Xenograft Models of Chronic Lymphocytic Leukemia: Problems, Pitfalls and Future Directions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Contribution of T Cell-Mediated Immunity to the Resistance
0022-202X/ 78/ 7006 0345$02.00/ 0 THE JOURNAL OF I NVESTIGATIVE DERMATOLOGY, 70:345-347, 1978 Vol. 70, No. 6 Copyright © 1978 by The Williams & Wilkins Co. Printed in U.S.A. Contribution ofT Cell-mediated Immunity to the Resistance to Staphylococcal Infection SHINGO TSUDA, M.D., YOICHIRO SASAI, M.D., KIKUO MINAMI, M.D., AND KIKUO NOMOTO, M.D. Department of Dermatology, Kurume University School of Medicine, Kurume, Japan, and Department of Immunology, Institute for Cancer Research, Kyushu University School of Medicine, Fuhuoha, Japan. Abscess formation in nude mice after subcutaneous -, DNase + and hemolysis of a type. The bacteria were cultured in a inoculation of Staphylococcus aureus (S. aureus) was meat infusion broth (distilled water 100 ml, meat extract obtained from more extensive and prolonged as compared with that in beef 5 gm, NaCl5 gm and NaHC03 0.5 gm) at 37°C for 24 hr, centrifuged phenotypically normallittermates. Abscess formation in at 3000 rpm for 30 min and resuspended in saline. Bacterial suspensions comparable to 1.7 x 107 colony-forming markedly by whole-body ir were adjusted to a dose nude mice was augmented units/ ml after estimation with a spectrophotometer at 580 nm (Hita radiation. Not only T cell-mediated immunity but also chi). radiosensitive, nonimmune phagocytosis appear to con tribute to the resistance against staphylococcal infec Procedures for Experimental Infection tion. Each mouse was inoculated subcutaneously with 0.1 ml of bacterial suspension into the back and the infected site was examined macro scopically 1, 2, 3, 5, 7, 10, 14, 21 and 27 days later. -

6510.Full.Pdf
(CANCER RESEARCH 48. 6510-6516. November 15, 1988) Quantitative Studies on the Transplantability of Murine and Human Tumors into the Brain and Subcutaneous Tissues of NCr/Sed Nude Mice1 Anthony L. Zietman, Herman D. Suit,2 Jonathan R. Ramsay, Vlatko Silobrcic, and Robert S. Sedlacek Kdtt'in L. Steele Laboratory for Radiation Biology; Department of Radiation Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 02114 ABSTRACT (5, 6), and cyclophosphamide (7); with use of immunologically immature young animals (8-10); or with transplantation into The transplantability of experimental tumors into the brain (i.e.) and immunologically privileged sites such as the brain (11-13). s.c. tissues of C3Hf/Sed and athymic NCr/Sed nude mice was examined Nude mice, though athymic, do possess small numbers of T- using quantitative cell transplantation assays. Studies using the immune- competent Oil animals showed that brain is a more favorable site for cells (14, 15), which have been shown to be capable of cytotoxic the transplantation of syngeneic tumor than s.c. tissue and that this is allo- and xenoreactivity (16, 17). In addition, their numbers of true for nonimmunogenic as well as immunogenic tumors. The capacity splenic and nodal B-cells have been reported to be normal (9) of the brain to act as an immunological sanctuary can be overwhelmed or higher (15) than that found in hétérozygotes.Theactivity of by a strong, systemic, secondary immune response such as that evoked NK3 cells and peritoneal macrophages may also be higher (15, by the methylcholanthrene-induced sarcoma FSal. In studies performed 18, 19). -

