Clear Cell Acanthoma: a Clinical, Dermatoscopic, and Histological Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

The Tamilnadu Dr. M.G.R. Medical University Chennai, Tamil Nadu
CLINICO-PATHOLOGICAL STUDY OF SKIN SURFACE EPIDERMAL AND APPENDAGEAL TUMOURS Dissertation Submitted in partial fulfillment of university regulations for M.D. DEGREE IN DERMATOLOGY, VENEREOLOGY AND LEPROSY BRANCH XII – A THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, TAMIL NADU SEPTEMBER 2006 CERTIFICATE This is to certify that this Dissertation entitled “CLINICO-PATHOLOGICAL STUDY OF SKIN SURFACE EPIDERMAL AND APPENDAGEAL TUMOURS” is a bonafide work done by DR.G.BALAJI, Postgraduate student of Department of Dermatology, Leprosy and Institute of STD, Madras Medical College and Government General Hospital, Chennai – 3 for the award of Degree of M.D.( Dermatology, Venereology and Leprosy ) Branch XII – A during the academic year of 2003-2006. This work has not previously formed in the basis for the award of any degree or diploma. Prof. Dr. B. Parveen, MD., DD., Professor & Head, Dept. of Dermatology and Leprosy, Madras Medical College & Govt. General Hospital, Chennai – 3. Prof. Dr. Kalavathy Ponniraivan, MD., The Dean Madras Medical College & Govt. General Hospital, Chennai – 3. SPECIAL ACKNOWLEDGEMENT I sincerely thank Prof. Dr. Kalavathy Ponniraivan, MD., Dean, Madras Medical College & Govt. General Hospital, Chennai – 3, for granting me permission to use the resources of this institution for my study. ACKNOWLEDGEMENT I sincerely thank Prof. B.Parveen MD.,DD, Professor and Head of Department of Dermatology for her invaluable guidance and encouragement for the successful completion of this study. I express my heart felt gratitude to Dr.N.Gomathy MD.,DD, former Head of department of Dermatology who was instrumental in the initiation of this project, giving constant guidance throughout my work. -

Expert-Level Diagnosis of Nonpigmented Skin Cancer by Combined Convolutional Neural Networks
Supplementary Online Content Tschandl P, Rosendahl C, Akay BN, et al. Expert-level diagnosis of nonpigmented skin cancer by combined convolutional neural networks. JAMA Dermatol. Published online November 28, 2018. doi:10.1001/jamadermatol.2018.4378 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set eAppendix. Neural Network Training eTable 1. Complete List of Diagnoses and Their Frequencies Within the Test-Set eTable 2. Education of Users According to Their Experience Group eTable 3. Percent of Correct Prediction of the Malignancy Status for Specific Diagnoses of a CNN Using Either Close-up or Dermatoscopic Images This supplementary material has been provided by the authors to give readers additional information about their work. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set A threshold cut at 0.2 (black) is found for a minimum of 51.3% specificity. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eAppendix. Neural Network Training We compared multiple architecture and training hyperparameter combinations in a grid-search fashion, and used only the single best performing network for dermoscopic and close-up images, based on validation accuracy, for further analyses. We trained four different CNN architectures (InceptionResNetV2, InceptionV3, Xception, ResNet50) and used model definitions and ImageNet pretrained weights as available in the Tensorflow (version 1.3.0)/ Keras (version 2.0.8) frameworks. -
A Case of Polypoid Clear Cell Acanthoma on the Nipple
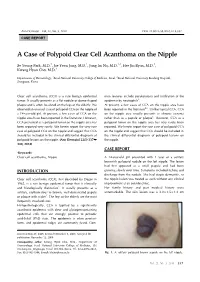
Ann Dermatol Vol. 22, No. 3, 2010 DOI: 10.5021/ad.2010.22.3.337 CASE REPORT A Case of Polypoid Clear Cell Acanthoma on the Nipple Se Young Park, M.D.1, Jae Yoon Jung, M.D.1, Jung Im Na, M.D.1,2, Hee Jin Byun, M.D.1, Kwang Hyun Cho, M.D.1 Departments of Dermatology, 1Seoul National University College of Medicine, Seoul, 2Seoul National University Bundang Hospital, Seongnam, Korea Clear cell acanthoma (CCA) is a rare benign epidermal mon features include parakeratosis and infiltration of the tumor. It usually presents as a flat nodule or dome-shaped epidermis by neutrophils3. plaque and is often localized on the legs of the elderly. We At present, a few cases of CCA on the nipple area have observed an unusual case of polypoid CCA on the nipple of been reported in the literature4-6. Unlike typical CCA, CCA a 14-year-old girl. At present, a few cases of CCA on the on the nipple area usually presents as chronic eczema nipple area have been reported in the literature. However, rather than as a papule or plaque6. However, CCA as a CCA presented as a polypoid tumor on the nipple area has polypoid tumor on the nipple area has very rarely been been reported very rarely. We herein report the very rare reported. We herein report the rare case of polypoid CCA case of polypoid CCA on the nipple and suggest that CCA on the nipple and suggest that CCA should be included in should be included in the clinical differential diagnosis of the clinical differential diagnosis of polypoid lesions on polypoid lesions on the nipple. -

