Modern Surgery, 4Th Edition, by John Chalmers Da Costa Rare Medical Books
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Downhill Varices Resulting from Giant Intrathoracic Goiter
E40 UCTN – Unusual cases and technical notes Downhill varices resulting from giant intrathoracic goiter Fig. 2 Sagittal com- puted tomography of the chest. The goiter was immense, reaching the aortic arch, sur- rounding the trachea and partially compres- sing the upper esopha- gus. The esophagus was additionally com- pressed by anterior spinal spondylophytes. Fig. 1 Multiple submucosal veins in the upper esophagus, consistent with downhill varices. An 82-year-old man was admitted to the hospital because of substernal chest pain, dyspnea, and occasional dysphagia to sol- ids. His past medical history was remark- geal varices are called “downhill varices”, References able for diabetes mellitus type II, hyper- as they are located in the upper esophagus 1 Kotfila R, Trudeau W. Extraesophageal vari- – lipidemia, and Parkinson’s disease. On and project downwards. Downhill varices ces. Dig Dis 1998; 16: 232 241 2 Basaranoglu M, Ozdemir S, Celik AF et al. A occur as a result of shunting in cases of up- physical examination he appeared frail case of fibrosing mediastinitis with obstruc- but with no apparent distress. Examina- per systemic venous obstruction from tion of superior vena cava and downhill tion of the neck showed no masses, stri- space-occupying lesions in the medias- esophageal varices: a rare cause of upper dor or jugular venous distension. Heart tinum [2,3]. Downhill varices as a result of gastrointestinal hemorrhage. J Clin Gastro- – examination disclosed a regular rate and mediastinal processes are reported to enterol 1999; 28: 268 270 3 Calderwood AH, Mishkin DS. Downhill rhythm; however a 2/6 systolic ejection occur in up to 50% of patients [3,4]. -

Selective Venous Sampling for Primary Hyperparathyroidism: How to Perform an Examination and Interpret the Results with Reference to Thyroid Vein Anatomy
Jpn J Radiol DOI 10.1007/s11604-017-0658-3 INVITED REVIEW Selective venous sampling for primary hyperparathyroidism: how to perform an examination and interpret the results with reference to thyroid vein anatomy Takayuki Yamada1 · Masaya Ikuno1 · Yasumoto Shinjo1 · Atsushi Hiroishi1 · Shoichiro Matsushita1 · Tsuyoshi Morimoto1 · Reiko Kumano1 · Kunihiro Yagihashi1 · Takuyuki Katabami2 Received: 11 April 2017 / Accepted: 28 May 2017 © Japan Radiological Society 2017 Abstract Primary hyperparathyroidism (pHPT) causes and brachiocephalic veins for catheterization of the thyroid hypercalcemia. The treatment for pHPT is surgical dis- veins and venous anastomoses. section of the hyperfunctioning parathyroid gland. Lower rates of hypocalcemia and recurrent laryngeal nerve injury Keywords Primary hyperparathyroidism · Localization · imply that minimally invasive parathyroidectomy (MIP) is Thyroid vein · Venous sampling safer than bilateral neck resection. Current trends in MIP use can be inferred only by reference to preoperative locali- zation studies. Noninvasive imaging studies (typically pre- Introduction operative localization studies) show good detection rates of hyperfunctioning glands; however, there have also been Primary hyperparathyroidism (pHPT) is a common endocrine cases of nonlocalization or discordant results. Selective disease. Most patients have one adenoma, but double adeno- venous sampling (SVS) is an invasive localization method mas have been reported in up to 15% of cases [1]. Approxi- for detecting elevated intact parathyroid -

Anatomy & Embryology of Thyroid & Parathyroid
