Concurrent Session Presentations (Pdf)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Acral Lick Granuloma
Acral Lick Granuloma Also Known As: Acral lick dermatitis, acral lick furunculosis, lick granuloma Transmission or Cause: The causes of acral lick granulomas include infections caused by bacteria, fungi, or mites; allergies, cancer, joint disease, or previous trauma; or an obsessive-compulsive disorder caused by boredom in some dogs. Dogs are provoked by these conditions to lick an area until they cause hair loss and erosion of the superficial skin layers. The consequence is further inflammation, which then results in more licking. With time, excessive licking can cause secondary infections, thickening of the skin, and changes in skin-color. Affected Animals: Acral lick granulomas may affect dogs of any breed and gender, however, males and dogs that are five years and older are more often affected. Breeds predisposed to this condition include Great Dane, Doberman Pinscher, Labrador Retriever, Golden Retriever, German Shepherd, and Irish Setter. Overview: A commonly seen skin disorder of dogs, acral lick granulomas are skin wounds that are worsened by a dog's constant licking of the affected area. Because the repeated licking hinders healing of the lesion, dogs must be prevented from licking the area until the wound has healed completely. Acral lick granulomas have a wide variety of possible causes. The disease is often bothersome to pets as well as their owners. A veterinarian can implement appropriate medical therapies to treat the lick granuloma and to prevent recurrence. Clinical Signs: Lick granulomas are skin wounds typically located on the lower portion of the front or hind leg of a dog. Some dogs may have more than one area affected at a time. -

Species List 02/11/2017
1 of 27 Kelvingrove Park - species list 02/11/2017 Group Taxon Common Name Earliest Latest Records acarine Hydracarina 2004 2004 1 amphibian Bufo bufo Common Toad 2014 2014 2 amphibian Lissotriton helveticus Palmate Newt 2006 2006 1 amphibian Lissotriton vulgaris Smooth Newt 1997 1997 1 amphibian Rana temporaria Common Frog 2009 2017 6 annelid Alboglossiphonia heteroclita 2003 2004 2 annelid Erpobdella testacea 2003 2003 1 annelid Glossiphonia complanata 2003 2003 1 annelid Helobdella stagnalis 2003 2014 3 annelid Lumbricus terrestris Common Earthworm 1996 2000 1 annelid Naididae 2004 2004 1 annelid Tubificidae Tubificid Worm Sp. 2003 2004 2 bird Acanthis flammea Common (Mealy) Redpoll 1991 1991 1 bird Accipiter nisus Sparrowhawk 1983 2008 7 bird Aegithalos caudatus Long-tailed Tit 1991 2017 16 bird Aix galericulata Mandarin Duck 1969 1969 1 bird Alcedo atthis Kingfisher 1988 2017 27 bird Anas penelope Wigeon 1994 1994 1 bird Anas platyrhynchos Mallard 1968 2014 246 bird Anser anser Greylag Goose 1973 1973 1 bird Apus apus Swift 2008 2014 4 bird Ardea cinerea Grey Heron 1991 2014 28 bird Aythya ferina Pochard 1939 1994 10 bird Aythya fuligula Tufted Duck 1992 2004 16 bird Bucephala clangula Goldeneye 1991 2006 59 bird Carduelis carduelis Goldfinch 1998 2014 12 bird Certhia familiaris Treecreeper 1995 2017 11 bird Chloris chloris Greenfinch 1988 2016 7 bird Chroicocephalus ridibundus Black-headed Gull 1961 2014 16 bird Cinclus cinclus Dipper 1991 2014 8 bird Columba livia Feral Pigeon 1958 2015 21 bird Columba oenas Stock Dove 2014 2015 2 bird Columba palumbus Woodpigeon 2014 2014 7 bird Corvus corone Carrion Crow 2014 2014 1 2 of 27 Kelvingrove Park - species list 02/11/2017 Group Taxon Common Name Earliest Latest Records bird Corvus corone agg. -

Student Organization List 2020-2021 Academic Year (Past)