Establishment of Peritoneal and Hepatic Metastasis Mouse
in vivo 33 : 1785-1792 (2019) doi:10.21873/invivo.11669 Establishment of Peritoneal and Hepatic Metastasis Mouse Xenograft Models Using Gastric Cancer Cell Lines TAKASHI MIWA, MITSURO KANDA, SHINICHI UMEDA, HARUYOSHI TANAKA, DAI SHIMIZU, CHIE TANAKA, DAISUKE KOBAYASHI, MASAMICHI HAYASHI, SUGURU YAMADA, GORO NAKAYAMA, MASAHIKO KOIKE and YASUHIRO KODERA Department of Gastroenterological Surgery (Surgery II), Nagoya University Graduate School of Medicine, Nagoya, Japan Abstract. Background/Aim: Establishment of mouse xenograft it is still less than satisfactory in its therapeutic efficacy, models is necessary for oncological research and depends on because some patients with advanced GC often experience the characteristics of the cell lines and the immune system of recurrence even after curative gastrectomy. To develop a the host. In this study, we describe the development of mouse therapeutic strategy, elucidation of the mechanisms of xenograft models using human gastric cancer (GC) cell lines. metastasis formation and identification of therapeutic targets Materials and Methods: MKN1 stably-expressing luciferase are urgently required. (MKN1-Luc), N87, KATO III, MKN45 stably-expressing As previously reported, complex processes such as luciferase (MKN45-Luc), NUGC4, and OCUM-1 human GC invasion into the circulation, survival in the circulation, cell lines were injected intraperitoneally into mice to establish adhesion, migration, invasion and proliferation in other peritoneal metastasis models. MKN45-Luc were injected into organs are necessary for metastasis formation (5). Various subcutaneously implanted spleen, and MKN1-Luc and MKN45- molecules are involved in these processes (5-10). Analysis of Luc were injected directly into the portal veins of mice for the certain molecules and development of therapeutic agents are establishment of hepatic metastasis models. -

Regulatory T Cells
Control of Autoimmune Myocarditis and Multiorgan Inflammation by Glucocorticoid-Induced TNF Receptor Family-Related Protein high, This information is current as Foxp3-Expressing CD25 + and CD25− of September 29, 2021. Regulatory T Cells Masahiro Ono, Jun Shimizu, Yoshiki Miyachi and Shimon Sakaguchi Downloaded from J Immunol 2006; 176:4748-4756; ; doi: 10.4049/jimmunol.176.8.4748 http://www.jimmunol.org/content/176/8/4748 http://www.jimmunol.org/ References This article cites 51 articles, 27 of which you can access for free at: http://www.jimmunol.org/content/176/8/4748.full#ref-list-1 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision by guest on September 29, 2021 • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2006 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Control of Autoimmune Myocarditis and Multiorgan Inflammation by Glucocorticoid-Induced TNF Receptor Family-Related Proteinhigh, Foxp3-Expressing CD25؉ and CD25؊ Regulatory T Cells1 Masahiro Ono,*† Jun Shimizu,‡ Yoshiki Miyachi,† and Shimon Sakaguchi2*§ Anomalies of naturally occurring CD4؉ regulatory T cells (Treg) cause severe autoimmune/inflammatory diseases in humans and rodents. -

Application of Highly Immunocompromised Mice for the Establishment of Patient-Derived Xenograft (PDX) Models
cells Review Application of Highly Immunocompromised Mice for the Establishment of Patient-Derived Xenograft (PDX) Models Seiji Okada 1,2,* , Kulthida Vaeteewoottacharn 1,3,4 and Ryusho Kariya 1 1 Division of Hematopoiesis, Joint Research Center for Human Retrovirus Infection, Kumamoto University, Kumamoto 860-0811, Japan 2 Graduate School of Medical Sciences, Kumamoto University, Kumamoto 860-0811, Japan 3 Department of Biochemistry, Khon Kaen University, Khon Kaen 40002, Thailand 4 Cholangiocarcinoma Research Institute, Khon Kaen University, Khon Kaen 40002, Thailand * Correspondence: [email protected]; Tel.: +81-9-6373-6522 Received: 20 June 2019; Accepted: 9 August 2019; Published: 13 August 2019 Abstract: Patient-derived xenograft (PDX) models are created by engraftment of patient tumor tissues into immunocompetent mice. Since a PDX model retains the characteristics of the primary patient tumor including gene expression profiles and drug responses, it has become the most reliable in vivo human cancer model. The engraftment rate increases with the introduction of Non-obese diabetic Severe combined immunodeficiency (NOD/SCID)-based immunocompromised mice, especially the NK-deficient NOD strains NOD/SCID/interleukin-2 receptor gamma chain(IL2Rγ)null (NOG/NSG) and NOD/SCID/Jak3(Janus kinase 3)null (NOJ). Success rates differ with tumor origin: gastrointestinal tumors acquire a higher engraftment rate, while the rate is lower for breast cancers. Subcutaneous transplantation is the most popular method to establish PDX, but some tumors require specific environments, e.g., orthotropic or renal capsule transplantation. Human hormone treatment is necessary to establish hormone-dependent cancers such as prostate and breast cancers. PDX mice with human hematopoietic and immune systems (humanized PDX) are powerful tools for the analysis of tumor–immune system interaction and evaluation of immunotherapy response. -