ANATOMY & EMBRYOLOGY OF THYROID & PARATHYROID By Prof . Saeed Abuel Makarem & Associate Prof. Sanaa Alshaarawy 1 OBJECTIVES Ò By the end of the lecture, the student should be able to: Ò Describe the shape, position, relations and structure of the thyroid gland. Ò List the blood supply & lymphatic drainage of the thyroid gland. Ò List the nerves endanger with thyroidectomy operation. Ò Describe the shape, position, blood supply & lymphatic drainage of the parathyroid glands. Ò Describe the development of the thyroid & parathyroid glands. Ò Describe the most common congenital anomalies of the thyroid gland. 2 Before we go to the thyroid What are the parts of the deep fascia or deep cervical fascia of the neck? It is divided mainly into 3 layers: 1- Investing layer. 2- Pretracheal layer. 3- Prevertebral layer. 3 Ò Endocrine, butterfly Thyroid gland shaped gland. Ò Consists of right & left lobes. Ò The 2 lobes are connected to each other by a narrow isthmus, which overlies the 2nd ,3rd & 4th tracheal rings. Ò It is surrounded by a facial sheath derived from the pretracheal layer of the deep cervical fascia. 4 Thyroid gland Ò Each lobe is pear- shaped, with its apex reaches up to the oblique line of thyroid cartilage. Ò Its base lies at the level of 4th or 5th tracheal rings. Ò Inside the pretracheal facial capsule, there is another C.T capsule. Ò So, it s surrounded by 2 membranes. 5 Each lobe is pear shape, with its apex directed upward as far as the Anterior oblique line of the thyroid cartilage; its base lies at the 4th or 5th tracheal ring. -

An Unusual Origin and Course of the Thyroidea Ima Artery, with Absence of Inferior Thyroid Artery Bilaterally
Surgical and Radiologic Anatomy (2019) 41:235–237 https://doi.org/10.1007/s00276-018-2122-1 ANATOMIC VARIATIONS An unusual origin and course of the thyroidea ima artery, with absence of inferior thyroid artery bilaterally Doris George Yohannan1 · Rajeev Rajan1 · Akhil Bhuvanendran Chandran1 · Renuka Krishnapillai1 Received: 31 May 2018 / Accepted: 21 October 2018 / Published online: 25 October 2018 © Springer-Verlag France SAS, part of Springer Nature 2018 Abstract We report an unusual origin and course of the thyroidea ima artery in a male cadaver. The ima artery originated from the right subclavian artery very close to origin of the right vertebral artery. The artery coursed anteriorly between the common carotid artery medially and internal jugular vein laterally. It then coursed obliquely, from below upwards, from lateral to medial superficial to common carotid artery, to reach the inferior pole of the right lobe of thyroid and branched repeatedly to supply the anteroinferior and posteroinferior aspects of both the thyroid lobes and isthmus. The superior thyroid arteries were normal. Both the inferior thyroid arteries were absent. The unusual feature of this thyroidea ima artery is its origin from the subclavian artery close to vertebral artery origin, the location being remarkably far-off from the usual near midline position, and the oblique and relatively superficial course. This report is a caveat to neck surgeons to consider such a superficially running vessel to be a thyroidea ima artery. Keywords Thyroid vascular anatomy · Thyroidea ima artery · Artery of Neubauer · Blood supply of thyroid · Variations Introduction (1.1%), transverse scapular (1.1%), or pericardiophrenic or thyrocervical trunk [8, 10]. -

Endocrine Block اي كالم باللون الذهبي مأخوذ من التيم وورك فايل )الي يقال انه اكسترا( EDITING FLIE Anatomy of Pituitary Gland
PRACTICAL ANATOMY Endocrine Block اي كﻻم باللون الذهبي مأخوذ من التيم وورك فايل )الي يقال انه اكسترا( EDITING FLIE Anatomy Of Pituitary Gland 2 Identify the Pointed areas: 1 1- hypophyseal fossa(Sella turcica). 2-anterior & posterior clinoidal process. The pituitary gland: located in middle cranial fossa and protected in sella turcica (hypophyseal fossa) of body of sphenoid. Relations Of Pituitary Gland Identify the Pointed areas: 1- mamillary bodies (posteriorly). 2 2-optic chiasma (anteriorly). 1 3-Sphenoidal air sinuses (inferior) . 3 4-body of the sphenoid. If Pituitary gland became enlarged (e.g 4 adenoma ) it will cause pressure on optic chiasma and lead to Bilateral temporal eye field blindness Relations Of Pituitary Gland 1 2 Identify the Pointed area : 1- Pituitary gland. 2- Diaphragma sellae (superior). 3-Sphenoidal air sinuses(inferior) . 4-Cavernous sinuses (lateral) . 4 3 Identify the Pointed area : 2 1- Anterior lobe(Adenohypophysis) . 2- optic chiasma 3- infundibulum . 4- Posterior lobe (Neurohypophysis) 3 SUBDIVISIONS OF PITUITARY GLAND 1 Anterior Posterior 4 Lobe(Adenohyp Lobe(Neurohyp ophysis) ophysis) The true gland connected to hypothalamus through hypothalamo- hypophyseal tract synthesizes & Secretes hormones Stores hormones secreted by hypothalamicnuclei receives a nerve supply from some of the hypothalamic nuclei (supraoptic & Hormone-releasing & inhibiting factors paraventricular) The axons of these produced by hypothalamus use nuclei convey their neurosecretion to Hypophyseal Portal System to reach the the Posterior lobe of pituitary gland Anterior lobe of pituitary gland through Hypothalamo-Hypophyseal tract from where it passes into the blood stream. Blood Supply Of Pituitary Gland Identify the Pointed area : 1- Superior hypophyseal artery: supplies infundibulum & forms a capillary network from which vessels pass downward & form sinusoids into the anterior lobe of pituitary gland (hypophyseal portal system). -

