Party Parliamentary Group for Ending Homelessness
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Victoria Prentis MP Presents a Bill
Victoria Prentis MP presents a bill "to make provision about mandatory local consultation in relation to changes in services proposed by NHS Trusts and healthcare commissioning authorities;and for connected purposes" 25 October 2016 Source: https://www.theyworkforyou.com/debates/?id=2016-10- 25a.190.8&s=victoria+prentis#g191.2 On Tuesday 25 October, North Oxfordshire MP Victoria Prentis, presented her first Ten Minute Rule Motion to the House on the subject of the Horton General Hospital. The National Health Service Provision (Local Consultation) Bill was a direct response to events over the summer at the Horton General Hospital, which saw the downgrade of the maternity unit to a midwife-only service with no public consultation. During her speech, Victoria voiced her concerns about the way in which the decision was taken and emphasised the need for public consultation whenever there is a change to NHS services, even when it is in response to an emergency situation. Presenting her Bill to the Commons, Victoria said in the Chamber: I do find it encouraging to have paternal, maternal and, indeed, filial support in this place, Mr Speaker. I beg to move, That leave be given for to bring in a bill to make provision about mandatory local consultation in relation to changes in services proposed by NHS Trusts and healthcare commissioning authorities; and for connected purposes. The Bill is the result of our experience in Oxfordshire this summer when the Oxford University Hospitals NHS Foundation Trust suspended consultant-led maternity services at our local general hospital with no warning and no consultation. -

Saturday 18 June 2011
Saturday 18 June 2011 Session 2010-12 No. 42 Edition No. 1117 House of Commons Weekly Information Bulletin This bulletin includes information on the work of the House of Commons in the period 13 - 17 June 2011 and forthcoming business for 20 - 24 June 2011 Contents House of Commons • Noticeboard .......................................................................................................... 1 • The Week Ahead .................................................................................................. 2 • Order of Oral Questions ....................................................................................... 3 Weekly Business Information • Business of the House of Commons 10 – 17 June 2011 ....................................... 4 Bulletin • Written Ministerial Statements ............................................................................. 8 • Forthcoming Business of the House of Commons 20 June – 1 July 2011 ............ 9 • Forthcoming Business of the House of Lords 20 June – 1 July 2011 ................. 12 Editor: Nerys Davies Legislation House of Commons Public Legislation Information Office • Public Bills before Parliament 2010/11 .............................................................. 15 London • Bills – Presentation, Publication and Royal Assent ............................................ 28 SW1A 2TT • Public and General Acts 2010/11 ....................................................................... 29 www.parliament.uk • Draft Bills under consideration or published during 2010/11 Session -

THE 422 Mps WHO BACKED the MOTION Conservative 1. Bim
THE 422 MPs WHO BACKED THE MOTION Conservative 1. Bim Afolami 2. Peter Aldous 3. Edward Argar 4. Victoria Atkins 5. Harriett Baldwin 6. Steve Barclay 7. Henry Bellingham 8. Guto Bebb 9. Richard Benyon 10. Paul Beresford 11. Peter Bottomley 12. Andrew Bowie 13. Karen Bradley 14. Steve Brine 15. James Brokenshire 16. Robert Buckland 17. Alex Burghart 18. Alistair Burt 19. Alun Cairns 20. James Cartlidge 21. Alex Chalk 22. Jo Churchill 23. Greg Clark 24. Colin Clark 25. Ken Clarke 26. James Cleverly 27. Thérèse Coffey 28. Alberto Costa 29. Glyn Davies 30. Jonathan Djanogly 31. Leo Docherty 32. Oliver Dowden 33. David Duguid 34. Alan Duncan 35. Philip Dunne 36. Michael Ellis 37. Tobias Ellwood 38. Mark Field 39. Vicky Ford 40. Kevin Foster 41. Lucy Frazer 42. George Freeman 43. Mike Freer 44. Mark Garnier 45. David Gauke 46. Nick Gibb 47. John Glen 48. Robert Goodwill 49. Michael Gove 50. Luke Graham 51. Richard Graham 52. Bill Grant 53. Helen Grant 54. Damian Green 55. Justine Greening 56. Dominic Grieve 57. Sam Gyimah 58. Kirstene Hair 59. Luke Hall 60. Philip Hammond 61. Stephen Hammond 62. Matt Hancock 63. Richard Harrington 64. Simon Hart 65. Oliver Heald 66. Peter Heaton-Jones 67. Damian Hinds 68. Simon Hoare 69. George Hollingbery 70. Kevin Hollinrake 71. Nigel Huddleston 72. Jeremy Hunt 73. Nick Hurd 74. Alister Jack (Teller) 75. Margot James 76. Sajid Javid 77. Robert Jenrick 78. Jo Johnson 79. Andrew Jones 80. Gillian Keegan 81. Seema Kennedy 82. Stephen Kerr 83. Mark Lancaster 84. -

