Federal Register/Vol. 84, No. 201/Thursday, October 17, 2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

MIAMI-DADE COUNTY EDUCATIONAL FACILITIES AUTHORITY $235,000,000* Revenuebonds,Series2018a(Universityofmiamiissue) Wells Fargosecurities
PRELIMINARY OFFICIAL STATEMENT DATED MARCH 8, 2018 NEW ISSUE Moody’s: A3 (Book-Entry Only) S&P: A- (See “RATINGS” herein) In the opinion of Bryant Miller Olive P.A. and Llorente & Heckler, P.A., Co-Bond Counsel, assuming continuing compliance by the Authority and the University with certain covenants, under existing statutes, regulations and judicial decisions, the interest on the Series 2018A Bonds is excluded from gross income for federal income tax purposes of the holders thereof and is not an item of tax preference for purposes of the federal alternative minimum tax. However, interest on the Series 2018A Bonds shall be taken into account in determining adjusted current earnings for purposes of computing the alternative minimum tax on corporations for taxable years that began prior to January 1, 2018. The alternative minimum tax on corporations was repealed for taxable years beginning on and after January 1, 2018. INTEREST ON THE SERIES 2018B BONDS WILL NOT BE EXCLUDED FROM GROSS INCOME FOR FEDERAL INCOME TAX PURPOSES. See “TAX MATTERS” herein for a description of certain other tax consequences to holders of the Series 2018 Bonds. $250,000,000* MIAMI-DADE COUNTY EDUCATIONAL FACILITIES AUTHORITY $235,000,000* Revenue Bonds, Series 2018A (University of Miami Issue) $15,000,000* Revenue Bonds, Series 2018B (University of Miami Issue) (Taxable) Dated: Date of Delivery Due: April 1, as shown on the inside cover page This cover page contains certain information for quick reference only. It is not a summary of this Issue. Investors must read the entire Official Statement for information essential to the making of an informed investment decision. -

Sunday, October 4 Saturday, October 17
DUE TO COVID-19, ALL RESIDENTS MUST REMAIN IN THEIR VEHICLE AND PLACE THEIR MATERIALS IN THEIR TRUNK. Household Hazardous Waste, E-Waste & Tire Collection Days FREE! Sunday, October 4 Saturday, October 17 9AM – 1PM (RAIN OR SHINE) 9AM – 1PM (RAIN OR SHINE) Gorman Field in Bayonne Jersey City Municipal Service Complex Parking Lot – West 1st Street near Humphry Ave 13-15 Linden Ave Hoboken DPW Kearny DPW Willow Ave & Observer Highway 357 Bergen Ave WHAT TO BRING: WHAT NOT TO BRING: • Thermostats • Solvents & Thinners • Consumer Electronics • Infectious Waste • Tires • Pesticides • Alkaline Batteries • Silvex 2,4,5-t • Cleaners & Corrosives & Herbicides • Latex Paint • Radioactive Material • Pool & Photographic • Formaldehyde • Explosives • Unknown or Chemicals • Compact • Compressed Gas Unidentified Material • Oil Based Paints Fluorescent Bulbs Cylinders & Tanks • Ballasts & Varnishes • Used Motor Oil • TCBs, TCCD • Washers, Dryers, • Rechargeable • Old Gasoline (such as Freon & Helium) Refrigerators, & Car Batteries • Fire Extinguishers • Woodlife Air Conditioners • Propane Tanks • Antifreeze • Asbestos • Any OTC or (from BBQ grills only) • Smoke Detectors • Kepone Prescription Drugs TIRE AMNESTY COLLECTION COMPUTER & Hudson County residents are asked to bring no more than 4 tires for TECH RECYCLING proper disposal. If you cannot participate in this year’s Tire Amnesty Event, eitherstore tires indoors (in a garage or shed) or cover them until Computers, monitors, computer mice, keyboards, they can bedisposed of properly.* *CONTACT YOUR MUNICIPAL DPW FOR DISPOSAL LOCATIONS. tablets and cellphones can also be recycled. This program is sponsored, in part, by a grant from the NJDEP-Division of Solid and Hazardous Waste. Residents can drop off materials at any site. Proof of residency may be required. -