Thyroid and Parathyroid Glands
Thyroid and Parathyroid Glands Lecture (2) . Important . Doctors Notes Please check our Editing File . Notes/Extra explanation هذا العمل مبني بشكل أساسي على عمل دفعة 436 مع المراجعة {ومنْْيتو َ ّكْْع َلْْا ِّْللْفَهُوْْحس بهْ} َ َ َ َ َ َ َ َ َ ُ ُ والتدقيق وإضافة المﻻحظات وﻻ يغني عن المصدر اﻷساسي للمذاكرة . Objectives At the end of the lecture, students should be able to: Describe the shape, position, relations and of the thyroid gland. List the blood supply & lymphatic drainage of the thyroid gland. List the nerves endanger with thyroidectomy operation. Describe the shape, position, blood supply & lymphatic drainage of the parathyroid glands. Parts of the deep cervical fascia of the neck o It is divided mainly into 3 layers (or more) important during surgeries: • Investing layer (covers neck completely) • Pretracheal layer (covers thyroid gland and trachea) • Prevertebral layer (surrounds vertebra & prevretbral muscles). o The carotid sheath is part of the deep cervical fascia of the neck Note: At the 4 the corners of the neck, the investing layer separates to form two layers (anterior and posterior layers) to cover the sternocleidomastoid muscle in the anterolateral corner and trapezius muscle in the posterolateral corner "الغدة الدرقية" Thyroid Gland o Endocrine, butterfly shaped gland, Consists of right & left lobes connected to each other by a narrow isthmus, which overlies the 2nd ,3rd & 4th tracheal rings. o The gland is surrounded by a facial sheath derived from the pretracheal layer of the deep cervical fascia, what is the -

THE VARIATIONS of the INFERIOR THYROID VEIN of the DOMESTIC Clit
AUTHOR'S ABSTRACT OF THIS PAPER ISSCED BY THE BIBLIOGR.4PHIC SERVICE, FEBRUbRY 24 THE VARIATIONS OF THE INFERIOR THYROID VEIN OF THE DOMESTIC CLiT HARRISON R. HUNT West Virginia Universitv SEVEN FIGURES The inferior thyroid veins of man vary considerably. The following observations, made on thirty-three domestic cats selected at random, show that the same is true of this vein in the cat. Each of the accompanying figures represents, some- what diagrammatically, the conditions in a single animal. These seven animals suffice to give a fairly complete idea of the variations in the remaining twenty-six. Figure 1 shows the inferior thyroid vein (I) communicating anteriorly with the left internal jugular, receiving branches from only the left lobe of the thyroid gland (14), then passing ob- liquely backward across the trachea (13) to join the right innominate vein (10). The veins labeled 2 and 3 in this and the following figures were not homologized with certainty with the human superior and middle thyroid veins. Two other dis- sections resembled figure 1 very closely, except that in one of them the inferior thyroid vein joined the external jugular vein at a. Figure 2 resembles figure 1 in some respects. However, the inferior thyroid vein (1) in figure 2 receives a branch (a) from the right lobe of the thyroid gland (14), empties into the right internal jugular vein (a), but in the dissection did not appear to communicate directly with the left internal jugular. The inferior thyroid vein in a second cat joined the jugulars at m 39 40 HARRISON R. -
MR Venography
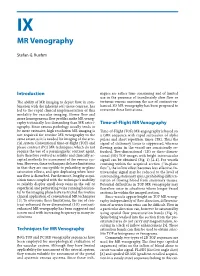