Thursday 9 June 2016 Order Paper No.9: Part 1 SUMMARY AGENDA
Thursday 9 June 2016 Order Paper No.9: Part 1 SUMMARY AGENDA: CHAMBER 9.30am Prayers Afterwards Oral Questions: Culture, Media and Sport 10.15am Oral Questions: House of Commons Commission and the Leader of the House 10.30am Urgent Questions (if any), Business Question to the Leader of the House, Ministerial Statements (if any) Up to 90 minutes Referendums (Statutory Instrument) (Motion to Approve) Until 5.00pm General debate: Carers Until 5.30pm or for Adjournment Debate: Section 136 of the Mental Health Act 1983 half an hour (Sir Paul Beresford) WESTMINSTER HALL 1.30pm Stillbirth 3.00pm Refugee family reunion rules CONTENTS PART 1: BUSINESS TODAY 3 Chamber 7 Westminster Hall 8 Committees meeting today 9 Committee reports published today 10 Announcements 13 Further Information PART 2: FUTURE BUSINESS 16 A. Calendar of Business 20 B. Remaining Orders and Notices Notes: Items marked [R] indicates that a Member has declared a relevant interest. BUSINESS TODAY: CHAMBER 9.30am Prayers Followed by QUESTIONS Oral Questions to the Secretary of State for Culture, Media and Sport 1 Stephen Metcalfe (South Basildon and East Thurrock) What steps his Department is taking to ensure the greatest possible engagement by children and young people in the commemoration of the First World War. (905288) 2 Christian Matheson (City of Chester) When part two of the Leveson Inquiry will commence; and if he will make a statement. (905290) 3 Cat Smith (Lancaster and Fleetwood) What steps he is taking to support the tourism sector. (905291) 4 Pauline Latham (Mid Derbyshire) What steps his Department plans to take to increase the level of tourism in England from (a) domestic and (b) foreign visitors. -

Contents Theresa May - the Prime Minister
Contents Theresa May - The Prime Minister .......................................................................................................... 5 Nancy Astor - The first female Member of Parliament to take her seat ................................................ 6 Anne Jenkin - Co-founder Women 2 Win ............................................................................................... 7 Margaret Thatcher – Britain’s first woman Prime Minister .................................................................... 8 Penny Mordaunt – First woman Minister of State for the Armed Forces at the Ministry of Defence ... 9 Lucy Baldwin - Midwifery and safer birth campaigner ......................................................................... 10 Hazel Byford – Conservative Women’s Organisation Chairman 1990 - 1993....................................... 11 Emmeline Pankhurst – Leader of the British Suffragette Movement .................................................. 12 Andrea Leadsom – Leader of House of Commons ................................................................................ 13 Florence Horsbrugh - First woman to move the Address in reply to the King's Speech ...................... 14 Helen Whately – Deputy Chairman of the Conservative Party ............................................................. 15 Gillian Shephard – Chairman of the Association of Conservative Peers ............................................... 16 Dorothy Brant – Suffragette who brought women into Conservative Associations ........................... -
Members of the House of Commons December 2019 Diane ABBOTT MP
Members of the House of Commons December 2019 A Labour Conservative Diane ABBOTT MP Adam AFRIYIE MP Hackney North and Stoke Windsor Newington Labour Conservative Debbie ABRAHAMS MP Imran AHMAD-KHAN Oldham East and MP Saddleworth Wakefield Conservative Conservative Nigel ADAMS MP Nickie AIKEN MP Selby and Ainsty Cities of London and Westminster Conservative Conservative Bim AFOLAMI MP Peter ALDOUS MP Hitchin and Harpenden Waveney A Labour Labour Rushanara ALI MP Mike AMESBURY MP Bethnal Green and Bow Weaver Vale Labour Conservative Tahir ALI MP Sir David AMESS MP Birmingham, Hall Green Southend West Conservative Labour Lucy ALLAN MP Fleur ANDERSON MP Telford Putney Labour Conservative Dr Rosena ALLIN-KHAN Lee ANDERSON MP MP Ashfield Tooting Members of the House of Commons December 2019 A Conservative Conservative Stuart ANDERSON MP Edward ARGAR MP Wolverhampton South Charnwood West Conservative Labour Stuart ANDREW MP Jonathan ASHWORTH Pudsey MP Leicester South Conservative Conservative Caroline ANSELL MP Sarah ATHERTON MP Eastbourne Wrexham Labour Conservative Tonia ANTONIAZZI MP Victoria ATKINS MP Gower Louth and Horncastle B Conservative Conservative Gareth BACON MP Siobhan BAILLIE MP Orpington Stroud Conservative Conservative Richard BACON MP Duncan BAKER MP South Norfolk North Norfolk Conservative Conservative Kemi BADENOCH MP Steve BAKER MP Saffron Walden Wycombe Conservative Conservative Shaun BAILEY MP Harriett BALDWIN MP West Bromwich West West Worcestershire Members of the House of Commons December 2019 B Conservative Conservative -