Stark Reality
LITCH’S LAW LOG C. Scott Litch Chief Operating Officer and General Counsel Stark Reality Dentists must be in compliance with federal anti-kickback laws and self-referral laws. The latter is often referred to as the Stark Law in recognition of its legislative creator, Congressman Pete Stark (D-13th Calif.). The ADA has addressed these issues in their recently updated publication The ADA Practical Guide to Frequently Asked Legal Questions. Specifically, they note that: • A dentist risks violating federal and state anti-kickback and There is also new law in this area under the Patient Protection self-referral laws if he or she might receive a direct or indirect and Affordable Care Act (PPACA) aka the health care reform law: benefit from referring a patient. • Section 6402 provides that an “overpayment” is any funds • Federal law makes it a crime to pay or receive (or even to offer received or retained under Medicare or Medicaid to which or solicit) any kind of remuneration for a referral for which a a person is not entitled. A provider must report and return federal health care program will pay in whole or in part. This overpayments by the later of: 60 days after the date of identifi- is a felony punishable by fines of up to $25,000 and/or up cation of the overpayment; or the date when a corresponding to five years in prison. However, there are a number of “safe cost report is due, if applicable. harbors” that provide exceptions. For example, a physician • Section 6409 requires the Centers for Medicare and Medicaid can rent office space from a dentist, provided that the rent is Services (CMS) to publish a protocol advising providers and consistent with fair market value and does not take into ac- suppliers how they may voluntarily disclose actual and poten- count the volume or value of referrals. -

Anti-Kickback, Stark and the Affordable Care Act
Anti-Kickback, Stark and the Affordable Care Act As the Affordable Care Act continues to reward enterprises such as Accountable Care Organizations that (i) improve the health experience of patients, and (ii) operate efficiently by reducing costs, a health care practitioner should not lose sight on schemes that could run afoul of prohibited self- referral or anti-kickback laws. Since 1972, Congress prohibited practitioners from entering into “kickback” arrangements if such arrangements involved a paid referral that related to the Medicare Program. As enforcement of the anti-kickback law has expanded to include self-referrals as a prohibited activity, the anti-kickback and self-referral laws now cover the Medicaid and Tricare Programs . In fact, 2016 is expected to be a busy year with respect to enforcement of Stark and Anti-kickback violations. As the year continues to unfold, it is important to be reminded generally what (i) anti-kickback and (ii) self-referral means in the ever changing economics of providing health care. In general, the anti- kickback prohibition or specifically Section 1320a-7b of Title 42 of the United States Code prohibits any person from: (i) knowingly and willfully (ii) soliciting, receiving, offering to pay, or paying any (iii) remuneration (including any kickback, bribe, or rebate) in return for (a) referring an individual to a person for the furnishing or arranging for the furnishing of any item or service for which payment may be made under a federal health care program, or (b) purchasing, leasing, ordering, arranging any good, facility, service, or item for which payment may be made under a federal health care program. -