Student Organization List 2020-2021 Academic Year (past) ALPHABETICAL ORDER Group Name Group Acronym Group Type Organization Type (not so) Average Women NotSoAvWomen Undergraduate Student Organization Independent 14Strings! Cornell Filipino Rondalla 14Strings Undergraduate Student Organization Independent 180 Degrees Consulting at Cornell 180dcCornell Undergraduate Student Organization Independent University 3 Day Startup, Cornell 3DS Undergraduate Student Organization Independent 302 Wait Avenue Co-op 302 Undergraduate Student Organization University A Cappella Advisory Council ACAC Undergraduate Student Organization Independent A Seat at the Table ASATT Undergraduate Student Organization Independent A.G. Musical Theatre Troupe AnythingGoes Undergraduate Student Organization Independent AAP - Cornell AAP ASSOCIATION ASSOCIATION Undergraduate Student Organization Independent Absolute A Cappella Absolute Undergraduate Student Organization Independent Absolute Zero Break Dance Club AZero Undergraduate Student Organization Independent Academy FC, Cornell (CAFC) AcademyFC Undergraduate Student Organization Independent Accounting Association, Cornell CAA Undergraduate Student Organization University ACE: The Ace/Asexual Support Group at ACE Undergraduate Student Organization University Cornell Actuarial Society, Cornell CAS Undergraduate Student Organization University Graduate/Professional Student Advancing Science And Policy ASAP Independent Organization Advent Christian Fellowship, Cornell ACF Undergraduate Student Organization Independent -

Dermatology Appointment Compliance 10 Common Characteristics Ofhighly Successful Practices Keith a Hnilica DVM, MS, DACVD
Better Dermatology Appointment Compliance 10 Common Characteristics ofHighly Successful Practices Keith A Hnilica DVM, MS, DACVD Who am I to decide: I am a veterinary dermatologist currently enrolled in an MBA program. During the last year, I have had the wonderful opportunity to visit dozens of great practices (through the Novartis LEAD and Pfizer’s Partners for Success programs). During these visits, I was able to learn many lessons from successful practices. In addition, I have listened to many practice managers, sales reps, and business people much smarter than myself. What I have learned is that there are common behaviors that are found in most of the truly great clinics: THIS is THAT list. Immutable Lessons from the Road: 1. All staff members are motivated to solve specific client problems with practice specific protocols formulated to implement the “Best in Class” treatment options. 2. The mission statement includes a commitment to the highest quality of practice (not the cheapest). 3. Staff rounds are conducted to educate everyone in the clinic on the most common diseases and the practice’s protocols treatment. 4. All staff provides consistent client education and treatment recommendations: the same message from the front to the back of the practice. 5. The doctors are removed from all treatment cost discussions: decisions are made based on medical appropriateness not negotiated based on cost. 6. Follow up counts. 7. Technicians are used to their full potential: great knowledge, tremendous ability, and enthusiasm produce an effective patient advocate that functions like a physician’s assistant. 8. The receptions are recognized as the store front window of the practice. -

Zbornik Refera Zbornik Referatov Xxiii. Simpozij O
ZBORNIK REFERATOV XXIII. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH @IVALI Dolenjske Toplice, 22. - 24. april 2010 1 XXIII. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH @IVALI ZBORNIK REFERATOV Dolenjske Toplice, 22. - 24. april 2010 2 ZBORNIK REFERATOV XXIII. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH @IVALI Dolenjske Toplice, 22. - 24. april 2010 SLOVENSKO ZDRU@ENJE VETERINARJEV ZA MALE @IVALI SLOVENIAN SMALL ANIMAL VETERINARY ASSOCIATION ZBORNIK REFERATOV XXIII. SIMPOZIJA O AKTUALNIH BOLEZNIH MALIH @IVALI http://www.zdruzenje-szvmz.si/ 3 XXIII. SIMPOZIJ O AKTUALNIH BOLEZNIH MALIH @IVALI ZBORNIK REFERATOV Dolenjske Toplice, 22. - 24. april 2010 VSEBINA Hackett T: The critical cat – Triage, vascular access and emergency treament ............................. 