Acute Appendicitis Leading to Small and Large Bowel Obstruction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Print This Article
International Surgery Journal Lew D et al. Int Surg J. 2021 May;8(5):1575-1578 http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902 DOI: https://dx.doi.org/10.18203/2349-2902.isj20211831 Case Report Acute gangrenous appendicitis and acute gangrenous cholecystitis in a pregnant patient, a difficult diagnosis: a case report David Lew, Jane Tian*, Martine A. Louis, Darshak Shah Department of Surgery, Flushing Hospital Medical Center, Flushing, New York, USA Received: 26 February 2021 Accepted: 02 April 2021 *Correspondence: Dr. Jane Tian, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Abdominal pain is a common complaint in pregnancy, especially given the physiological and anatomical changes that occur as the pregnancy progresses. The diagnosis and treatment of common surgical pathologies can therefore be difficult and limited by the special considerations for the fetus. While uncommon in the general population, concurrent or subsequent disease processes should be considered in the pregnant patient. We present the case of a 36 year old, 13 weeks pregnant female who presented with both acute appendicitis and acute cholecystitis. Keywords: Appendicitis, Cholecystitis, Pregnancy, Pregnant INTRODUCTION population is rare.5 Here we report a case of concurrent appendicitis and cholecystitis in a pregnant woman. General surgeons are often called to evaluate patients with abdominal pain. The differential diagnosis list must CASE REPORT be expanded in pregnant woman and the approach to diagnosing and treating certain diseases must also be A 36 year old, 13 weeks pregnant female (G2P1001) adjusted to prevent harm to the fetus. -

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

ACUTE Yellow Atrophy Ofthe Liver Is a Rare Disease; Ac
ACUTE YELLOW ATROPHY OF THE LIVER AS A SEQUELA TO APPENDECTOMY.' BY MAX BALLIN, M.D., OF DETROIT, MICHIGAN. ACUTE yellow atrophy of the liver is a rare disease; ac- cording to Osler about 250 cases are on record. This affection is also called Icterus gravis, Fatal icterus, Pernicious jaundice, Acute diffuse hepatitis, Hepatic insufficiency, etc. Acute yellow atrophy of the liver is characterized by a more or less sudden onset of icterus increasing to the severest form, headaches. insomnia, violent delirium, spasms, and coma. There are often cutaneous and mucous hiemorrhages. The temperature is usually high and irregular. The pulse, first normal, later rapid; urine contains bile pigments, albumen, casts, and products of incomplete metabolism of albumen, leucin, and tyrosin, the pres- ence of which is considered pathognomonic. The affection ends mostly fatally, but there are recoveries on record. The findings of the post-mortem are: liver reduced in size; cut surface mot- tled yellow, sometimes with red spots (red atrophy), the paren- chyma softened and friable; microscopically the liver shows biliary infiltration, cells in all stages of degeneration. Further, we find parenchymatous nephritis, large spleen, degeneration of muscles, haemorrhages in mucous and serous membranes. The etiology of this affection is not quite clear. We find the same changes in phosphorus poisoning; many believe it to be of toxic origin, but others consider it to be of an infectious nature; and we have even findings of specific germs (Klebs, Tomkins), of streptococci (Nepveu), staphylococci (Bourdil- lier), and also the Bacillus coli is found (Mintz) in the affected organs. The disease seems to occur always secondary to some other ailment, and is observed mostly during pregnancy (about one-third of all cases, hence the predominance in women), after Read before the Wayne County Medical Society, January 5, I903. -

A Case Report of Fibro-Stenotic Crohn's Disease in the Middle
DOI: https://doi.org/10.22516/25007440.185 Case report A Case Report of Fibro-Stenotic Crohn’s Disease in the Middle Ileum as the Initial Manifestation Adriana Margarita Rey,1 Gustavo Reyes,1 Fernando Sierra,1 Rafael García-Duperly,2 Rocío López,3 Leidy Paola Prada.4 1 Gastroenterologist in the Gastroenterology and Abstract Hepatology Service of the Hospital Universitario Fundación Santa Fe de Bogotá in Bogotá, Colombia Crohn’s disease (CD) is an inflammatory bowel disease that can affect the entire gastrointestinal tract. The small 2 Colon and Rectum Surgeon in the Department of intestine is affected in about 50% of patients among whom the terminal ileum is the area most commonly affected. Surgery of the Hospital Universitario Fundación Intestinal stenosis is a common complication in CD and approximately 30% to 50% of patients present Santa Fe de Bogotá in Bogotá, Colombia 3 Pathologist at of the Hospital Universitario Fundación stenosis or penetrating lesions at the time of diagnosis. Because conventional endoscopic techniques do not Santa Fe de Bogotá and Professor at Universidad de allow evaluation of small bowel lesions, techniques such as enteroscopy and endoscopic video-capsule were los Andes in Bogotá, Colombia developed. Each has advantages and indications. 4 Third Year Internal Medicine Resident at the Hospital Universitario Fundación Santa Fe de Bogotá in We present the case of a patient with CD with localized fibrostenosis in the middle ileum which is not a Bogotá, Colombia frequent site for this type of lesion. Author for correspondence: Adriana Margarita Rey. Bogotá D.C. Colombia [email protected] Keywords ........................................ -