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -
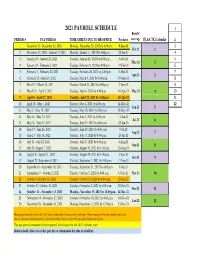
Payroll Calendar 2021
2021 PAYROLL SCHEDULE 1 Benefit PERIOD # PAY PERIOD TIME SHEETS DUE TO HR OFFICE Paydates coverage FLSA 7K Calendar 2 1 December 13- December 26, 2020 Monday, December 28, 2020 by 4:00 p.m. 8-Jan-21 3 Feb-21 1 2 December 27, 2020 - Janurary 9, 2021 Monday, January 11, 2021 by 4:00 p.m. 22-Jan-21 4 3 January 10 - January 23, 2021 Tuesday, January 26, 2021 by 4:00 p.m. 5-Feb-21 5 Mar-21 2 4 January 24 - February 6, 2021 Tuesday, February 9, 2021 by 4:00 p.m. 19-Feb-21 6 5 February 7 - February 20, 2021 Tuesday, February 26, 2021 by 4:00 p.m. 5-Mar-21 7 Apr-21 3 6 February 21 - March 6, 2021 Tuesday, March 9, 2021 by 4:00 p.m. 19-Mar-21 8 7 March 7 - March 20, 2021 Tuesday, March 23, 2021 by 4:00 p.m. 2-Apr-21 9 8 March 21 - April 3, 2021 Tuesday, April 6, 2021 by 4:00 p.m. 16-Apr-21 May-21 4 10 9 April 4 - April 17, 2021 Tuesday, April 20, 2021 by 4:00 p.m. 30-Apr-21 11 10 April 18 - May 1, 2021 Tuesday, May 4, 2021 by 4:00 p.m. 14-May-21 12 Jun-21 5 11 May 2 - May 15, 2021 Tuesday, May 18, 2021 by 4:00 p.m. 28-May-21 12 May 16 - May 29, 2021 Tuesday, June 1, 2021 by 4:00 p.m. 11-Jun-21 Jul-21 6 13 May 30 - June 12, 2021 Tuesday, June 15, 2021 by 4:00 p.m. -

FOR RELEASE October 17, 2019 for MEDIA OR
FOR RELEASE October 17, 2019 FOR MEDIA OR OTHER INQUIRIES: Carroll Doherty, Director of Political Research Jocelyn Kiley, Associate Director, Research Nida Asheer, Communications Associate 202.419.4372 www.pewresearch.org RECOMMENDED CITATION Pew Research Center, October 2019, “Modest Changes in Views of Impeachment Proceedings Since Early September” 1 PEW RESEARCH CENTER About Pew Research Center Pew Research Center is a nonpartisan fact tank that informs the public about the issues, attitudes and trends shaping the world. It does not take policy positions. The Center conducts public opinion polling, demographic research, content analysis and other data-driven social science research. It studies U.S. politics and policy; journalism and media; internet, science and technology; religion and public life; Hispanic trends; global attitudes and trends; and U.S. social and demographic trends. All of the Center’s reports are available at www.pewresearch.org. Pew Research Center is a subsidiary of The Pew Charitable Trusts, its primary funder. © Pew Research Center 2019 www.pewresearch.org 2 PEW RESEARCH CENTER Most Americans have not changed their views on whether the House should conduct impeachment proceedings against President Donald Trump since early September, before House Speaker Nancy Pelosi announced that the House would conduct an impeachment inquiry of the president. Majority of public approves of House But about one-in-ten adults (9%) who had decision to begin impeachment inquiry opposed the House opening impeachment % who ___ of the House of Representatives’ decision to proceedings last month now approve of the begin an impeachment inquiry decision to conduct an impeachment inquiry, based on an analysis that tracks change in opinion among the same survey respondents How confident are you that ____ in Congress will be over time. -

The Stark Law, Post-Pandemic
THOMSON REUTERS The Stark Law, post-pandemic By Kelly M. Cleary, Esq., Akin Gump Strauss Hauer & Feld LLP JULY 10, 2020 When our nation’s hospitals and health professionals found of 1989 was passed with the purpose of prohibiting physicians from themselves on the front lines in the battle against the 2019 Novel referring Medicare patients to clinical labs in which the physician Coronavirus (COVID-19) pandemic, the United States Department had some financial relationship.4 of Health and Human Services (HHS) acted quickly and decisively Another wave of studies conducted on the heels of the 1989 to issue an array of temporary regulatory waivers and new rules OIG study produced more fodder for reform, finding additional designed to give the health care system “maximum flexibility” to instances outside of the clinical laboratory context where physician respond to the crisis.1 financial interests appeared to be driving increases in utilization.5 Among the temporary waivers issued were partial waivers of sanctions under Section 1877 of the Social Security Act, otherwise The law and its implementing regulations known as the physician self-referral law or the “Stark Law.” embody a regulatory scheme that has been The waivers of sanctions under the Stark Law have allowed hospitals and other providers to support the physician community, referred to as “a booby trap rigged with strict and vice versa, and allowed the reshaping of financial relationships liability and potentially ruinous exposure.” in ways that might otherwise have opened the door to major liability. Moved by these studies, Congress expanded the law in 1993 to ban These waivers provided welcome regulatory relief, but they are self-referrals for a vast array of services, including inpatient and limited in scope, applicability and, importantly, duration. -

