Allergies in Children
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Caring for Children with Special Needs ALLERGIES and ASTHMA
caring for children with special needs ALLERGIES AND ASTHMA We don’t usually think of children with allergies or asthma as children with “special needs,” but they certainly are. In fact, children with these conditions are probably the most frequently encountered “special needs” children. Child care providers can do a great deal to help individual children manage their specific allergy or asthma needs and feel more comfortable in a child care setting. Allergies wastes. Every house has them, no matter how clean. Other inhaled Children with allergies face the allergens include mold, pollen (hay same social difficulties as do adults, fever), animal dander (especially but they have less maturity and from cats), chemicals, and per emotional resources to deal with fumes. them. Children find that they cannot eat what their friends eat or The most common allergy symp cannot play outside during some toms are seasons. Until a child is mature � a clear, runny nose and enough to understand why she sneezing, cannot do something, you must be � itchy or stuffed-up nose or careful to help the child through the itchy, runny eyes, and difficulties. Start teaching a child early on about what he is allergic to; � asthma (remember that not all you will not always be able to people with asthma have monitor everything. allergies and not all allergies Some foods can cause a life cause or develop into asthma). threatening reaction. The mouth, throat, and bronchial tubes swell enough to interfere with breathing. Strategies for inclusion The person may wheeze or faint. Some parents have found that by Often there are generalized hives volunteering to bring food to and/or a swollen face. -

Differentiating Between Anxiety, Syncope & Anaphylaxis
Differentiating between anxiety, syncope & anaphylaxis Dr. Réka Gustafson Medical Health Officer Vancouver Coastal Health Introduction Anaphylaxis is a rare but much feared side-effect of vaccination. Most vaccine providers will never see a case of true anaphylaxis due to vaccination, but need to be prepared to diagnose and respond to this medical emergency. Since anaphylaxis is so rare, most of us rely on guidelines to assist us in assessment and response. Due to the highly variable presentation, and absence of clinical trials, guidelines are by necessity often vague and very conservative. Guidelines are no substitute for good clinical judgment. Anaphylaxis Guidelines • “Anaphylaxis is a potentially life-threatening IgE mediated allergic reaction” – How many people die or have died from anaphylaxis after immunization? Can we predict who is likely to die from anaphylaxis? • “Anaphylaxis is one of the rarer events reported in the post-marketing surveillance” – How rare? Will I or my colleagues ever see a case? • “Changes develop over several minutes” – What is “several”? 1, 2, 10, 20 minutes? • “Even when there are mild symptoms initially, there is a potential for progression to a severe and even irreversible outcome” – Do I park my clinical judgment at the door? What do I look for in my clinical assessment? • “Fatalities during anaphylaxis usually result from delayed administration of epinephrine and from severe cardiac and respiratory complications. “ – What is delayed? How much time do I have? What is anaphylaxis? •an acute, potentially -

Symptoms Related to Asthma and Chronic Bronchitis in Three Areas of Sweden
Eur Respir J, 1994, 7, 2146–2153 Copyright ERS Journals Ltd 1994 DOI: 10.1183/09031936.94.07122146 European Respiratory Journal Printed in UK - all rights reserved ISSN 0903 - 1936 Symptoms related to asthma and chronic bronchitis in three areas of Sweden E. Björnsson*, P. Plaschke**, E. Norrman+, C. Janson*, B. Lundbäck+, A. Rosenhall+, N. Lindholm**, L. Rosenhall+, E. Berglund++, G. Boman* Symptoms related to asthma and chronic bronchitis in three areas of Sweden. E. Björnsson, *Dept of Lung Medicine and Asthma P. Plaschke, E. Norrman, C. Janson, B. Lundbäck, A. Rosenhall, N. Lindholm, L. Research Center, Akademiska sjukhu- Rosenhall, E. Berglund, G. Boman. ERS Journals Ltd 1994. set, Uppsala University, Uppsala, Sweden. ABSTRACT: Does the prevalence of respiratory symptoms differ between regions? **Asthma and Allergy Research Center, Sahlgren's Hospital, University of Göteborg, As a part of the European Community Respiratory Health Survey, we present data Göteborg, Sweden. +Dept of Pulmonary from an international questionnaire on asthma symptoms occurring during a 12 Medicine and Allergology, Univer- month period, smoking and symptoms of chronic bronchitis. The questionnaire was sity Hospital of Northern Sweden, Umeå, mailed to 10,800 persons aged 20–44 yrs living in three regions of Sweden (Västerbotten, Sweden. ++Dept of Pulmonary Medicine, Uppsala and Göteborg) with different environmental characteristics. The total Sahlgrenska University Hospital, Göteborg, response rate was 86%. Sweden. Wheezing was reported by 20.5%, and the combination of wheezing without a Correspondence: E. Björnsson, Dept of cold and wheezing with breathlessness by 7.4%. The use of asthma medication was Lung Medicine, Akademiska sjukhuset, S- reported by 5.3%. -