7 Hackett T: Feline shock – The unique challenges of treating cats ............................................... 11 Romagnoli S: Feline pediatrics ................................................................................................... 13 Romagnoli S: Techniques for neonatal resuscitation and critical care ........................................ 18 Hackett T: Managing the dyspneic cat – Case studies in feline respiratory distress .................... 23 Hackett T: Feline trauma ........................................................................................................... 26 Romagnoli S: Practical use of hormones in feline reproduction ................................................. 29 Romagnoli S: Ovarian remnant syndrome in the queen: Clinical approach to a surgeon’s dilemma -

Zoonotic Diseases Associated with Free-Roaming Cats R
Zoonoses and Public Health REVIEW ARTICLE Zoonotic Diseases Associated with Free-Roaming Cats R. W. Gerhold1 and D. A. Jessup2 1 Center for Wildlife Health, Department of Forestry, Wildlife, and Fisheries, The University of Tennessee, Knoxville, TN, USA 2 California Department of Fish and Game (retired), Santa Cruz, CA, USA Impacts • Free-roaming cats are an important source of zoonotic diseases including rabies, Toxoplasma gondii, cutaneous larval migrans, tularemia and plague. • Free-roaming cats account for the most cases of human rabies exposure among domestic animals and account for approximately 1/3 of rabies post- exposure prophylaxis treatments in humans in the United States. • Trap–neuter–release (TNR) programmes may lead to increased naı¨ve populations of cats that can serve as a source of zoonotic diseases. Keywords: Summary Cutaneous larval migrans; free-roaming cats; rabies; toxoplasmosis; zoonoses Free-roaming cat populations have been identified as a significant public health threat and are a source for several zoonotic diseases including rabies, Correspondence: toxoplasmosis, cutaneous larval migrans because of various nematode parasites, R. Gerhold. Center for Wildlife Health, plague, tularemia and murine typhus. Several of these diseases are reported to Department of Forestry, Wildlife, and cause mortality in humans and can cause other important health issues includ- Fisheries, The University of Tennessee, ing abortion, blindness, pruritic skin rashes and other various symptoms. A Knoxville, TN 37996-4563, USA. Tel.: 865 974 0465; Fax: 865-974-0465; E-mail: recent case of rabies in a young girl from California that likely was transmitted [email protected] by a free-roaming cat underscores that free-roaming cats can be a source of zoonotic diseases. -

Flea Control in Cats Where Did My Cat Get Fleas? the Most Common Flea
Flea Control in Cats Where did my cat get fleas? The most common flea found on cats and dogs is the cat flea (Ctenocephalides felis), although any species of fleas, including fleas from rabbits, squirrels or other wildlife, can be found on cats. The most important source of cat fleas is newly emerged adult fleas from flea pupae in your house or yard. Adult fleas live, feed and mate on our pets; the female flea lays eggs that fall off into the environment where they hatch into larvae. The larvae eat organic debris until they mature into pupae. The pupae are encased in a sticky cocoon, helping them to camouflage in the environment and making them difficult to eradicate. Adult fleas will not emerge from the pupae until they sense an animal nearby to feed on. Newly hatched adult fleas jump onto a host animal to complete their life cycle. Two days after eating a blood meal from the host, the female flea begins to lay eggs. Under ideal conditions, the flea can complete its entire life cycle in as little as two weeks; in adverse conditions, the fleas within the pupae remain dormant, and can wait as much as a year to hatch, when conditions are more desirable. Homes with carpets and central heating provide ideal conditions for the year-round development of fleas. The highest numbers of flea eggs, larvae and pupae will be found in areas of the house where pets spend the most time, such as their beds and furniture. Even though fleas may be in your house, you probably won't see them. -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Veterinary Public Health