Parliamentary Debates House of Commons Official Report General Committees
PARLIAMENTARY DEBATES HOUSE OF COMMONS OFFICIAL REPORT GENERAL COMMITTEES Public Bill Committee FISHERIES BILL [LORDS] First Sitting Tuesday 8 September 2020 (Morning) CONTENTS Programme motion agreed to. CLAUSE 1 agreed to, with an amendment. Adjourned till this day at Two o’clock. PBC (Bill 153) 2019 - 2021 No proofs can be supplied. Corrections that Members suggest for the final version of the report should be clearly marked in a copy of the report—not telephoned—and must be received in the Editor’s Room, House of Commons, not later than Saturday 12 September 2020 © Parliamentary Copyright House of Commons 2020 This publication may be reproduced under the terms of the Open Parliament licence, which is published at www.parliament.uk/site-information/copyright/. 1 Public Bill Committee 8 SEPTEMBER 2020 Fisheries Bill [Lords] 2 The Committee consisted of the following Members: Chairs: †STEVE MCCABE,SIR CHARLES WALKER † Bonnar, Steven (Coatbridge, Chryston and Bellshill) † O’Hara, Brendan (Argyll and Bute) (SNP) (SNP) † Owatemi, Taiwo (Coventry North West) (Lab) † Bowie, Andrew (West Aberdeenshire and † Peacock, Stephanie (Barnsley East) (Lab) Kincardine) (Con) † Pollard, Luke (Plymouth, Sutton and Devonport) † Butler, Rob (Aylesbury) (Con) (Lab/Co-op) † Coutinho, Claire (East Surrey) (Con) † Prentis, Victoria (Parliamentary Under-Secretary of † Duffield, Rosie (Canterbury) (Lab) State for Environment, Food and Rural Affairs) † Smith, Cat (Lancaster and Fleetwood) (Lab) † Fletcher, Katherine (South Ribble) (Con) † Wild, James (North West -