Pediatric Clerkship Manual Se Campus-Fargo
PEDIATRIC CLERKSHIP MANUAL SE CAMPUS-FARGO 1 | P a g e Table of Contents Curriculum and Objectives 3 Introduction-Inpatient, Outpatient, Subsp. Clinic, NNN, CTC 4 Pediatric Clerkship Requirements 9 Inpatient H&P Outline 10 Inpatient Progress Note Outline 17 Outpatient Write-Up Outline 19 Oral Case Primer 21 Oral Case Template 33 Professor Rounds – OPCRS Rating For m 35 Midclerkship Feedback 39 Aquifer Pediatrics/Radiology (CLIPP/CORE) Cases 40 Pediatric Grand Rounds 40 Grading Policy and Honors Designation Guidelines 42 2 | P a g e PEDIATRIC CLERKSHIP UND SCHOOL OF MEDICINE AND HEALTH SCIENCES SOUTHEAST CAMPUS – FARGO Welcome to the 3rd year Pediatric Clerkship where “The care of children is the finest privilege!” We hope that your eight-week experience in Pediatrics will provide you with a broad and exciting introduction to the care of infants, children, and adolescents. While rotating through Pediatrics, you will have the opportunity to work as part of a team comprised of community attending physicians, nurses, and paramedical personnel. Our commitment to you: The faculty of the Southeast Campus is composed of volunteer faculty pediatricians under the leadership of Dr. Chris DeCock, pediatric clerkship director. You will be provided prompt feedback to ensure you to optimize your learning experience on Pediatrics. We expect that as third year medical students you come to the Pediatric Clerkship prepared to give 100% to each patient encounter. We also expect you will conduct yourself in a professional manner. If you have any concerns or problems during your rotation feel free to contact Dr. Chris DeCock, pediatric clerkship director or Kathy Kraft, clerkship coordinator. -

Pediatric Institute & Cleveland Clinic Children's
Pediatric Institute & Cleveland Clinic Children’s This project would not have been possible without the commitment and expertise of a team led by Dr. Vera Hupertz, Anne Shi, and Allan Cohn. Graphic design and photography were provided by Cleveland Clinic’s Center for Medical Art and Photography. © The Cleveland Clinic Foundation 2017 9500 Euclid Avenue, Cleveland, OH 44195 clevelandclinic.org 2016 Outcomes 17-OUT-420 108373_CCFBCH_17OUT420_ACG.indd 1-3 9/7/17 1:42 PM Measuring Outcomes Promotes Quality Improvement Clinical Trials Cleveland Clinic is running more than 2200 clinical trials at any given time for conditions including breast and liver cancer, coronary artery disease, heart failure, epilepsy, Parkinson disease, chronic obstructive pulmonary disease, asthma, high blood pressure, diabetes, depression, and eating disorders. Cancer Clinical Trials is a mobile app that provides information on the more than 200 active clinical trials available to cancer patients at Cleveland Clinic. clevelandclinic.org/cancertrialapp Healthcare Executive Education Cleveland Clinic has programs to share its expertise in operating a successful major medical center. The Executive Visitors’ Program is an intensive, 3-day behind-the-scenes view of the Cleveland Clinic organization for the busy executive. The Samson Global Leadership Academy is a 2-week immersion in challenges of leadership, management, and innovation taught by Cleveland Clinic leaders, administrators, and clinicians. Curriculum includes coaching and a personalized 3-year leadership development plan. clevelandclinic.org/executiveeducation Consult QD Physician Blog A website from Cleveland Clinic for physicians and healthcare professionals. Discover the latest research insights, innovations, treatment trends, and more for all specialties. consultqd.clevelandclinic.org Social Media Cleveland Clinic uses social media to help caregivers everywhere provide better patient care. -