AMEDISYS, INC. (Exact Name of Registrant As Specified in Its Charter)
Section 1: 10-Q (10-Q) Table of Contents UNITED STATES SECURITIES AND EXCHANGE COMMISSION Washington D.C. 20549 FORM 10-Q (Mark One) x QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the quarterly period ended June 30, 2014 or ¨ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the transition period from to Commission File Number: 0-24260 AMEDISYS, INC. (Exact Name of Registrant as Specified in its Charter) Delaware 11-3131700 (State or other jurisdiction of (I.R.S. Employer incorporation or organization) Identification No.) 5959 S. Sherwood Forest Blvd., Baton Rouge, LA 70816 (Address of principal executive offices, including zip code) (225) 292-2031 or (800) 467-2662 (Registrant’s telephone number, including area code) Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨ Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). -

2018 - 2019 Days of Rotation Calendar
2018 - 2019 DAYS OF ROTATION CALENDAR Day # Date Rotation Day Type Notes Day # Date Rotation Day Type Notes Saturday, October 13, 2018 Sunday, October 14, 2018 Monday, September 3, 2018 Holiday/Vaca Labor Day 27 Monday, October 15, 2018 Day 3 In Session 1 Tuesday, September 4, 2018 Day 1 In Session 28 Tuesday, October 16, 2018 Day 4 In Session 2 Wednesday, September 5, 2018 Day 2 In Session 29 Wednesday, October 17, 2018 Day 5 In Session 3 Thursday, September 6, 2018 Day 3 In Session 30 Thursday, October 18, 2018 Day 6 In Session 4 Friday, September 7, 2018 Day 4 In Session 31 Friday, October 19, 2018 Day 1 In Session Saturday, September 8, 2018 Saturday, October 20, 2018 Sunday, September 9, 2018 Sunday, October 21, 2018 Monday, September 10, 2018 Day Holiday/Vaca Rosh Hashanah 32 Monday, October 22, 2018 Day 2 In Session 5 Tuesday, September 11, 2018 Day 5 In Session 33 Tuesday, October 23, 2018 Day 3 In Session 6 Wednesday, September 12, 2018 Day 6 In Session 34 Wednesday, October 24, 2018 Day 4 In Session 7 Thursday, September 13, 2018 Day 1 In Session 35 Thursday, October 25, 2018 Day 5 In Session 8 Friday, September 14, 2018 Day 2 In Session 36 Friday, October 26, 2018 Day 6 In Session Saturday, September 15, 2018 Saturday, October 27, 2018 Sunday, September 16, 2018 Sunday, October 28, 2018 9 Monday, September 17, 2018 Day 3 In Session 37 Monday, October 29, 2018 Day 1 In Session 10 Tuesday, September 18, 2018 Day 4 In Session 38 Tuesday, October 30, 2018 Day 2 In Session Wednesday, September 19, 2018 Day Holiday/Vaca Yom Kippur 39 Wednesday, October 31, 2018 Day 3 In Session 11 Thursday, September 20, 2018 Day 5 In Session 40 Thursday, November 1, 2018 Day 4 In Session 12 Friday, September 21, 2018 Day 6 In Session 41 Friday, November 2, 2018 Day 5 In Session Saturday, September 22, 2018 Saturday, November 3, 2018 Sunday, September 23, 2018 Sunday, November 4, 2018 13 Monday, September 24, 2018 Day 1 In Session 42 Monday, November 5, 2018 Day 6 In Session 14 Tuesday, September 25, 2018 Day 2 In Session Tuesday, November 6, 2018 Prof Dev. -