Local Needs Issue 3
Local Needs Local Health issue 3 January 2009 Reviewing the way the Trust is shaped Welcome Project support Last summer, we announced plans with our strategic PricewaterhouseCoopers (PWC) has been appointed to health authority, NHS London, to review the way the offer expert advice to the Local Needs, Local Health review. Trust is managed. This is a briefing to update staff, Their role includes helping the project partners to volunteers, patients, local people and other stakeholders understand the financial and clinical implications of the on the latest news from the Local Needs, Local Health three proposed options (status quo, de-merger and review. divestment). They will also help the Trust involve staff, volunteers and other stakeholders in the review process. Involving staff Samantha Jones Plans are being developed to ensure as many staff and Chief Executive volunteers, both clinical and non-clinical, are able to get involved with Local Needs, Local Health, giving them a chance to help shape the review. Project Board All Trust consultants have already been invited to attend a seminar on 23 January, 1pm – 5pm, at Epsom Racecourse. Consultants are asked to confirm their attendance by The first meeting of the Local Needs, Local Health Project emailing [email protected]. Board will take place on 22 January. The Board, which is made up of representatives from the five partner Events for other staff and volunteers will be publicised shortly. organisations, will be asked to formally agree how the review will be run (called the Terms of Reference) and how it will be managed (known as the governance structure). -
Stephen Kinnock MP Aberav
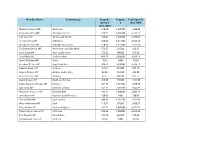
Member Name Constituency Bespoke Postage Total Spend £ Spend £ £ (Incl. VAT) (Incl. VAT) Stephen Kinnock MP Aberavon 318.43 1,220.00 1,538.43 Kirsty Blackman MP Aberdeen North 328.11 6,405.00 6,733.11 Neil Gray MP Airdrie and Shotts 436.97 1,670.00 2,106.97 Leo Docherty MP Aldershot 348.25 3,214.50 3,562.75 Wendy Morton MP Aldridge-Brownhills 220.33 1,535.00 1,755.33 Sir Graham Brady MP Altrincham and Sale West 173.37 225.00 398.37 Mark Tami MP Alyn and Deeside 176.28 700.00 876.28 Nigel Mills MP Amber Valley 489.19 3,050.00 3,539.19 Hywel Williams MP Arfon 18.84 0.00 18.84 Brendan O'Hara MP Argyll and Bute 834.12 5,930.00 6,764.12 Damian Green MP Ashford 32.18 525.00 557.18 Angela Rayner MP Ashton-under-Lyne 82.38 152.50 234.88 Victoria Prentis MP Banbury 67.17 805.00 872.17 David Duguid MP Banff and Buchan 279.65 915.00 1,194.65 Dame Margaret Hodge MP Barking 251.79 1,677.50 1,929.29 Dan Jarvis MP Barnsley Central 542.31 7,102.50 7,644.81 Stephanie Peacock MP Barnsley East 132.14 1,900.00 2,032.14 John Baron MP Basildon and Billericay 130.03 0.00 130.03 Maria Miller MP Basingstoke 209.83 1,187.50 1,397.33 Wera Hobhouse MP Bath 113.57 976.00 1,089.57 Tracy Brabin MP Batley and Spen 262.72 3,050.00 3,312.72 Marsha De Cordova MP Battersea 763.95 7,850.00 8,613.95 Bob Stewart MP Beckenham 157.19 562.50 719.69 Mohammad Yasin MP Bedford 43.34 0.00 43.34 Gavin Robinson MP Belfast East 0.00 0.00 0.00 Paul Maskey MP Belfast West 0.00 0.00 0.00 Neil Coyle MP Bermondsey and Old Southwark 1,114.18 7,622.50 8,736.68 John Lamont MP Berwickshire Roxburgh -

South East Coast
NHS South East Coast New MPs ‐ May 2010 Please note: much of the information in the following biographies has been taken from the websites of the MPs and their political parties. NHS BRIGHTON AND HOVE Mike Weatherley ‐ Hove (Cons) Caroline Lucas ‐ Brighton Pavillion (Green) Leader of the Green Party of England and Qualified as a Chartered Management Wales. Previously Green Party Member Accountant and Chartered Marketeer. of the European Parliament for the South From 1994 to 2000 was part owner of a East of England region. company called Cash Based in She was a member of the European Newhaven. From 2000 to 2005 was Parliament’s Environment, Public Health Financial Controller for Pete Waterman. and Food Safety Committee. Most recently Vice President for Finance and Administration (Europe) for the Has worked for a major UK development world’s largest non-theatrical film licensing agency providing research and policy company. analysis on trade, development and environment issues. Has held various Previously a Borough Councillor in positions in the Green Party since joining in 1986 and is an Crawley. acknowledged expert on climate change, international trade and Has run the London Marathon for the Round Table Children’s Wish peace issues. Foundation and most recently last year completed the London to Vice President of the RSPCA, the Stop the War Coalition, Campaign Brighton bike ride for the British Heart Foundation. Has also Against Climate Change, Railfuture and Environmental Protection completed a charity bike ride for the music therapy provider Nordoff UK. Member of the Campaign for Nuclear Disarmament National Robbins. Council and a Director of the International Forum on Globalization. -

