Loss-Of-Function Mutations in CARD14 Are Associated with a Severe Variant of Atopic Dermatitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
An Integrated Analysis of Public Genomic Data Unveils a Possible
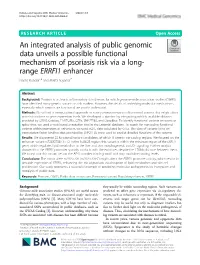
Kubota and Suyama BMC Medical Genomics (2020) 13:8 https://doi.org/10.1186/s12920-020-0662-9 RESEARCH ARTICLE Open Access An integrated analysis of public genomic data unveils a possible functional mechanism of psoriasis risk via a long- range ERRFI1 enhancer Naoto Kubota1,2 and Mikita Suyama1* Abstract Background: Psoriasis is a chronic inflammatory skin disease, for which genome-wide association studies (GWAS) have identified many genetic variants as risk markers. However, the details of underlying molecular mechanisms, especially which variants are functional, are poorly understood. Methods: We utilized a computational approach to survey psoriasis-associated functional variants that might affect protein functions or gene expression levels. We developed a pipeline by integrating publicly available datasets provided by GWAS Catalog, FANTOM5, GTEx, SNP2TFBS, and DeepBlue. To identify functional variants on exons or splice sites, we used a web-based annotation tool in the Ensembl database. To search for noncoding functional variants within promoters or enhancers, we used eQTL data calculated by GTEx. The data of variants lying on transcription factor binding sites provided by SNP2TFBS were used to predict detailed functions of the variants. Results: We discovered 22 functional variant candidates, of which 8 were in noncoding regions. We focused on the enhancer variant rs72635708 (T > C) in the 1p36.23 region; this variant is within the enhancer region of the ERRFI1 gene, which regulates lipid metabolism in the liver and skin morphogenesis via EGF signaling. Further analysis showed that the ERRFI1 promoter spatially contacts with the enhancer, despite the 170 kb distance between them. We found that this variant lies on the AP-1 complex binding motif and may modulate binding levels. -

Defining the Relevant Combinatorial Space of the PKC/CARD-CC Signal Transduction Nodes
bioRxiv preprint doi: https://doi.org/10.1101/228767; this version posted May 2, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. Defining the relevant combinatorial space of the PKC/CARD-CC signal transduction nodes Jens Staal1,2,*, Yasmine Driege1,2, Mira Haegman1,2, Styliani Iliaki1,2, Domien Vanneste1,2, Inna Affonina1,2, Harald Braun1,2, Rudi Beyaert1,2 1 Department of Biomedical Molecular Biology, Ghent University, Ghent, Belgium, 2 VIB-UGent Center for Inflammation Research, Unit of Molecular Signal Transduction in Inflammation, VIB, Ghent, Belgium. * corresponding author: [email protected] Running title: PKC/CARD-CC signaling Abbreviations: Bcl10 = B Cell CLL/Lymphoma 10 CARD = Caspase activation and recruitment domain CC = Coiled-coil domain MALT1 = Mucosa-associated lymphoid tissue lymphoma translocation protein 1 PKC = protein kinase C Keywords: Inflammation, cancer, NF-kappaB, paracaspase Conflict of interests: The authors declare no conflict of interest. bioRxiv preprint doi: https://doi.org/10.1101/228767; this version posted May 2, 2019. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-ND 4.0 International license. Abstract Biological signal transduction typically display a so-called bow-tie or hour glass topology: Multiple receptors lead to multiple cellular responses but the signals all pass through a narrow waist of central signaling nodes. -