Adult Intussusception
1 Adult Intussusception Saulius Paskauskas and Dainius Pavalkis Lithuanian University of Health Sciences Kaunas Lithuania 1. Introduction Intussusception is defined as the invagination of one segment of the gastrointestinal tract and its mesentery (intussusceptum) into the lumen of an adjacent distal segment of the gastrointestinal tract (intussuscipiens). Sliding within the bowel is propelled by intestinal peristalsis and may lead to intestinal obstruction and ischemia. Adult intussusception is a rare condition wich can occur in any site of gastrointestinal tract from stomach to rectum. It represents only about 5% of all intussusceptions (Agha, 1986) and causes 1-5% of all cases of intestinal obstructions (Begos et al., 1997; Eisen et al., 1999). Intussusception accounts for 0.003–0.02% of all hospital admissions (Weilbaecher et al., 1971). The mean age for intussusception in adults is 50 years, and and the male-to-female ratio is 1:1.3 (Rathore et. al., 2006). The child to adult ratio is more than 20:1. The condition is found in less than 1 in 1300 abdominal operations and 1 in 100 patients operated for intestinal obstruction. Intussusception in adults occurs less frequently in the colon than in the small bowel (Zubaidi et al., 2006; Wang et al., 2007). Mortality for adult intussusceptions increases from 8.7% for the benign lesions to 52.4% for the malignant variety (Azar & Berger, 1997) 2. Etiology of adult intussusception Unlike children where most cases are idiopathic, intussusception in adults has an identifiable etiology in 80- 90% of cases. The etiology of intussusception of the stomach, small bowel and the colon is quite different (Table 1). -
Recognizing-Consitpation-And-Bowel
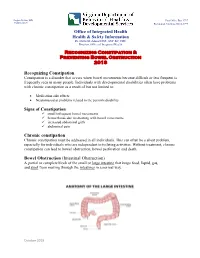
Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Office of Integrated Health Health & Safety Information Dr. Dawn M. Adams DNP, ANP-BC, CHC Director, Office of Integrated Health Recognizing Constipation & Preventing Bowel Obstruction 2018 Recognizing Constipation Constipation is a disorder that occurs when bowel movements become difficult or less frequent is frequently seen in many people. Individuals with developmental disabilities often have problems with chronic constipation as a result of but not limited to: Medication side effects Neuromuscular problems related to the person's disability Signs of Constipation small infrequent bowel movements hemorrhoids due to straining with bowel movements increased abdominal girth abdominal pain Chronic constipation Chronic constipation must be addressed in all individuals. This can often be a silent problem, especially for individuals who are independent in toileting activities. Without treatment, chronic constipation can lead to bowel obstruction, bowel perforation and death. Bowel Obstruction (Intestinal Obstruction) A partial or complete block of the small or large intestine that keeps food, liquid, gas, and stool from moving through the intestines in a normal way. October 2018 Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Bowel obstructions may be caused by a twist in the intestines. Intestines are called the gut. The large intestine includes the appendix, cecum, colon, and rectum and is 5 feet long. It absorbs water from stool and changes it from a liquid to a solid form. The small intestine is where most digestion occurs. It measures about 20 feet and includes the duodenum, jejunum, and ileum. o Digestion is the process of breaking down food into substances the body can use for energy, tissue growth, and repair. -