Clinical Pharmacists' Role in Paediatric Patients' Medical Care
International Journal of Contemporary Pediatrics Balakrishnan RP et al. Int J Contemp Pediatr. 2020 Dec;7(12):2416-2420 http://www.ijpediatrics.com pISSN 2349-3283 | eISSN 2349-3291 DOI: https://dx.doi.org/10.18203/2349-3291.ijcp20205110 Review Article Clinical pharmacists’ role in paediatric patients’ medical care Raveena Pachal Balakrishnan1*, Rajganesh Ravichandran1, Jaya Shree Dillibatcha1, Abrana Lakshmi Ravi1, Nikhil Cherian Sam1, Ramya Nuthalapati2 1Department of Pharmacy Practice, C. L. Baid Metha college of Pharmacy, The Tamil Nadu Dr. M. G. R. Medical University, Chennai, Tamil Nadu, India 2Clinical Pharmacist, Gleneagles Global Health City, Perumbakkam, Chennai Tamil Nadu, India Received: 11 October 2020 Accepted: 13 November 2020 *Correspondence: Dr, Raveena Pachal Balakrishnan, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Clinical pharmacists give valuable administrations to adult patients, however, their advantages for pediatric and neonatal patients are less characterized. Many studies state that medication errors in children are more common than in adults with a greater risk of death.Clinical Pharmacists are accepted as the primary source for providing evidence-based information and advice, to ensure the delivery of correct, safest, and most effective medication to patients. This paper presents a review of the role of clinical pharmacists in the pediatric unit and emphasis the importance of clinical pharmacists for all patients, especially in the pediatric age group. -

Download WAO White Book on Allergy
WORLD ALLERGY ORGANIZATION WAWAOO WhiteWhite BookBook onon AllergyAllergy WAO White Book on Allergy World Allergy Organization (WAO) White Book on Allergy Copyright 2011 World Allergy Organization WAO White Book on Allergy Editors Prof. Ruby Pawankar, MD, PhD Prof. Giorgio Walter Canonica, MD WAO President Elect (2010-2011) WAO Past President (2010-2011) Allergy and Rhinology Allergy & Respiratory Diseases Nippon Medical School Department of Internal Medicine 1-1-5 Sendagi, Bunkyo-ku University of Genoa Tokyo 113-8603 Padiglione Maragliano, Largo Rosanna Benzi 10 JAPAN 1-16132 Genoa ITALY Prof. Stephen T. Holgate, BSc, MD, DSc, FMed Sci Prof. Richard F. Lockey, MD Member, WAO Board of Directors (2010-2011) WAO President (2010-2011) Medical Research Council Clinical Professor of Division of Allergy & Immunology Immunopharmacology Joy McCann Culverhouse Chair in Allergy & Immunology Infection, Inflammation and Immunity University of South Florida College of Medicine School of Medicine James Haley Veterans Administration Medical Center (111D) University of Southampton 13000 Bruce B. Downs Boulevard Level F, South Block Tampa, Florida 33612 Southampton General Hospital USA Tremona Road Southampton SO16 6YD United Kingdom Acknowledgement On behalf of the World Allergy Organization (WAO), the editors and authors of the WAO White Book on Allergy express their gratitude to the charity, Asthma, Allergy, Inflammation Research (AAIR) and Asian Allergy Asthma Foundation (AAAF) for their support in the production of this publication. The Editors of the White book extend their gratitude to His Excellency Dr. APJ Abdul Kalam, Former President of India and Madame Ilora Finlay Baronness of the House of Lords for their Forewords to the White Book and to the International Primary Care Respiratory Group (IPCRG) and European Federation of Allergy and Airways Diseases Patients ‘Associations (EFA) for their supporting statements. -