Veterinary Public Health - MPH Increasing focus on zoonotic diseases, foodborne illness, public health preparedness, antibiotic resistance, the human-animal bond, and environmental health has dramatically increased opportunities for public health veterinarians - professionals who address key issues surrounding human and animal health. Adding the MPH to your DVM degree positions you to work at the interface of human wellness and animal health, spanning agriculture and food industry concerns, emerging infectious diseases, and ecosystem health. Unique Features Curriculum Veterinary Public Health • Earn a MPH degree in the same four 42 credits MPH Program Contacts: years as your DVM. Core Curriculum (21.5 credits) • PubH 6299 - Public Health is a Team Sport: The Power www.php.umn.edu • The MPH is offered through a mix of Collaboration (1.5 cr) of online and in-person classes. Online • PubH 6020-Fundanmentals of Social and Behavioral Program Director: courses are taken during summer Science (3 cr) Larissa Minicucci, DVM, MPH terms, before and during your • PubH 6102 - Issues in Environmental and [email protected] veterinary curriculum. Attendance at Occupational Health (2 cr) 612-624-3685 the Public Health Institute, held each • PubH 6320 - Fundamentals of Epidemiology (3 cr) Program Coordinator: summer at the University of • PubH 6414 - Biostatistical Methods (3 cr) Sarah Summerbell, BS Minnesota, provides you with the • PubH 6741 - Ethics in Public Health: Professional [email protected] opportunity to earn elective credits. Practice and Policy (1 cr) 612-626-1948 The Public Health Institute is a unique • PubH 6751 - Principles of Management in Health forum for professionals from multiple Services Organizations (2 cr) disciplines to connect and immerse • PubH 7294 - Master’s Project (3 cr) Cornell Faculty Liaisons: themselves in emerging public health • PubH 7296 - Field Experience (3 cr) Alfonso Torres, DVM, MS, PhD issues. -

Skin Diseases of the Dog and Cat, Third Edition
Skin Diseases of the Dog and Cat THIRD EDITION Skin Diseases of the Dog and Cat THIRD EDITION NICOLE A. HEINRICH, DVM, DACVD McKeever Dermatology Clinics Eden Prairie and Inver Grove Heights Minnesota, USA MELISSA EISENSCHENK, MS, DVM, DACVD Pet Dermatology Clinic Maple Grove Minnesota, USA RICHARD G. HARVEY, BVSc, DVDF, Dip. ECVD, FRSB, PhD, MRCVS The Veterinary Centre Coventry, UK TIM NUTTALL, BSc, BVSc, PhD, CertVD, CBiol, MRSB, MRCVS Head of Dermatology The Royal (Dick) School of Veterinary Studies The University of Edinburgh Roslin, UK CRC Press Taylor & Francis Group 6000 Broken Sound Parkway NW, Suite 300 Boca Raton, FL 33487-2742 © 2019 by Taylor & Francis Group, LLC CRC Press is an imprint of Taylor & Francis Group, an Informa business No claim to original U.S. Government works Printed on acid-free paper International Standard Book Number-13: 978-1-4822-2596-9 (Hardback) International Standard Book Number-13: 978-1-138-30870-1 (Paperback) This book contains information obtained from authentic and highly regarded sources. While all reasonable efforts have been made to publish reliable data and information, neither the author[s] nor the publisher can accept any legal responsibility or liability for any errors or omissions that may be made. The publishers wish to make clear that any views or opinions expressed in this book by individual editors, authors or contributors are personal to them and do not necessarily reflect the views/opinions of the publishers. The information or guidance contained in this book is intended for use by medical, scientific or health-care professionals and is provided strictly as a supplement to the medical or other professional’s own judgement, their knowledge of the patient’s medical history, relevant manufacturer’s instructions and the appropriate best practice guidelines. -