Case Report Perforated Acute Appendicitis Misdiagnosed As Colonic Perforation in Colon Cancer Patients After Colonoscopy: a Report of Two Cases and Literature Reviews
Int J Clin Exp Pathol 2017;10(6):7256-7260 www.ijcep.com /ISSN:1936-2625/IJCEP0050313 Case Report Perforated acute appendicitis misdiagnosed as colonic perforation in colon cancer patients after colonoscopy: a report of two cases and literature reviews Kaiyuan Zheng, Ji Wang, Wenhao Lv, Yongjia Yan, Zhicheng Zhao, Weidong Li, Weihua Fu Department of General Surgery, Tianjin Medical University General Hospital, Tianjin 300052, China Received January 23, 2017; Accepted May 9, 2017; Epub June 1, 2017; Published June 15, 2017 Abstract: Free gas in the abdominal cavity usually indicates that the perforation of the gastrointestinal tract from many factors including perforated ulcer, tumor perforation and severe infection, etc. But the pneumoperitoneum in perforated acute appendix secondary to the colonoscopy was rare relative. We reported two colon cancer patients with signs of abdominal free air after the operation of colonoscopy, considered the diagnosis of colon perforation at first, but eventually they were confirmed as perforated appendicitis. This report highlights that purulent perforated appendicitis should be considered especially for elderly patients with colon tumor presenting as signs of pneumo- peritoneum after the endoscopic operation. Keywords: Pneumoperitoneum, perforated appendicitis, colon cancer perforation, colonoscopy Introduction Acute perforated appendicitis is one of the common causes of acute abdomen and is Pneumoperitoneum is defined as free gas ap- needed emergency surgery. Its incidence was pears in the abdominal cavity, is usually caused higher in elderly population [6]. However, acute by the perforation of the alimentary tract sec- appendicitis following the operation of colonos- ondary to pathological or iatrogenic factors, but copy as a rare complication, with a consider- caused by purulent perforated appendix was ed incidence of 0.038%, and the appendix is rare relative. -

Patient Selection Criteria
M∙ACS MACS Patient Selection Criteria The objective is to screen, on a daily basis, the Acute Care Surgical service “touches” at your hospital to identify patients who meet criteria for further data entry. The specific patient diseases/conditions that we are interested in capturing for emergent general surgery (EGS) are: 1. Acute Appendicitis 2. Acute Gallbladder Disease a. Acute Cholecystitis b. Choledocholithiasis c. Cholangitis d. Gallstone Pancreatitis 3. Small Bowel Obstruction a. Adhesive b. Hernia 4. Emergent Exploratory Laparotomy (Refer to the ex-lap algorithm under the Diseases or Conditions section below for inclusion/exclusion criteria.) The daily census for patients admitted to the Acute Care Surgery Service or seen as a consult will have to be screened. There may be other sources to accomplish this screening such as IT and we are interested in learning about these sources from you. From this census, a list can be compiled of patients with the aforementioned diseases/conditions. The first level of data entry involves capture and entry of the patient into the MACS Qualtrics database. All patients with the identified diseases/conditions will have data entered regardless of whether or not they received an operation during admission/ED visit. The second level of data entry takes place if an existing MACS patient returns to the hospital (ED or admission) or has outcome events identified within the 30-day post-operative time frame if the patient had surgery, or within 30 days from discharge for the non-operative patients. You will see that we are capturing diagnostic, interventional, and therapeutic data that extend beyond what is typically captured for MSQC patients. -

Crohn's Disease Manifesting As Acute Appendicitis: Case Report and Review of the Literature
Case Report World Journal of Surgery and Surgical Research Published: 20 Jan, 2020 Crohn's Disease Manifesting as Acute Appendicitis: Case Report and Review of the Literature Terrazas-Espitia Francisco1*, Molina-Dávila David1, Pérez-Benítez Omar2, Espinosa-Dorado Rodrigo2 and Zárate-Osorno Alejandra3 1Division of Digestive Surgery, Hospital Español, Mexico 2Department of General Surgery Resident, Hospital Español, Mexico 3Department of Pathology, Hospital Español, Mexico Abstract Crohn’s Disease (CD) is one of the two clinical presentations of Inflammatory Bowel Disease (IBD) which involves the GI tract from the mouth to the anus, presenting a transmural pattern of inflammation. CD has been described as being a heterogenous disorder with multifactorial etiology. The diagnosis is based on anamnesis, physical examination, laboratory finding, imaging and endoscopic findings. There have been less than 200 cases of Crohn’s disease confined to the appendix since it was first described by Meyerding and Bertram in 1953. We present the case of a 24 year old male, who presented with acute onset, right lower quadrant pain, mimicking acute appendicitis with histopathological report of Crohn’s disease confined to the appendix. Introduction Crohn’s Disease (CD) is a chronic entity which clinical diagnosis represents one of the two main presentations of Inflammatory Bowel Disease (IBD), and it occurs throughout the gastrointestinal tract from the mouth to the anus, presenting a transmural pattern of inflammation of the gastrointestinal wall and non-caseating small granulomas. The exact origin of the disease remains OPEN ACCESS unknown, but it has been proposed as an interaction of genetic predisposition, environmental risk *Correspondence: factors and immune dysregulation of intestinal microbiota [1,2]. -