Functional Human to Mouse Adipose Tissue Xenotransplantation
41 Functional human to mouse adipose tissue xenotransplantation Vitaly Ablamunits, Simon Klebanov1, Sharon Y Giese2 and Kevan C Herold Department of Immunobiology, Yale University School of Medicine, 300 George Street, Suite 334-D, New Haven, Connecticut, USA 1Obesity Research Center, St. Luke’s Hospital, New York, New York, USA 2Lenox Hill Hospital and Private Ambulatory Clinic, New York, New York, USA (Correspondence should be addressed to V Ablamunits; Email: [email protected]) Abstract White adipose tissue (WAT) produces a number of metabo- human leptin in circulation, reduced body mass gain, and lically important factors and, therefore, some inborn errors of amelioration of hepatic steatosis. Food consumption and metabolism may potentially be corrected by transplantation of plasma insulin levels were reduced only in recipients of 5 ml normal allogeneic WAT.Toexplore the ability of human WAT WAT. Transfer of 2!107 human mononuclear cells to reject (HuWAT) to compensate for a missing factor and to induce WAT as an allograft was ineffective and resulted only in some allogeneic immune response, we created leptin-deficient, reduction of circulating leptin and a limited damage to the immunodeficient mice and transplanted them with either 2.5 WAT grafts followed by the loss of human leukocytes. or 5 ml HuWAT. Recipient mice showed stable levels of Journal of Endocrinology (2012) 212, 41–47 Introduction and how graft rejection can be avoided. We have reported that mouse WAT grafts transplanted into leptin-deficient mice A growing evidence indicates that white adipose tissue may be monitored by reversal of the obese phenotype (WAT) is an important endocrine organ secreting a number (Klebanov et al. -
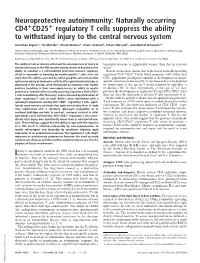
Neuroprotective Autoimmunity: Naturally Occurring CD4 CD25
Neuroprotective autoimmunity: Naturally occurring CD4؉CD25؉ regulatory T cells suppress the ability to withstand injury to the central nervous system Jonathan Kipnis*, Tal Mizrahi*, Ehud Hauben*, Iftach Shaked*, Ethan Shevach†, and Michal Schwartz*‡ *Department of Neurobiology, The Weizmann Institute of Science, 76100 Rehovot, Israel; and †Cellular Immunology Section, Laboratory of Immunology, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, MD 20892 Communicated by Michael Sela, The Weizmann Institute of Science, Rehovot, Israel, September 17, 2002 (received for review June 20, 2002) The ability of rats or mice to withstand the consequences of injury to beneficial outcome is significantly weaker than that in resistant myelinated axons in the CNS was previously shown to depend on the strains? ability to manifest a T cell-mediated protective immune response, Recent studies have shown that depletion of naturally occurring which is amenable to boosting by myelin-specific T cells. Here we regulatory CD4ϩCD25ϩ T cells, which comprise Ϸ10% of the total show that this ability, assessed by retinal ganglion cell survival after CD4ϩ population, predisposes animals to development of organ- optic nerve injury or locomotor activity after spinal cord contusion, is specific autoimmune diseases (9). In rats these cells can be depleted decreased if the animals were immunized as neonates with myelin by thymectomy at the age of 4 weeks followed by split-dose ␥ proteins (resulting in their nonresponsiveness as adults to myelin irradiation (10). In mice, thymectomy at the age of 3–5 days ϩ ϩ proteins) or injected with naturally occurring regulatory CD4؉CD25؉ prevents the development of regulatory T cells (CD4 CD25 ) but T cells immediately after the injury, and is improved by elimination of does not alter the repertoire of effector T cells significantly (11). -