Molecular Architecture and Regulation of BCL10-MALT1 Filaments
ARTICLE DOI: 10.1038/s41467-018-06573-8 OPEN Molecular architecture and regulation of BCL10-MALT1 filaments Florian Schlauderer1, Thomas Seeholzer2, Ambroise Desfosses3, Torben Gehring2, Mike Strauss 4, Karl-Peter Hopfner 1, Irina Gutsche3, Daniel Krappmann2 & Katja Lammens1 The CARD11-BCL10-MALT1 (CBM) complex triggers the adaptive immune response in lymphocytes and lymphoma cells. CARD11/CARMA1 acts as a molecular seed inducing 1234567890():,; BCL10 filaments, but the integration of MALT1 and the assembly of a functional CBM complex has remained elusive. Using cryo-EM we solved the helical structure of the BCL10- MALT1 filament. The structural model of the filament core solved at 4.9 Å resolution iden- tified the interface between the N-terminal MALT1 DD and the BCL10 caspase recruitment domain. The C-terminal MALT1 Ig and paracaspase domains protrude from this core to orchestrate binding of mediators and substrates at the filament periphery. Mutagenesis studies support the importance of the identified BCL10-MALT1 interface for CBM complex assembly, MALT1 protease activation and NF-κB signaling in Jurkat and primary CD4 T-cells. Collectively, we present a model for the assembly and architecture of the CBM signaling complex and how it functions as a signaling hub in T-lymphocytes. 1 Gene Center, Ludwig-Maximilians University, Feodor-Lynen-Str. 25, 81377 München, Germany. 2 Research Unit Cellular Signal Integration, Institute of Molecular Toxicology and Pharmacology, Helmholtz-Zentrum München - German Research Center for Environmental Health, Ingolstaedter Landstrasse 1, 85764 Neuherberg, Germany. 3 University Grenoble Alpes, CNRS, CEA, Institut de Biologie Structurale IBS, F-38044 Grenoble, France. 4 Department of Anatomy and Cell Biology, McGill University, Montreal, Canada H3A 0C7. -

UBAC1/KPC2 Regulates TLR3 Signaling in Human Keratinocytes Through Functional Interaction with the CARD14/Carma2sh-TANK Complex
International Journal of Molecular Sciences Article UBAC1/KPC2 Regulates TLR3 Signaling in Human Keratinocytes through Functional Interaction with the CARD14/CARMA2sh-TANK Complex Pellegrino Mazzone 1, Michele Congestrì 2, Ivan Scudiero 1, Immacolata Polvere 2,3, Serena Voccola 3, Lucrezia Zerillo 3, Gianluca Telesio 1, Pasquale Vito 2,3,*, Romania Stilo 2 and Tiziana Zotti 2,3 1 Biogem Consortium, Via Camporeale, 83031 Ariano Irpino (AV), Italy; [email protected] (P.M.); [email protected] (I.S.); [email protected] (G.T.) 2 Dipartimento di Scienze e Tecnologie, Università degli Studi del Sannio, Via Port’Arsa 11, 82100 Benevento, Italy; [email protected] (M.C.); [email protected] (I.P.); [email protected] (R.S.); [email protected] (T.Z.) 3 Genus Biotech, Università degli Studi del Sannio, Via Appia snc, 82030 Apollosa (BN), Italy; [email protected] (S.V.); [email protected] (L.Z.) * Correspondence: [email protected]; Tel.: +39-0824305105 Received: 8 November 2020; Accepted: 8 December 2020; Published: 9 December 2020 Abstract: CARD14/CARMA2 is a scaffold molecule whose genetic alterations are linked to human inherited inflammatory skin disorders. However, the mechanisms through which CARD14/CARMA2 controls innate immune response and chronic inflammation are not well understood. By means of a yeast two-hybrid screening, we identified the UBA Domain Containing 1 (UBAC1), the non-catalytic subunit of the E3 ubiquitin-protein ligase KPC complex, as an interactor of CARMA2sh, the CARD14/CARMA2 isoform mainly expressed in human keratinocytes. UBAC1 participates in the CARMA2sh/TANK complex and promotes K63-linked ubiquitination of TANK. -
A Chromosome-Centric Human Proteome Project (C-HPP) To
computational proteomics Laboratory for Computational Proteomics www.FenyoLab.org E-mail: [email protected] Facebook: NYUMC Computational Proteomics Laboratory Twitter: @CompProteomics Perspective pubs.acs.org/jpr A Chromosome-centric Human Proteome Project (C-HPP) to Characterize the Sets of Proteins Encoded in Chromosome 17 † ‡ § ∥ ‡ ⊥ Suli Liu, Hogune Im, Amos Bairoch, Massimo Cristofanilli, Rui Chen, Eric W. Deutsch, # ¶ △ ● § † Stephen Dalton, David Fenyo, Susan Fanayan,$ Chris Gates, , Pascale Gaudet, Marina Hincapie, ○ ■ △ ⬡ ‡ ⊥ ⬢ Samir Hanash, Hoguen Kim, Seul-Ki Jeong, Emma Lundberg, George Mias, Rajasree Menon, , ∥ □ △ # ⬡ ▲ † Zhaomei Mu, Edouard Nice, Young-Ki Paik, , Mathias Uhlen, Lance Wells, Shiaw-Lin Wu, † † † ‡ ⊥ ⬢ ⬡ Fangfei Yan, Fan Zhang, Yue Zhang, Michael Snyder, Gilbert S. Omenn, , Ronald C. Beavis, † # and William S. Hancock*, ,$, † Barnett Institute and Department of Chemistry and Chemical Biology, Northeastern University, Boston, Massachusetts 02115, United States ‡ Stanford University, Palo Alto, California, United States § Swiss Institute of Bioinformatics (SIB) and University of Geneva, Geneva, Switzerland ∥ Fox Chase Cancer Center, Philadelphia, Pennsylvania, United States ⊥ Institute for System Biology, Seattle, Washington, United States ¶ School of Medicine, New York University, New York, United States $Department of Chemistry and Biomolecular Sciences, Macquarie University, Sydney, NSW, Australia ○ MD Anderson Cancer Center, Houston, Texas, United States ■ Yonsei University College of Medicine, Yonsei University, -