MANAGEMENT of ACUTE ABDOMINAL PAIN Patrick Mcgonagill, MD, FACS 4/7/21 DISCLOSURES
MANAGEMENT OF ACUTE ABDOMINAL PAIN Patrick McGonagill, MD, FACS 4/7/21 DISCLOSURES • I have no pertinent conflicts of interest to disclose OBJECTIVES • Define the pathophysiology of abdominal pain • Identify specific patterns of abdominal pain on history and physical examination that suggest common surgical problems • Explore indications for imaging and escalation of care ACKNOWLEDGEMENTS (1) HISTORICAL VIGNETTE (2) • “The general rule can be laid down that the majority of severe abdominal pains that ensue in patients who have been previously fairly well, and that last as long as six hours, are caused by conditions of surgical import.” ~Cope’s Early Diagnosis of the Acute Abdomen, 21st ed. BASIC PRINCIPLES OF THE DIAGNOSIS AND SURGICAL MANAGEMENT OF ABDOMINAL PAIN • Listen to your (and the patient’s) gut. A well honed “Spidey Sense” will get you far. • Management of intraabdominal surgical problems are time sensitive • Narcotics will not mask peritonitis • Urgent need for surgery often will depend on vitals and hemodynamics • If in doubt, reach out to your friendly neighborhood surgeon. Septic Pain Sepsis Death Shock PATHOPHYSIOLOGY OF ABDOMINAL PAIN VISCERAL PAIN • Severe distension or strong contraction of intraabdominal structure • Poorly localized • Typically occurs in the midline of the abdomen • Seems to follow an embryological pattern • Foregut – epigastrium • Midgut – periumbilical • Hindgut – suprapubic/pelvic/lower back PARIETAL/SOMATIC PAIN • Caused by direct stimulation/irritation of parietal peritoneum • Leads to localized -

Small Bowel Obstruction Following Appendectomy: a Retrospective Study
New Indian Journal of Surgery21 Original Article January - March 2012, Volume 3 Number 1 Small Bowel Obstruction Following Appendectomy: A Retrospective Study Jyothi S Karegoudar*, Prabhakar PJ**, Rajashri S Patil***, VIjayanath V**** *Asso. Prof in General Surgery, ** Prof & HOD in General Surgery, ***Asst. Prof (biostatistician), S. S. I. M. S & R. C., Davangere, Karnataka State, ****MD, DNB, MNAMS, Associate Professor, Department of Forensic Medicine & Toxicology, Vinayaka Mission’s Kirupananda Variyar Medical College & Hospital, Salem,Tamil Nadu, India. Abstract appendectomy adhesive small bowel The incidence of post-operative small bowel obstruction occurs in 1 to 1.5% of all patients obstruction after standard, open appendectomy was within 14 years of the operation.[1] calculated during five year duration at S. S. Institute Appendectomy is one of the most frequently and Research Centre, Davangere, Karnataka State. performed emergency surgery, and it is Post-operative small bowel obstruction is one of associated with various short and long term the adverse effects of appendectomy but its frequency morbidities. Postoperative small bowel varies from centre to centre. The incidence of small obstruction is recognized as long term adverse bowel obstruction is significantly high in perforated effect of appendectomy.[2] appendicitis, midline incisions, and chronic appendicular pathology. The midline incision has The frequency of this complication is not increased the frequency of post-operative adhesions. well known but the reported risk ranges from This study was conducted to determine the 0.2- 10.7%.[3] The post-operative adhesions incidence of this complication among our patients are a significant problem after colorectal who had open appendectomy and identify the factors surgery. -

Problems in Family Practice Acute Abdominal Pain in Children
dysuria. The older child may start bed wetting with or without dysuria. A problems in Family Practice drop of fresh, clean unspun urine will usually reveal pyuria, but in the early case relatively few white blood cells may be seen compared to gross bacillu- Acute Abdominal Pain ria. The infection may have underlying urinary tract abnormality, stone, in Children hydronephrosis, polycystic kidney or renal neoplasms. The IVP is important Hyman Shrand, M D in detecting these underlying prob lems. Cambridge, M assachusetts 4. Viral Hepatitis. Malaise, anorexia, abdominal pain, and tenderness over Acute abdominal pain in children is a common and challenging prob the liver occur with hepatitis A or B. lem for the family physician. The many causes of this problem require Later, patients who become jaundiced a systematic approach to making the diagnosis and planning specific have dark urine and pale stools. In therapy. A careful history and physical examination, together with a teenagers, “needle tracks” suggest sy ringe transmitted Type B (H.A.A.) small number of selected laboratory studies, provide a rational basis hepatitis. Youngsters with infectious for effective management in most cases. This paper reviews the more mononucleosis may present as hepati common causes of acute abdominal pain in children with special em tis. phasis on their clinical differentiation. 5. Upper Respiratory Tract. Strepto coccal pharyngitis, a common cause of Abdominal pain in a child is always followed by vomiting is more likely an vomiting and abdominal pain, can be an emergency. The primary physician intra-abdominal disorder. recognized by looking at the throat must identify a “medical” cause in or with confirmatory throat culture.