1179.Full.Pdf
Vol. 1. 1 179-i 187, October 1995 Clinical Cancer Research 1179 Elimination of Human Leukemia by Monoclonal Antibodies in an Athymic Nude Mouse Leukemia Model’ Yang Xu and David A. Scheinberg2 pies can be evaluated. Current models are extremely limited: (a) Memorial Sloan-Kettering Cancer Center, New York, A true mouse nonlymphoid leukemia, such as Friend on Raus- cher leukemia (3, 9), is not useful, because the antigen targets of New York 10021 human leukemias are not expressed on mouse cells or in other small animals. (b) Xenogmafted nude mouse tumors have been ABSTRACT proposed (10-13), but these models are not relevant as a model A human acute myeboid leukemia model has been de- of leukemia, because the cells grow as a solid tumor or as veboped by i.v. transplantation of HL-60 myeloid leukemia ascites, and many of the biological and pharmacological issues cells into Swiss nude mice pretreated with cycbophospha- are not addressed. (c) The growth of human cells from AML mide. HL-60 cells disseminated into hematopoietic tissues as patients in the hematopoietic tissues of immunodeficient mice determined by flow cytometric analysis, fluorescence ml- has been described (14, 15). These human leukemia cells were croscopy, fluorescence in situ hybridization analysis, and grown in irradiated SCID mice. This model mimics the human colony formation assay. Passive immunotherapy using mu- disease, but it is less reproducible because it uses fresh human rine anti-CD13 (F23) or anti-CD33 (M195) mAbs was able to cells as opposed to a cell line. Moreover, the mice are heavily eliminate completely the HL-60 cells in the mice, as deter- immunocompromised, which renders their cane and mainte- mined by fluorescence in situ hybridization analysis, colony nance difficult and expensive. -
Grand Rounds Protocol V2
Immunotherapy: A New Era in Cancer Treatment This is to acknowledge that Dr. Deepak Nijhawan M.D. PhD has disclosed that he does not have any financial interests or other relationships with commercial concerns related directly or indirectly to this program. Dr. Nijhawan will not be discussing off-label uses in his presentation. Deepak Nijhawan Assistant Professor Division of Oncology and Department of Biochemistry Dr. Nijhawan supervises a laboratory interested in discovering the mode of action for chemicals that are toxic to cancer cells. These discoveries have the potential to not only unveil new biology, but also lead to potential therapies. Purpose: A review of the discovery and development of immunotherapeutic drugs for cancer. Overview: Drugs that manipulate the immune system have recently been shown to have durable clinical responses in patients with melanoma. In this protocol and presentation, we discuss the scientific and clinical milestones that led to that achievement. Each of these milestones was surrounded by controversy and there are lessons to be learned in how the challenges were overcome. Educational objectives: o Learn the experimental rationale for cancer immunosurveillance o Learn how CTLA-4 was discovered and the rationale for targeting CTLA-4 in cancer o Review clinical trials for immunotherapeutic agents Cancer continues to be a common cause for death, and there is an urgent need for new treatments. Most of our attempts to treat cancer have yielded modest improvement in outcomes measured in weeks to months of prolonged survival. These modest gains are further compromised by severe, sometimes fatal adverse events. For more than a century, it has been proposed that the immune system could be harnessed to fight cancer. -

Oncology Animal Models
Oncology Animal Models The following information provides an overview of Charles River’s Overview portfolio of immunodeficient and immunocompetent oncology animal models. Oncology is one of the leading areas of research into new therapeutics. Due to the challenges inherent Immunodeficient Animal Models in researching and developing anticancer therapeutics, it is critical Immunodeficient animal models are extremely useful in a wide range of that you have the right tools and biomedical research, including infectious disease, stem cell, immunology resources available to you. Backed and oncology studies. Due to the unique vulnerability that makes these by decades of technical, scientific models vital to research, their care and maintenance demands a high and veterinary experience, Charles level of expertise and technological resources. River’s global portfolio of high-quality oncology models gives you the T-Cell B-Cell NK Cell benefit of partnering with an industry Strain Hair Deficient Deficient Deficient leader offering an infrastructure Athymic Nude Mouse No Yes No No capable of advancing your research CD-1® Nude Mouse No Yes No No now and in the future. Swiss Nude Mouse No Yes No No BALB/c Nude Mouse No Yes No No NMRI Nude Mouse Yes Yes No No NIH-III Mouse No Yes Yes Impaired RNU Rat No Yes No No SCID Hairless Outbred No Yes Yes No (SHO®) Mouse SCID Hairless Congenic No Yes Yes No (SHC™) Mouse Fox Chase SCID® Congenic Yes Yes Yes No Mouse Fox Chase SCID® Yes Yes Yes Impaired Beige Mouse NOD SCID Mouse Yes Yes Yes Impaired NOD scid gamma (NSG) Yes Yes Yes Yes Mouse Nude Models Athymic Nude Mouse Nomenclature: Crl:NU(NCr)-Foxn1nu Origin: This immunodeficient nude mouse originated from NIH and was originally thought to be a BALB/c congenic. -