Seborrheic Keratosis
Benign Epidermal and Dermal Tumors REAGAN ANDERSON, DO- PROGRAM DIRECTOR, COLORADO DERMATOLOGY INSTITUTE, RVU PGY3 RESIDENTS- JONATHAN BIELFIELD, GEORGE BRANT PGY2 RESIDENT- MICHELLE ELWAY Seborrheic Keratosis Common benign growth seen after third/fourth decade of life Ubiquitous among older individuals Tan to black, macular, papular, or verrucous lesion Occur everywhere except palms, soles, and mucous membranes Can simulate melanocytic neoplasms Pathogenesis: Sun exposure- Australian study found higher incidence in the head/neck Alteration in distribution of epidermal growth factors Somatic activating mutations in fibroblast growth factor receptor and phosphoinositide-3-kinase Seborrheic Keratosis Sign of Leser-Trelat: Rare cutaneous marker of internal malignancy • Gastric/colonic adenocarcinoma, breast carcinoma, and lymphoma m/c • Abrupt increase in number/size of SKs that can occur before, during, or after an internal malignancy is detected • 40% pruritus • M/C location is the back • Malignant acanthosis nigricans may also appear in 20% of patients • Should resolve when primary tumor is treated, and reappear with recurrence/mets Seborrheic Keratosis 6 Histologic types Acanthotic Hyperkeratotic Reticulated Irritated Clonal Melanoacanthoma Borst-Jadassohn phenomenon Well-demarcated nests of keratinocytes within the epidermis Seborrheic Keratoses Treatment Reassurance Irritated SKs (itching, catching on clothes, inflamed) Cryotherapy, curettage, shave excision Pulsed CO2, erbium:YAG lasers Electrodessication Flegel -