RNA-Seq Identifies a Diminished Differentiation Gene Signature in Primary Monolayer Keratinocytes Grown from Lesional and Uninvo
www.nature.com/scientificreports OPEN RNA-seq identifes a diminished diferentiation gene signature in primary monolayer keratinocytes Received: 27 September 2017 Accepted: 11 December 2017 grown from lesional and uninvolved Published: xx xx xxxx psoriatic skin William R. Swindell 1,2, Mrinal K. Sarkar2, Yun Liang2, Xianying Xing2, Jaymie Baliwag2, James T. Elder2, Andrew Johnston2, Nicole L. Ward3,4 & Johann E. Gudjonsson2 Keratinocyte (KC) hyper-proliferation and epidermal thickening are characteristic features of psoriasis lesions, but the specifc contributions of KCs to plaque formation are not fully understood. This study used RNA-seq to investigate the transcriptome of primary monolayer KC cultures grown from lesional (PP) and non-lesional (PN) biopsies of psoriasis patients and control subjects (NN). Whole skin biopsies from the same subjects were evaluated concurrently. RNA-seq analysis of whole skin identifed a larger number of psoriasis-increased diferentially expressed genes (DEGs), but analysis of KC cultures identifed more PP- and PN-decreased DEGs. These latter DEG sets overlapped more strongly with genes near loci identifed by psoriasis genome-wide association studies and were enriched for genes associated with epidermal diferentiation. Consistent with this, the frequency of AP-1 motifs was elevated in regions upstream of PN-KC-decreased DEGs. A subset of these genes belonged to the same co-expression module, mapped to the epidermal diferentiation complex, and exhibited diferentiation- dependent expression. These fndings demonstrate a decreased diferentiation gene signature in PP/PN-KCs that had not been identifed by pre-genomic studies of patient-derived monolayers. This may refect intrinsic defects limiting psoriatic KC diferentiation capacity, which may contribute to compromised barrier function in normal-appearing uninvolved psoriatic skin. -

Identification of 15 New Psoriasis Susceptibility Loci Highlights the Role of Innate Immunity
LETTERS Identification of 15 new psoriasis susceptibility loci highlights the role of innate immunity To gain further insight into the genetic architecture of psoriasis, We combined three existing GWAS data sets (referred to as Kiel3, we conducted a meta-analysis of 3 genome-wide association the Collaborative Association Study of Psoriasis (CASP)4 and the studies (GWAS) and 2 independent data sets genotyped on Wellcome Trust Case Control Consortium 2 (WTCCC2)5) with two the Immunochip, including 10,588 cases and 22,806 controls. independent case-control data sets of individuals of European descent We identified 15 new susceptibility loci, increasing to 36 the genotyped on the Immunochip: the Psoriasis Association Genetics number associated with psoriasis in European individuals. We Extension (PAGE: 3,580 cases and 5,902 controls) and the Genetic also identified, using conditional analyses, five independent Analysis of Psoriasis Consortium (GAPC: 2,997 cases and 9,183 con- signals within previously known loci. The newly identified loci trols) (data sets are described in Supplementary Tables 1 and 2). shared with other autoimmune diseases include candidate After quality control, the combined data set consisted of 10,588 indivi- genes with roles in regulating T-cell function (such as RUNX3, duals with psoriasis and 22,806 healthy controls. For each GWAS, we TAGAP and STAT3). Notably, they included candidate genes increased the SNP density through imputation, using European haplo- whose products are involved in innate host defense, including type sequences generated by the 1000 Genomes Project (20100804 interferon-mediated antiviral responses (DDX58), macrophage release) as templates. Overall, our analysis included 111,236 SNPs activation (ZC3H12C) and nuclear factor (NF)-kB signaling that were genotyped in both Immunochip data sets that also had good (CARD14 and CARM1). -