Surrey Mps Urge Natural England to Begin Review of Surrey Hills AONB Boundary
Office of Jonathan Lord MP Surrey MPs urge Natural England to begin review of Surrey Hills AONB boundary ***FOR IMMEDIATE RELEASE*** • Surrey MPs call on Natural England and Defra to protect the Surrey Hills by starting the AONB extension review • Natural England agreed this boundary review in 2014, but is yet to confirm that it will be going ahead • The proposed extension is needed so that this precious area is protected for generations to come under the AONB designation Thursday 22nd October: Surrey MPs, led by Jonathan Lord MP, are urging Natural England to begin the long-awaited review of the proposed extension to the Surrey Hills Area of Outstanding Natural Beauty (AONB). Natural England agreed in 2014 to conduct a boundary review and assured the AONB Board that the Surrey Hills review would be started as soon as a review of Suffolk Coast and Heath had been completed. It has now been completed, but Natural England has not yet confirmed when it will start the Surrey Hills review. And while large areas around the boundary of Surrey Hills AONB have been protected as ‘Areas of Great Landscape Value’ (AGLV) – a local designation which has given a helpful ‘buffer zone’ around the AONB – if Natural England pulls out of the boundary review, all of the AGLVs are in danger of being encroached upon by inappropriate intensification of use or, ultimately, even by development. The MPs have also written today to the Department for Environment, Food and Rural Affairs to urge the Secretary of State to give timely approval to the review, which Natural England agreed to over five years ago. -

Whole Day Download the Hansard
Monday Volume 642 4 June 2018 No. 146 HOUSE OF COMMONS OFFICIAL REPORT PARLIAMENTARY DEBATES (HANSARD) Monday 4 June 2018 © Parliamentary Copyright House of Commons 2018 This publication may be reproduced under the terms of the Open Parliament licence, which is published at www.parliament.uk/site-information/copyright/. HER MAJESTY’S GOVERNMENT MEMBERS OF THE CABINET (FORMED BY THE RT HON. THERESA MAY, MP, JUNE 2017) PRIME MINISTER,FIRST LORD OF THE TREASURY AND MINISTER FOR THE CIVIL SERVICE—The Rt Hon. Theresa May, MP CHANCELLOR OF THE DUCHY OF LANCASTER AND MINISTER FOR THE CABINET OFFICE – The Rt Hon. David Lidington, MP CHANCELLOR OF THE EXCHEQUER—The Rt Hon. Philip Hammond, MP SECRETARY OF STATE FOR THE HOME DEPARTMENT—The Rt Hon. Sajid Javid, MP SECRETARY OF STATE FOR FOREIGN AND COMMONWEALTH AFFAIRS—The Rt Hon. Boris Johnson, MP SECRETARY OF STATE FOR EXITING THE EUROPEAN UNION—The Rt Hon. David Davis, MP SECRETARY OF STATE FOR DEFENCE—The Rt Hon. Gavin Williamson, MP LORD CHANCELLOR AND SECRETARY OF STATE FOR JUSTICE—The Rt Hon. David Gauke, MP SECRETARY OF STATE FOR HEALTH AND SOCIAL CARE—The Rt Hon. Jeremy Hunt, MP SECRETARY OF STATE FOR BUSINESS,ENERGY AND INDUSTRIAL STRATEGY—The Rt Hon. Greg Clark, MP SECRETARY OF STATE FOR HOUSING,COMMUNITIES AND LOCAL GOVERNMENT—The Rt Hon. James Brokenshire, MP SECRETARY OF STATE FOR INTERNATIONAL TRADE AND PRESIDENT OF THE BOARD OF TRADE—The Rt Hon. Liam Fox, MP SECRETARY OF STATE FOR EDUCATION—The Rt Hon. Damian Hinds, MP SECRETARY OF STATE FOR ENVIRONMENT,FOOD AND RURAL AFFAIRS—The Rt Hon.