A Deep Learning System for Differential Diagnosis of Skin Diseases
A deep learning system for differential diagnosis of skin diseases 1 1 1 1 1 1,2 † Yuan Liu , Ayush Jain , Clara Eng , David H. Way , Kang Lee , Peggy Bui , Kimberly Kanada , ‡ 1 1 1 Guilherme de Oliveira Marinho , Jessica Gallegos , Sara Gabriele , Vishakha Gupta , Nalini 1,3,§ 1 4 1 1 Singh , Vivek Natarajan , Rainer Hofmann-Wellenhof , Greg S. Corrado , Lily H. Peng , Dale 1 1 † 1, 1, 1, R. Webster , Dennis Ai , Susan Huang , Yun Liu * , R. Carter Dunn * *, David Coz * * Affiliations: 1 G oogle Health, Palo Alto, CA, USA 2 U niversity of California, San Francisco, CA, USA 3 M assachusetts Institute of Technology, Cambridge, MA, USA 4 M edical University of Graz, Graz, Austria † W ork done at Google Health via Advanced Clinical. ‡ W ork done at Google Health via Adecco Staffing. § W ork done at Google Health. *Corresponding author: [email protected] **These authors contributed equally to this work. Abstract Skin and subcutaneous conditions affect an estimated 1.9 billion people at any given time and remain the fourth leading cause of non-fatal disease burden worldwide. Access to dermatology care is limited due to a shortage of dermatologists, causing long wait times and leading patients to seek dermatologic care from general practitioners. However, the diagnostic accuracy of general practitioners has been reported to be only 0.24-0.70 (compared to 0.77-0.96 for dermatologists), resulting in over- and under-referrals, delays in care, and errors in diagnosis and treatment. In this paper, we developed a deep learning system (DLS) to provide a differential diagnosis of skin conditions for clinical cases (skin photographs and associated medical histories). -

Inverted Follicular Keratosis
J Clin Pathol: first published as 10.1136/jcp.28.6.465 on 1 June 1975. Downloaded from J. clin. Path., 1975, 28, 465-471 Inverted follicular keratosis J. G. AZZOPARDI AND R. LAURINI From the Department ofHistopathology, Royal Postgraduate Medical School, London SYNOPSIS Attention is drawn to a benign skin tumour which has escaped recognition in the British literature. Inverted follicular keratosis can be mistaken clinically for basal cell carcinoma and a variety of benign skin lesions. Pathologically it is easily confused with squamous carcinoma, a serious error because this lesion occurs dominantly on the face. The lesion is thought to arise from the infundibulum of the hair follicle. The purpose of this paper is to draw attention to a in consultation. Haemalum eosin sections were lesion which has been described in the dermatological studied in all cases. In the eight cases from our own and ophthalmic literature but which is little known material, Best carmine, Masson-Fontana, Alcian to general pathologists. Helwig (1954) gave it the green, and periodic acid Schiff stains were also name 'inverted follicular keratosis' and described studied. Step sections were examined in these eight its essential characteristics. This descripion is, cases. however, unavailable to most pathologists. Boniuk copyright. and Zimmerman (1963) reported on lesions of this CLINICAL DATA type on the eyelids. We have not been able to find All lesions were single, though one patient had a any reference to it in the British literature. basal cell carcinoma at another site in addition. As can be seen from the table, eight lesions were Materials and Methods situated on the face and one on the chest wall. -

Reportable Skin Cancers
11/18/2014 Reportable Skin Cancers 2014/2015 FCDS Educational Webcast Series November 20, 2014 Steven Peace, CTR Anatomy and Physiology of the Integumentary System WHO Classification of Neoplasms of the Skin Signs & Symptoms, Prognostic Factors and Tumor Markers CSv02.05 and SSFs, AJCC TNM 7thed, SS2000 Plus…NCCN Treatment Guidelines The Florida Cancer Data System sincerely thanks the Florida Department of Health, the Centers for Disease Control and Prevention National Program of Cancer Registries, and the University of Miami Miller School of Medicine for their support. 2 1 11/18/2014 Anatomy and Physiology of the Integumentary System Skin or Not Skin - Genital and Non-Genital “Skin” Sites Skin Cancer Facts and Figures Risk Factors – Signs and Symptoms Types of Skin Cancers Overview of Melanoma of Skin Staging Criteria for Melanoma of Skin Overview of Merkel Cell Carcinoma of Skin Staging Criteria for Merkel Cell Carcinoma of Skin Overview of Other Reportable Skin Neoplasms Staging Criteria for Other Reportable Skin Neoplasms 3 Source: http://www.healthandbeautyace.com 4 2 11/18/2014 Defensive Barrier protection from sun protection from injury protection from pathogens protection from environment Thermoregulation controls blood flow regulates evaporation controls release of sweat Vitamin D Production Absorption and Secretion Maintain Body Fluids Balance Excrete Waste Products in Sweat Synthesis of Epidermal Lipids (fats and oils) Sensory Perception and Sensation Touch/Feel/Hot/Cold/Pressure/Vibration/Wind 5 -