CARD10 in a Family with Progressive Immunodeficiency and Autoimmunity
www.nature.com/cmi Cellular & Molecular Immunology CORRESPONDENCE Mutant CARD10 in a family with progressive immunodeficiency and autoimmunity Dan-hui Yang1,2,3, Ting Guo1,2,3, Zhuang-zhuang Yuan4, Cheng Lei1,2,3, Shui-zi Ding1,2,3, Yi-feng Yang5, Zhi-ping Tan5 and Hong Luo1,2,3 Cellular & Molecular Immunology (2020) 17:782–784; https://doi.org/10.1038/s41423-020-0423-x Autoimmunity and immunodeficiency were previously considered (Fig. 1g). Reconstitution studies demonstrated decreased expres- to be mutually exclusive conditions. However, an increased sion of CARD10 mRNA and CARD10 protein in the patient with the understanding of the complex immune regulatory systems and R420C mutation (Fig. S1). signaling mechanisms, coupled with the application of genetic Our study suggests that the R420C mutation is associated with analysis, has demonstrated the complex relationships between recurrent infections, CD, allergic diseases, and other disorders in the two kinds of diseases.1 In recent years, several mild forms of patients. We found that both affected siblings suffered from primary immunodeficiencies have been discovered, presenting asthma, while their blood eosinophils were low. This phenomenon with opportunistic infections overlapping autoimmunity and/or is consistent with the features seen in Card10-deficient mice. In allergy late in life.1 the Card10−/− mouse asthma model, airway eosinophils are Caspase recruitment domain (CARD)-containing proteins, decreased but airway hyperresponsiveness is not decreased CARD9, CARD10 (CARMA3), CARD11 (CARMA1), and CARD14 compared with the respective levels in WT mice.8 In the affected 1234567890();,: (CARMA2), are members of the membrane-associated guanylate family member compared with the sibling, we observed that kinase family. -

Caspase Recruitment Domain (CARD) Family (CARD9, CARD10, CARD11, CARD14 and CARD15) Are Increased During Active Inflammation In
Yamamoto-Furusho et al. Journal of Inflammation (2018) 15:13 https://doi.org/10.1186/s12950-018-0189-4 RESEARCH Open Access Caspase recruitment domain (CARD) family (CARD9, CARD10, CARD11, CARD14 and CARD15) are increased during active inflammation in patients with inflammatory bowel disease Jesús K. Yamamoto-Furusho1* , Gabriela Fonseca-Camarillo1†, Janette Furuzawa-Carballeda2†, Andrea Sarmiento-Aguilar1, Rafael Barreto-Zuñiga3, Braulio Martínez-Benitez4 and Montserrat A. Lara-Velazquez5 Abstract Background: The CARD family plays an important role in innate immune response by the activation of NF-κB. The aim of this study was to determine the gene expression and to enumerate the protein-expressing cells of some members of the CARD family (CARD9, CARD10, CARD11, CARD14 and CARD15) in patients with IBD and normal controls without colonic inflammation. Methods: We included 48 UC patients, 10 Crohn’s disease (CD) patients and 18 non-inflamed controls. Gene expression was performed by RT-PCR and protein expression by immunohistochemistry. CARD-expressing cells were assessed by estimating the positively staining cells and reported as the percentage. Results: TheCARD9andCARD10geneexpressionwassignificantlyhigherinUCgroupscomparedwithCD (P<0.001). CARD11 had lower gene expression in UC than in CD patients (P<0.001). CARD14 gene expression was higher in the group with active UC compared to non-inflamed controls (P<0.001). The low expression of CARD14 gene was associated with a benign clinical course of UC, characterized by initial activity followed by long-term remission longer than 5 years (P=0.01, OR = 0.07, 95%CI:0.007–0.70). CARD15 gene expression was lower in UC patients versus CD (P=0.004). -