Pediatrics Community About the Residency Recruitment Process May 19, 2021
APPD/COMSEP/AMSPDC/FuturePedsRes/NextGenPediatricians Letter to Our Pediatrics Community About the Residency Recruitment Process May 19, 2021 The leadership of APPD, COMSEP, AMSPDC, FuturePedsRes, and NextGenPediatricians have been working collaboratively with Undergraduate Medical Education (UME) and Graduate Medical Education (GME) leaders and learners to optimize the recruitment process for applicants and programs. Through this process, we have sought substantial input from applicants, program leaders, chairs, and the greater community including other subspecialties. In addition, we have reviewed and appreciate the recommendations from the Coalition for Physician Accountability. Our primary goal is to optimize the recruitment process for both learners and programs by: (1) Helping learners find programs that match their career goals while providing an atmosphere conducive to their learning styles. (2) Creating a fair and equitable application process for both learners and programs. This past interview season has opened our eyes to ways of improving equity in our processes. In addition, there continues to be uncertainty due to the COVID‐19 pandemic, with some regions still experiencing surges and travel restrictions. Given that many are most focused on the types of interviews we will be doing this coming year, we present that recommendation up front, and then go into the additional recommendations below. Following many conversations and surveys with each of our organizations, we strongly recommend only offering virtual interviews for the 2021‐2022 recruitment cycle for several reasons: (1) Effective assessment: The majority of applicants and programs highlighted that they thought the assessment of applicants was sufficient using virtual interviews in the 2020‐ 2021 cycle. (2) Equity: Virtual interviews are more equitable for applicants and programs, both in terms of cost savings and in terms of any remaining restrictions from the COVID‐19 pandemic. -

Former General Pediatrics Fellows
Former General Pediatrics Fellows Alumni, 2007–2017 2007 Name: Copeland-Linder, Nikeea Prior Training: PhD (Psychology), University of Michigan Years In Program: 2005-2007 Mentors: Tina Cheng, Nick Lalongo Research Area: Youth violence prevention, child stress and mental health Current Position: Child psychologist, Ellicott City 2008 Name: Garg, Arvin Prior Training: MD: Boston University School of Medicine; MPH: Boston University School of Public Health; Pediatric Residency: Univ. of Connecticut School of Medicine Years In Program: 2004-2008 Mentors: Janet Serwint, Arlene Butz Research Area: Addressing social determinants of health within pediatric primary care Associate Professor, Boston University School of Medicine; Associate Director Current Position: of Medical Student Education for Pediatrics Name: Kuo, Dennis Prior Training: MD: University of Pennsylvania; Pediatric Residency, University of North Years In Program: Carolina Degrees Earned: 2005-2008 Mentors: MHS, Johns Hopkins University Bloomberg School of Public Health Research Area: Cynthia Minkovitz Current Position: Associate Professor and Chief, General Pediatrics, University at Buffalo, and Medical Director of Primary Care Services at Women & Children‘s Hospital of Buffalo 2009 Name: Dodge, Rachel Prior Training: MD: University of Maryland; Pediatric Residency: Rainbow Babies and Children’s Hospital, Cleveland, OH Years In Program: 2005-2009 Degrees Earned: MPH: Johns Hopkins University Bloomberg School of Public Health Mentors: Anne Duggan, Tina Cheng, Tracy King, Megan Bair-Merritt Research Area: Primary care based interventions to promote positive parenting Current Position: Pediatrician, Dundalk Pediatric Association (Johns Hopkins Medicine) Name: Murray, Kantahyaneee Prior Training: PhD (Public Health): University of Maryland Years In Program: 2007-9 Mentors: Tina Cheng, Megan Bair-Merritt Research Area: Role of primary care in youth violence prevention Current Position: Senior Research Associate, Annie E. -
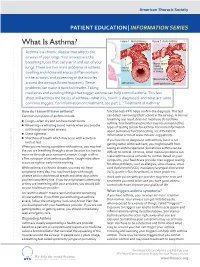
What Is Asthma? Figure 1
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES What Is Asthma? Figure 1. Normal Airway Figure 2. Acute Asthma Asthma is a chronic disease that affects the airways of your lungs. Your airways are the breathing tubes that carry air in and out of your Muscle spasm causing lungs. There are two main problems in asthma: relaxed narrowing muscles swelling and increased mucus (inflammation) of airways in the airways, and squeezing of the muscles Mucus build up around the airways (bronchospasm). These open airways Swelling/inammation problems can make it hard to breathe. Taking medicines and avoiding things that trigger asthma can help control asthma. This fact sheet will address the basics of asthma—what it is, how it is diagnosed, and what are some common triggers. For information on treatment, see part 2, “Treatment of Asthma”. How do I know if I have asthma? function test–PFT) helps confirm the diagnosis. This test Common symptoms of asthma include: can detect narrowing (obstruction) in the airways. A normal breathing test result does not mean you do not have ■ Cough—often dry and can have harsh bursts asthma. Your healthcare provider may recommend other ■ Wheezing—a whistling sound mainly when you breathe types of testing to look for asthma. For more information out through narrowed airways about pulmonary function testing, see ATS Patient ■ Chest tightness Information series at www.thoracic.org/patients. ■ Shortness of breath which may occur with activity or If you have been diagnosed with asthma, but it is not even at rest getting better with treatment, you might benefit from When you are having a problem with asthma, you may feel CLIP AND COPY AND CLIP seeing an asthma specialist. -