Skin Cancer Screening in Primary Care Using Dermoscopy
SKIN CANCER SCREENING IN PRIMARY CARE USING DERMOSCOPY A Dissertation Submitted to the Graduate Faculty of the North Dakota State University of Agriculture and Applied Science By Erin Eliza Lubitz In Partial Fulfillment of the Requirements for the Degree of DOCTOR OF NURSING PRACTICE Major Program: Nursing March 2020 Fargo, North Dakota North Dakota State University Graduate School Title SKIN CANCER SCREENING IN PRIMARY CARE USING DERMOSCOPY By Erin Eliza Lubitz The Supervisory Committee certifies that this disquisition complies with North Dakota State University’s regulations and meets the accepted standards for the degree of DOCTOR OF NURSING PRACTICE SUPERVISORY COMMITTEE: Dean Gross, PhD, FNP-BC Chair Kelly Buettner-Schmidt, PhD, RN, FAAN Nicole German, PhD Anna Thomas, DNP, APRN-C Approved: 04/06/2020 Carla Gross, PhD Date Department Chair ABSTRACT Skin cancer rates continue to rise affecting millions of individuals annually. While cutaneous malignant melanoma comprises a fraction of total skin cancers diagnosed, melanoma is associated with a poor prognosis and higher mortality rate when compared to other forms of skin cancer. The greatest risk factor for skin cancer is the amount of ultraviolet light exposure making skin cancer the most common preventable form of cancer. In conjunction with primary prevention, part of secondary prevention measures involves performing routine skin examinations. According to data from the National Health Interview Survey, only 8% of individuals who had seen a primary care provider in the previous 12 months had a skin examination performed (Johnson et al., 2017). A low rate of skin examination can largely be attributed to current professional guidelines from the United States Preventative Services Task Force (2016) not supporting routine skin screening of all patients. -