Julian Date Cheat Sheet for Regular Years
Date Code Cheat Sheet For Regular Years Day of Year Calendar Date 1 January 1 2 January 2 3 January 3 4 January 4 5 January 5 6 January 6 7 January 7 8 January 8 9 January 9 10 January 10 11 January 11 12 January 12 13 January 13 14 January 14 15 January 15 16 January 16 17 January 17 18 January 18 19 January 19 20 January 20 21 January 21 22 January 22 23 January 23 24 January 24 25 January 25 26 January 26 27 January 27 28 January 28 29 January 29 30 January 30 31 January 31 32 February 1 33 February 2 34 February 3 35 February 4 36 February 5 37 February 6 38 February 7 39 February 8 40 February 9 41 February 10 42 February 11 43 February 12 44 February 13 45 February 14 46 February 15 47 February 16 48 February 17 49 February 18 50 February 19 51 February 20 52 February 21 53 February 22 54 February 23 55 February 24 56 February 25 57 February 26 58 February 27 59 February 28 60 March 1 61 March 2 62 March 3 63 March 4 64 March 5 65 March 6 66 March 7 67 March 8 68 March 9 69 March 10 70 March 11 71 March 12 72 March 13 73 March 14 74 March 15 75 March 16 76 March 17 77 March 18 78 March 19 79 March 20 80 March 21 81 March 22 82 March 23 83 March 24 84 March 25 85 March 26 86 March 27 87 March 28 88 March 29 89 March 30 90 March 31 91 April 1 92 April 2 93 April 3 94 April 4 95 April 5 96 April 6 97 April 7 98 April 8 99 April 9 100 April 10 101 April 11 102 April 12 103 April 13 104 April 14 105 April 15 106 April 16 107 April 17 108 April 18 109 April 19 110 April 20 111 April 21 112 April 22 113 April 23 114 April 24 115 April -

Due Date Chart 201803281304173331.Xlsx
Special Event Permit Application Due Date Chart for Events from January 1, 2019 - June 30, 2020 If due date lands on a Saturday or Sunday, the due date is moved to the next business day Event Date 30 Calendar days 90 Calendar Days Tuesday, January 01, 2019 Sunday, December 02, 2018 Wednesday, October 03, 2018 Wednesday, January 02, 2019 Monday, December 03, 2018 Thursday, October 04, 2018 Thursday, January 03, 2019 Tuesday, December 04, 2018 Friday, October 05, 2018 Friday, January 04, 2019 Wednesday, December 05, 2018 Saturday, October 06, 2018 Saturday, January 05, 2019 Thursday, December 06, 2018 Sunday, October 07, 2018 Sunday, January 06, 2019 Friday, December 07, 2018 Monday, October 08, 2018 Monday, January 07, 2019 Saturday, December 08, 2018 Tuesday, October 09, 2018 Tuesday, January 08, 2019 Sunday, December 09, 2018 Wednesday, October 10, 2018 Wednesday, January 09, 2019 Monday, December 10, 2018 Thursday, October 11, 2018 Thursday, January 10, 2019 Tuesday, December 11, 2018 Friday, October 12, 2018 Friday, January 11, 2019 Wednesday, December 12, 2018 Saturday, October 13, 2018 Saturday, January 12, 2019 Thursday, December 13, 2018 Sunday, October 14, 2018 Sunday, January 13, 2019 Friday, December 14, 2018 Monday, October 15, 2018 Monday, January 14, 2019 Saturday, December 15, 2018 Tuesday, October 16, 2018 2019 Tuesday, January 15, 2019 Sunday, December 16, 2018 Wednesday, October 17, 2018 Wednesday, January 16, 2019 Monday, December 17, 2018 Thursday, October 18, 2018 Thursday, January 17, 2019 Tuesday, December 18, 2018