In Vitro Expanded CD4 CD25 Foxp3 Regulatory T Cells Maintain A
In Vitro Expanded CD4؉CD25؉Foxp3؉ Regulatory T Cells Maintain a Normal Phenotype and Suppress Immune-Mediated Ocular Surface Inflammation Karyn F. Siemasko,1 Jianping Gao,1 Virginia L. Calder,2 Rebecca Hanna,1 Margarita Calonge,3 Stephen C. Pflugfelder,4 Jerry Y. Niederkorn,5 and Michael E. Stern1,4 PURPOSE. To determine whether in vitro expanded of autoimmune and inflammatory diseases, but determination CD4ϩCD25ϩFoxp3ϩ regulatory T cells can suppress immune- of the mechanism of this suppression was limited because of mediated ocular surface inflammation in a mouse model of dry the low percentage of regulatory T cells present in vivo. eye. CD4ϩCD25ϩFoxp3ϩ regulatory T cells make up 5% to 10% of ϩ 1–5 METHODS. C57BL/6 or BALB/c mice were exposed to a dry, the mouse CD4 T-cell population. Because of this low cell desiccating environment produced by maintaining low humid- number and the inherent cell loss in the isolation process, ity (Ͻ40%), injections of scopolamine, and air flow produced mouse regulatory T cells were expanded in vitro to examine by a fan. CD4ϩCD25ϩ regulatory T cells were isolated and the mechanisms used by the cells to maintain an immune- expanded in vitro in the presence of rmIL-2 and beads coated tolerant environment on the ocular surface. with anti-CD28 and anti-CD3. In vitro expanded regulatory T Dry eye affects Ͼ10% of the population within the age cells were phenotypically compared with freshly isolated reg- range of 30 to 60 and Ͼ15% of the population over 65 years of ulatory T cells by flow cytometry and immunofluorescence. -

Immunodeficient Mouse Models: an Overview José E
The Open Immunology Journal, 2009, 2, 79-85 79 Open Access Immunodeficient Mouse Models: An Overview José E. Belizário* Department of Pharmacology, Institute of Biomedical Sciences, University of São Paulo, SP, CEP 05508-900, Brazil Abstract: The development and use of an increasing number and variety of naturally, transgenic, induced mutant, and genetically engineered immunodeficient mouse and mouse/human hybrids models have been imperative for understanding the gene-driven cellular and molecular mechanisms and pathophysiological manifestations (phenotypes) of immune disorders that are similar to mice and humans. Much more effort is needed to develop new system models to promote the integration of thousands of genes and their variants that are likely to affect the outcome of microbial infections, immune deficiency and autoimmunity. This article provides an update on characteristics and applications of most commonly used inbred and new hybrid strains of naturally immunodeficiency, knockout and transgenic mouse models, and a short discussion on how innovative technologies and databases presently available can be used for devising new models to better understand the human immune system and diseases that affect it. Keywords: Animal models, immune system, immunodeficiency, xenografts. INTRODUCTION There is a relatively high number of strains and sub- strains of natural immunodeficiency models and gene Modeling the immune response and rational immune deficient transgenic models available for genetic and approaches in vivo have relied heavily on basic studies immunological studies [http://www.jax.org/pub-cgi/imsrlist, performed in transgenic and immunodeficient mice models [1]. http://imsr.har.mrc.ac.uk/, http://www.apf.edu.au/index.shtml, The creation of chimaeras of mouse-human models that http://www.brc.riken.jp/lab/animal/en].