics.1 have PAOD. Twenty-seven percent of pulses. However, these methods are However, this estimate may be low. diabetic patients with PAOD will insensitive and may not identify pa- tients early enough. A more sensitive test is the ankle-brachial index Nurse practitioners must be able to identify PAOD and (ABI). The ABI is obtained by mea- initiate treatment quickly. suring systolic blood pressures in the ankles and arms via a Doppler and then calculating a ratio between the Experts believe over one-half of dia- have disease progression within 5 two. When compared to angiograph- betic patients with PAOD are years; 4% of those patients will re- ically determined arterial disease, asymptomatic, approximately one- quire amputation, and 20% will ex- measuring ABI is 95% sensitive and third have claudication, and the re- perience nonfatal cardiovascular almost 100% specific.1 However, maining patients have extremely events such as myocardial infarction sensitivity decreases in the elderly severe symptomatic disease. -

Consortium of Operative Dentistry Educators (CODE) REGIONAL
Consortium of Operative Dentistry Educators (CODE) REGIONAL REPORTS FALL 2014 Web site: http://www.unmc.edu/code 1 TABLE OF CONTENTS Foreward......................................................................................................................................... 5 Origins of CODE ........................................................................................................................... 5 Organization Operation ................................................................................................................ 7 CODE Advisory Committee ......................................................................................................... 8 Regions and Schools ..................................................................................................................... 8 2014 Agenda .................................................................................................................................10 CODE Regional Meeting Report Form ........................................................................................15 CODE Regional Attendees Form .................................................................................................17 Regional Reports: Region I (Pacific) ..........................................................................................................18 Region II (Midwest) ......................................................................................................50 Region III (South Midwest) ..........................................................................................75