The Mutational Pattern of Primary Lymphoma of the Central Nervous System Determined by Whole-Exome Sequencing
Leukemia (2015) 29, 677–685 © 2015 Macmillan Publishers Limited All rights reserved 0887-6924/15 www.nature.com/leu ORIGINAL ARTICLE The mutational pattern of primary lymphoma of the central nervous system determined by whole-exome sequencing I Vater1,8, M Montesinos-Rongen2,8, M Schlesner3,8, A Haake1, F Purschke2, R Sprute2, N Mettenmeyer2, I Nazzal2, I Nagel1, J Gutwein1, J Richter1, I Buchhalter3, RB Russell4,5, OD Wiestler6, R Eils3,5,7, M Deckert2,9 and R Siebert1,9 To decipher the mutational pattern of primary CNS lymphoma (PCNSL), we performed whole-exome sequencing to a median coverage of 103 × followed by mutation verification in 9 PCNSL and validation using Sanger sequencing in 22 PCNSL. We identified a median of 202 (range: 139–251) potentially somatic single nucleotide variants (SNV) and 14 small indels (range: 7–22) with potentially protein-changing features per PCNSL. Mutations affected the B-cell receptor, toll-like receptor, and NF-κB and genes involved in chromatin structure and modifications, cell-cycle regulation, and immune recognition. A median of 22.2% (range: 20.0–24.7%) of somatic SNVs in 9 PCNSL overlaps with the RGYW motif targeted by somatic hypermutation (SHM); a median of 7.9% (range: 6.2–12.6%) affects its hotspot position suggesting a major impact of SHM on PCNSL pathogenesis. In addition to the well-known targets of aberrant SHM (aSHM) (PIM1), our data suggest new targets of aSHM (KLHL14, OSBPL10, and SUSD2). Among the four most frequently mutated genes was ODZ4 showing protein-changing mutations in 4/9 PCNSL. -

Table S1. 103 Ferroptosis-Related Genes Retrieved from the Genecards
Table S1. 103 ferroptosis-related genes retrieved from the GeneCards. Gene Symbol Description Category GPX4 Glutathione Peroxidase 4 Protein Coding AIFM2 Apoptosis Inducing Factor Mitochondria Associated 2 Protein Coding TP53 Tumor Protein P53 Protein Coding ACSL4 Acyl-CoA Synthetase Long Chain Family Member 4 Protein Coding SLC7A11 Solute Carrier Family 7 Member 11 Protein Coding VDAC2 Voltage Dependent Anion Channel 2 Protein Coding VDAC3 Voltage Dependent Anion Channel 3 Protein Coding ATG5 Autophagy Related 5 Protein Coding ATG7 Autophagy Related 7 Protein Coding NCOA4 Nuclear Receptor Coactivator 4 Protein Coding HMOX1 Heme Oxygenase 1 Protein Coding SLC3A2 Solute Carrier Family 3 Member 2 Protein Coding ALOX15 Arachidonate 15-Lipoxygenase Protein Coding BECN1 Beclin 1 Protein Coding PRKAA1 Protein Kinase AMP-Activated Catalytic Subunit Alpha 1 Protein Coding SAT1 Spermidine/Spermine N1-Acetyltransferase 1 Protein Coding NF2 Neurofibromin 2 Protein Coding YAP1 Yes1 Associated Transcriptional Regulator Protein Coding FTH1 Ferritin Heavy Chain 1 Protein Coding TF Transferrin Protein Coding TFRC Transferrin Receptor Protein Coding FTL Ferritin Light Chain Protein Coding CYBB Cytochrome B-245 Beta Chain Protein Coding GSS Glutathione Synthetase Protein Coding CP Ceruloplasmin Protein Coding PRNP Prion Protein Protein Coding SLC11A2 Solute Carrier Family 11 Member 2 Protein Coding SLC40A1 Solute Carrier Family 40 Member 1 Protein Coding STEAP3 STEAP3 Metalloreductase Protein Coding ACSL1 Acyl-CoA Synthetase Long Chain Family Member 1 Protein -
Essential Role of CARD14 in Murine Experimental Psoriasis
Essential Role of CARD14 in Murine Experimental Psoriasis Mayuri Tanaka, Kouji Kobiyama, Tetsuya Honda, Kozue Uchio-Yamada, Yayoi Natsume-Kitatani, Kenji Mizuguchi, This information is current as Kenji Kabashima and Ken J. Ishii of September 28, 2021. J Immunol published online 17 November 2017 http://www.jimmunol.org/content/early/2017/11/17/jimmun ol.1700995 Downloaded from Supplementary http://www.jimmunol.org/content/suppl/2017/11/17/jimmunol.170099 Material 5.DCSupplemental http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 28, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2017 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Published November 17, 2017, doi:10.4049/jimmunol.1700995 The Journal of Immunology Essential Role of CARD14 in Murine Experimental Psoriasis Mayuri Tanaka,*,† Kouji Kobiyama,*,†,1 Tetsuya Honda,‡ Kozue Uchio-Yamada,x Yayoi Natsume-Kitatani,{ Kenji Mizuguchi,{ Kenji Kabashima,‡ and Ken J. Ishii*,† Caspase recruitment domain family member 14 (CARD14) was recently identified as a psoriasis-susceptibility gene, but its immunological role in the pathogenesis of psoriasis in vivo remains unclear.