IX Ruehm 6-06-2005 19:20 Pagina 331 IX MR Venography Stefan G. Ruehm Introduction niques are rather time consuming and of limited use in the presence of inordinately slow flow or The ability of MR imaging to depict flow, in com- tortuous venous anatomy, the use of contrast-en- bination with the inherent soft tissue contrast, has hanced 3D MR venography has been proposed to led to the rapid clinical implementation of this overcome these limitations. modality for vascular imaging. Slower flow and more homogeneous flow profiles make MR venog- raphy technically less demanding than MR arteri- Time-of-Flight MR Venography ography. Since venous pathology usually tends to be more extensive, high resolution MR imaging is Time-of-Flight (TOF) MR angiography is based on not required for routine MR venography to the a GRE sequence with rapid succession of alpha same extent as it is needed for imaging of the arte- pulses and short repetition times (TR). Thus the rial system. Conventional time-of-flight (TOF) and signal of stationary tissue is suppressed, whereas phase contrast (PC) MR techniques, which do not flowing spins in the vessel are consistently re- require the use of a paramagnetic contrast agent, freshed. Two-dimensional (2D) or three-dimen- have therefore evolved as reliable and clinically ac- sional (3D) TOF images with bright intravascular cepted methods for assessment of the venous sys- signal can be obtained (Fig. 1) [2-4]. For vessels tem. However, these techniques do have limitations coursing within the acquired section (“in-plane in that they are susceptible to pulsatility, in-plane flow”), the inflow effect becomes less effective. -

Lecture in Anatomy of Endocrine System by Dr
Lecture in Anatomy of Endocrine System By Dr. Mohammad Ahmad Abdulla The endocrine system is made up of several glands:- the pituitary gland (Cerebral hypophysis), pineal, thyroid, thymus, parathyroids, suprarenals, islets of Langerhans of the pancreas, testes, ovaries, and, when present, the placenta. In addition, there are groups of cells that form a minor part of the system and are not considered in this chapter: the gastroenteroendocrine cells, kidney cells, and certain cells the lung that store and secrete amines. The endocrine glands have no ducts and consist of masses of cells richly supplied by blood vessels, which pour their secretions (hormones) directly into the blood stream. The medical professional needs a sound grounding in the structure and function of the endocrine system to be able to apply physiology lid hormone therapy in daily clinical practice, moreover, it must be remembered that disease y affect more than one endocrine gland at same time in an individual patient, a condition own as multiple endocrine neoplasia. It should ) be remembered that patients with advanced malignant disease sometimes produce hormones that are not indigenous to the tissue from which the tumor arose (paraneoplastic syndromes). 1 Pituitary Gland (Hypophysis Cerebri) Location and Description The pituitary gland is a small, oval structure attached to the undersurface of the brain by the infundibulum. During pregnancy, it doubles in size. The gland is well protected by virtue of its location in the sella turcica of the sphenoid bone. Because the hormones produced by the gland influence the activities of many other endocrine glands, the hypophysis cerebri is often referred to as the master endocrine gland. -

Biology 218 – Human Anatomy RIDDELL
Biology 218 – Human Anatomy RIDDELL Chapter 23 Adapted form Tortora 10th ed. LECTURE OUTLINE A. Comparison of Nervous and Endocrine Systems (see Table 23.1): (p. 704) 1. The nervous and endocrine systems together coordinate functions of all body systems. 2. The nervous system controls homeostasis via nerve impulses that trigger release of neurotransmitter molecules which act on other neurons, muscle cells, or gland cells. 3. The endocrine system controls homeostasis by secreting hormones, i.e., messenger molecules, into the bloodstream for delivery to virtually all body cells. 4. The nervous and endocrine systems act as a coordinated supersystem called the neuroendocrine system: some neurons stimulate or inhibit the release of hormones and some hormones promote or inhibit the initiation of nerve impulses. 5. The nervous system causes muscles to contract and glands to secrete either more or less of their product; the endocrine system affects virtually all body tissues by altering metabolic activities, regulating growth and development, and influencing reproductive processes. 