Measles Clinical Guidance: Identification & Testing of Suspect Measles Cases
June 2019 Measles Clinical Guidance: Identification & Testing of Suspect Measles Cases The United States declared measles eliminated in 2000, meaning that there is not endemic transmission within the country and reported cases are due to infection while visiting another country. Measles continues to circulate in much of the world, including Europe, Asia and Africa. International travel, domestic travel through international airports, and contact with international visitors can pose a risk for exposure to measles. When measles is imported into the United States, additional transmission can occur locally. While providers should consider measles in patients with fever and a descending rash, measles is unlikely in the absence of confirmed measles cases in your community or a history of travel or exposure to travelers. This guidance discusses which patients should be prioritized for measles testing. Testing for measles should be based on: A) Measles symptoms: • Fever, including subjective fever. • Rash that starts on the head and descends. • Usually 1 or 2 of the 3 “Cs” – cough, coryza and conjunctivitis. B) Risk factors increasing the likelihood of a measles diagnosis: • In the prior 3 weeks: travel outside of North America, transit through U.S. international airports, or interaction with foreign visitors, including at a U.S. tourist attraction. • Confirmed measles cases in your community. • Never immunized with measles vaccine and born in 1957 or later. NOTE: Fever and rash occur in approximately 5% of MMR vaccine recipients, typically 6-12 days after immunization. Such reactions can be clinically identical to measles infection, and result in positive laboratory testing for measles. This reflects an immune response due to exposure to measles vaccine virus rather than wild measles virus and the patient is not infectious. -
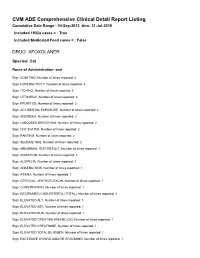
FDA CVM Comprehensive ADE Report Listing for Afoxolaner
CVM ADE Comprehensive Clinical Detail Report Listing Cumulative Date Range : 04-Sep-2013 -thru- 31-Jul-2018 Included 1932a cases = : True Included Medicated Feed cases = : False DRUG: AFOXOLANER Species: Cat Route of Administration: oral Sign: VOMITING, Number of times reported: 4 Sign: HYPERACTIVITY, Number of times reported: 3 Sign: ITCHING, Number of times reported: 3 Sign: LETHARGY, Number of times reported: 3 Sign: PRURITUS, Number of times reported: 3 Sign: ACCIDENTAL EXPOSURE, Number of times reported: 2 Sign: ANOREXIA, Number of times reported: 2 Sign: LABOURED BREATHING, Number of times reported: 2 Sign: NOT EATING, Number of times reported: 2 Sign: PANTING, Number of times reported: 2 Sign: SEIZURE NOS, Number of times reported: 2 Sign: ABNORMAL TEST RESULT, Number of times reported: 1 Sign: AGITATION, Number of times reported: 1 Sign: ALOPECIA, Number of times reported: 1 Sign: ANAEMIA NOS, Number of times reported: 1 Sign: ATAXIA, Number of times reported: 1 Sign: CERVICAL VENTROFLEXION, Number of times reported: 1 Sign: CONSTIPATION, Number of times reported: 1 Sign: DECREASED CHOLESTEROL (TOTAL), Number of times reported: 1 Sign: ELEVATED ALT, Number of times reported: 1 Sign: ELEVATED AST, Number of times reported: 1 Sign: ELEVATED BUN, Number of times reported: 1 Sign: ELEVATED CREATINE-KINASE (CK), Number of times reported: 1 Sign: ELEVATED CREATININE, Number of times reported: 1 Sign: ELEVATED TOTAL BILIRUBIN, Number of times reported: 1 Sign: EXCESSIVE LICKING AND/OR GROOMING, Number of times reported: 1 Sign: FEVER,