Keratoacanthoma As a Postoperative Complication of Skin Cancer Excision
DERMATOLOGIC SURGERY Keratoacanthoma as a postoperative complication of skin cancer excision Leonard H. Goldberg, MD, FRCP,a,b Sirunya Silapunt, MD,a Kathleen K. Beyrau, MD,c S. Ray Peterson, MD,a Paul M. Friedman, MD,a and Murad Alam, MDd Houston, Texas, Portage, Wisconsin; and Chicago, Illinois Background: Keratoacanthomas usually occur spontaneously as a single rapidly growing tumor on sun-exposed skin. Multiple keratoacanthomas are rarely seen. Keratoacanthomas may also develop after trauma, laser resurfacing, radiation therapy, and at the donor site after skin grafting. Objective: We report 6 cases of keratoacanthomas that developed in and around healing and healed surgical sites after treatment of skin cancer. These tumors developed 1 to 3 months after surgery and were sometimes multiple. Methods: We performed follow-up examinations of patients’ wounds after the treatment of skin cancer. Histological examination of nodules developing in the margins of healing wound sites and in the scars of healed wound sites after Mohs micrographic surgery revealed keratoacanthomas. Results: The tumors presented as a rapidly growing nodule or nodules, with the typical morphology and pathology of keratoacanthoma. One patient developed multiple keratoacanthomas at surgical and nonsur- gical sites. These nodules were treated by a combination of excision, curettage and electrodesiccation, and oral isotretinoin, 4 mg/d. Conclusion: Keratoacanthoma must be considered in the differential diagnosis of a rapidly growing nodule within or around the surgical site after skin cancer surgery. (J Am Acad Dermatol 2004;50:753-8.) eratoacanthoma (KA) usually occurs spon- of KA that developed in wounds healing by second taneously as a single rapidly growing tumor intention and in scars within 3 months after Mohs K with characteristic morphology on the sun- micrographic surgery (MMS) for squamous cell car- exposed regions of middle-aged or older persons. -
ASCP. Cutaneous Adnexal Neoplasms: Classification and A
1355 Cutaneous Adnexal Neoplasms: Classification And A Practical Diagnostic Approach David S. Cassarino, MD, PhD, FASCP WEEKEND OF PATHOLOGY AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W Monroe Ste 1600 Chicago, IL 60603 Program Content and Disclosure The primary purpose of this activity is educational and the comments, opinions, and/or recommendations expressed by the faculty or authors are their own and not those of the ASCP. There may be, on occasion, changes in faculty and program content. In order to ensure balance, independence, objectivity, and scientific rigor in all its educational activities, and in accordance with ACCME Standards, the ASCP requires all individuals in positions to influence and/or control the content of ASCP CME activities to disclose whether they do or do not have any relevant financial relationships with proprietary entities producing health care goods or services that are discussed in the CME activities, with the exemption of non-profit or government organizations and non-health care related companies. These relationships are reviewed and any identified conflicts of interest are resolved prior to the activity. Faculty are asked to use generic names in any discussion of therapeutic options, to base patient care recommendations on scientific evidence, and to base information regarding commercial products/services on scientific methods generally accepted by the medical community. All ASCP CME activities are evaluated by participants for the presence of any commercial bias and this input is utilized for subsequent CME planning decisions. The individuals below have responded that they have no relevant financial relationships with commercial interests to disclose: Course Faculty: David S. -

Clear Cell Acanthoma: a Clinical, Dermoscopic and Histological Review
Clear Cell Acanthoma: A Clinical, Dermoscopic and Histological Review John Howard, DO,* Andrei Gherghina, DO, MS,** Jacquiline Habashy, DO, MS,*** Angela Poulos Combs, DO, FAOCD, FAAD,**** Stanley Skopit, DO, MSE, FAOCD, FAAD***** *Dermatology Research Fellow, Larkin Community Hospital, Miami FL **Dermoscopy Fellow, Skin and Cancer Associates, Plantation, FL ***Traditional Rotating Intern, PGY1, Larkin Community Hospital, Miami, FL ****Dermatopathologist, Global Pathology/Aurora Diagnostics, Miami Lakes, FL *****Program Director, Larkin Community Hospital/NSU-COM Dermatology Residency, South Miami, FL Disclosures: None Correspondence: Jacquiline Habashy, DO; [email protected] Abstract Clear cell acanthoma (CCA) is an uncommon, benign epidermal tumor that may be easily misdiagnosed on a clinical basis alone. Although biopsy is commonly performed for diagnosis, perceptive clinicians may suspect a CCA with the use of clinical and dermoscopic findings. We present a case of a suspected clear cell acanthoma confirmed by biopsy along with a clinical, dermoscopic and histological review of the condition. Introduction arranged in a linear “string of pearls” distribution, of lesions can range from approximately 3 mm to CCA was first described in 1962 and was also revealing the characteristic dermoscopic vascular 20 mm, and they can slowly grow for up to 10 years. pattern seen in clear cell acanthoma (CCA) When closely examining the surface of the lesion, known as “Degos acanthoma” and “acanthome 3,4 cellules claires of Degos and Civatte.”1 There are (Figure 2). vascular puncta are present, which easily bleed currently no known risk factors, and the etiology is following minor trauma. These lesions are usually unknown. It is theorized that the cause may be an Discussion found on the lower extremities in middle-aged to CCA is a rare, benign lesion that is oftentimes elderly adults, with both sexes affected equally.5,6 inflammatory reaction secondary to an unknown difficult to diagnose with clinical observation alone.