6. Nerve impulses typically produce their effects within several milliseconds and the effects are relatively brief in duration; hormones may take seconds to hours to produce their effects and these effects are generally longer in duration. 7. Endocrinology is the science concerned with the structure and functions of the endocrine glands and the diagnosis and treatment of disorders of the endocrine system. B. Endocrine Glands Defined (p. 705) 1. The body contains two types of glands: i. exocrine glands (e.g., sudoriferous, sebaceous, and mucous glands) secrete their products into ducts which deliver the secretions into body cavities, into the lumen of an organ, or to the outer surface of the body ii. -
Incessant Bilobed Thymus in an Old Male Cadaver Case Report
Incessant Bilobed Thymus in an CASE REPORT Old Male Cadaver KC Sudikshya*1, Shah Aashish Kumar1, Khaling Rai Dipa2 1 Department of Anatomy, National Medical College, Birgunj, Nepal 2 Department of Medical Surgical Nursing, National Medical College, Birgunj, Nepal ABSTRACT INTRODUCTION Thymus is bilobed primary lymphoid organ Thymus is one of the primary lymphoid organs. situated in superior and anterior mediastinum. It is a soft, capsulated, bilobed gland which The appearance of thymus varies considerably belongs to endocrine system1responsible for the with age. It reaches maximum size at puberty and provision of thymus-processed lymphocytes (T eventually undergoes “fibro fatty involution”, lymphocytes) to the entire body, and provides but it may persist actively to old age. Therefore, a unique microenvironment in which T-cell normal appearance and size of thymus have precursors (thymocytes) undergo development, been elusive. Embryologically, it develops, as differentiation and clonal expansion. It’s lobes lie two separate organs from the endoderm of third close together side by side, joined in the midline pharyngeal pouches of embryo in common by connective tissue that merges with the capsule with inferior parathyroid glands and fuse in the of the organ. The greater part of the thymus lies midline. in the superior and anterior inferior mediastinum behind the manubrium. Superiorly, it extends The study was carried on 10 embalmed cadavers commonly into the neck and may reaches the of known sex in Anatomy Department of National inferior poles of the thyroid gland or even Medical College, Birgunj, Nepal. higher. Inferiorly, the lower border of the thymus reaches the level of the fourth costal cartilages. -
Review of the Variations of the Superficial Veins of the Neck
Open Access Review Article DOI: 10.7759/cureus.2826 Review of the Variations of the Superficial Veins of the Neck Dominic Dalip 1 , Joe Iwanaga 1 , Marios Loukas 2 , Rod J. Oskouian 3 , R. Shane Tubbs 4 1. Seattle Science Foundation, Seattle, USA 2. Anatomical Sciences, St. George's University, St. George's, GRD 3. Neurosurgery, Swedish Neuroscience Institute, Seattle, USA 4. Neurosurgery, Seattle Science Foundation, Seattle, USA Corresponding author: Joe Iwanaga, [email protected] Abstract The venous drainage of the neck can be characterized into superficial or deep. Superficial drainage refers to the venous drainage of the subcutaneous tissues, which are drained by the anterior and external jugular veins (EJVs). The brain, face, and neck structures are mainly drained by the internal jugular vein (IJV). The superficial veins are found deep to the platysma muscle while the deep veins are found encased in the carotid sheath. The junction of the retromandibular vein and the posterior auricular vein usually form the EJV, which continues along to drain into the subclavian vein. The anterior jugular vein is usually formed by the submandibular veins, travels downward anterior to the sternocleidomastoid muscle (SCM), and drains either into the EJV or the subclavian vein. Other superficial veins of the neck to consider are the superior, middle, and inferior thyroid veins. The superior thyroid and middle thyroid veins drain into the IJV whereas the inferior thyroid vein usually drains into the brachiocephalic veins. Categories: Miscellaneous Keywords: external jugular, vein, superficial, internal jugular, thyroid vein Introduction And Background The external jugular vein (EJV) is the preferred vein when performing a central venous catheterization.