Bee Venom Allergy in Beekeepers and Their Family Members Ulrich R
Bee venom allergy in beekeepers and their family members Ulrich R. Mu¨ller Purpose of review Introduction To analyze prevalence of allergic sting reactions, including Hymenoptera venom allergy is one of the major reasons the clinical and diagnostic features as well as management for anaphylaxis. Between 1961 and 2000, it caused 120 options in a population heavily exposed to honeybee stings fatalities in Switzerland – an average of three every year such as beekeepers and their family members. [1]. Extrapolated to Western Europe, this corresponds to Recent findings more than 150 fatal Hymenoptera sting reactions every The higher sting frequency is associated with an increased year in this region. Stings by honeybees and vespids are prevalence of allergic sting reactions. Major risk factors for most often responsible for such reactions. Beekeepers allergic sting reactions in beekepers are: fewer than 10 and their family members are heavily exposed to honey- annual stings, an atopic constitution and symptoms of bee stings and are thus at an especially high risk of upper respiratory allergy during work in the beehive. Bee becoming allergic, and therefore are an interesting popu- venom allergic beekeepers have higher levels of bee lation for the study of epidemiology and immunopatho- venom-specific IgG but lower skin sensitivity and bee genesis of venom allergy and the mechanism of its most venom-specific IgE than normally exposed bee venom effective treatment – venom immunotherapy. Finally, allergic patients. Safety of bee venom immunotherapy is owing to the high degree of exposure of this population, higher in beekeepers than in allergic controls, while efficacy indication and protocols for venom immunotherapy may of this treatment is similar in both groups. -

Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitisation
Allergic Bronchopulmonary Aspergillosis and Severe Asthma with Fungal Sensitisation Dr Rohit Bazaz National Aspergillosis Centre, UK Manchester University NHS Foundation Trust/University of Manchester ~ ABPA -a41'1 Severe asthma wl'th funga I Siens itisat i on Subacute IA Chronic pulmonary aspergillosjs Simp 1Ie a:spe rgmoma As r§i · bronchitis I ram une dysfu net Ion Lun· damage Immu11e hypce ractivitv Figure 1 In t@rarctfo n of Aspergillus Vliith host. ABP A, aHerg tc broncho pu~ mo na my as µe rgi ~fos lis; IA, i nvas we as ?@rgiH os 5. MANCHl·.'>I ER J:-\2 I Kosmidis, Denning . Thorax 2015;70:270–277. doi:10.1136/thoraxjnl-2014-206291 Allergic Fungal Airway Disease Phenotypes I[ Asthma AAFS SAFS ABPA-S AAFS-asthma associated with fu ngaIsensitization SAFS-severe asthma with funga l sensitization ABPA-S-seropositive a llergic bronchopulmonary aspergi ll osis AB PA-CB-all ergic bronchopulmonary aspergi ll osis with central bronchiectasis Agarwal R, CurrAlfergy Asthma Rep 2011;11:403 Woolnough K et a l, Curr Opin Pulm Med 2015;21:39 9 Stanford Lucile Packard ~ Children's. Health Children's. Hospital CJ Scanford l MEDICINE Stanford MANCHl·.'>I ER J:-\2 I Aspergi 11 us Sensitisation • Skin testing/specific lgE • Surface hydroph,obins - RodA • 30% of patients with asthma • 13% p.atients with COPD • 65% patients with CF MANCHl·.'>I ER J:-\2 I Alternar1a• ABPA •· .ABPA is an exagg·erated response ofthe imm1une system1 to AspergUlus • Com1pUcatio n of asthm1a and cystic f ibrosis (rarell·y TH2 driven COPD o r no identif ied p1 rior resp1 iratory d isease) • ABPA as a comp1 Ucation of asth ma affects around 2.5% of adullts.