Process of Respiration, the Relationship of Air to Diseases of the the Impact on Air Quality of Human Activities and the Effect
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Is Colonic Propionate Delivery a Novel Solution to Improve Metabolism and Inflammation in Overweight Or Obese Subjects?
Commentary in IgG levels in IPE-treated subjects versus Is colonic propionate delivery a novel those receiving cellulose supplementa- tion. This interesting discovery is the Gut: first published as 10.1136/gutjnl-2019-318776 on 26 April 2019. Downloaded from solution to improve metabolism and first evidence in humans that promoting the delivery of propionate in the colon inflammation in overweight or may affect adaptive immunity. It is worth noting that previous preclinical and clin- obese subjects? ical data have shown that supplementation with inulin-type fructans was associated 1,2 with a lower inflammatory tone and a Patrice D Cani reinforcement of the gut barrier.7 8 Never- theless, it remains unknown if these effects Increased intake of dietary fibre has been was the lack of evidence that the observed are directly linked with the production of linked to beneficial impacts on health for effects were due to the presence of inulin propionate, changes in the proportion of decades. Strikingly, the exact mechanisms itself on IPE or the delivery of propionate the overall levels of SCFAs, or the pres- of action are not yet fully understood. into the colon. ence of any other bacterial metabolites. Among the different families of fibres, In GUT, Chambers and colleagues Alongside the changes in the levels prebiotics have gained attention mainly addressed this gap of knowledge and of SCFAs, plasma metabolome analysis because of their capacity to selectively expanded on their previous findings.6 For revealed that each of the supplementa- modulate the gut microbiota composition 42 days, they investigated the impact of tion periods was correlated with different 1 and promote health benefits. -

Occupational Airborne Particulates
Environmental Burden of Disease Series, No. 7 Occupational airborne particulates Assessing the environmental burden of disease at national and local levels Tim Driscoll Kyle Steenland Deborah Imel Nelson James Leigh Series Editors Annette Prüss-Üstün, Diarmid Campbell-Lendrum, Carlos Corvalán, Alistair Woodward World Health Organization Protection of the Human Environment Geneva 2004 WHO Library Cataloguing-in-Publication Data Occupational airborne particulates : assessing the environmental burden of disease at national and local levels / Tim Driscoll … [et al.]. (Environmental burden of disease series / series editors: Annette Prüss-Ustun ... [et al.] ; no. 7) 1.Dust - adverse effects 2.Occupational exposure 3.Asthma - chemically induced 4.Pulmonary disease, Chronic obstructive - chemically induced 5.Pneumoconiosis - etiology 6.Cost of illness 7.Epidemiologic studies 8.Risk assessment - methods 9.Manuals I.Driscoll, Tim. II.Prüss-Üstün, Annette. III.Series. ISBN 92 4 159186 2 (NLM classification: WA 450) ISSN 1728-1652 Suggested Citation Tim Driscoll, et al. Occupational airborne particulates: assessing the environmental burden of disease at national and local levels. Geneva, World Health Organization, 2004. (Environmental Burden of Disease Series, No. 7). © World Health Organization 2004 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). -

The Lower Critical Solution Temperature (LCST) Transition
Copyright by David Samuel Simmons 2009 The Dissertation Committee for David Samuel Simmons certifies that this is the approved version of the following dissertation: Phase and Conformational Behavior of LCST-Driven Stimuli Responsive Polymers Committee: ______________________________ Isaac Sanchez, Supervisor ______________________________ Nicholas Peppas ______________________________ Krishnendu Roy ______________________________ Venkat Ganesan ______________________________ Thomas Truskett Phase and Conformational Behavior of LCST-Driven Stimuli Responsive Polymers by David Samuel Simmons, B.S. Dissertation Presented to the Faculty of the Graduate School of The University of Texas at Austin in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy The University of Texas at Austin December, 2009 To my grandfather, who made me an engineer before I knew the word and to my wife, Carey, for being my partner on my good days and bad. Acknowledgements I am extraordinarily fortunate in the support I have received on the path to this accomplishment. My adviser, Dr. Isaac Sanchez, has made this publication possible with his advice, support, and willingness to field my ideas at random times in the afternoon; he has my deep appreciation for his outstanding guidance. My thanks also go to the members of my Ph.D. committee for their valuable feedback in improving my research and exploring new directions. I am likewise grateful to the other members of Dr. Sanchez’ research group – Xiaoyan Wang, Yingying Jiang, Xiaochu Wang, and Frank Willmore – who have shared their ideas and provided valuable sounding boards for my mine. I would particularly like to express appreciation for Frank’s donation of his own post-graduation time in assisting my research. -
Exercise and Cellular Respiration Lab
California State University of Bakersfield, Department of Chemistry Exercise and Cellular Respiration Lab Standards: MS-LS1-7 Develop a model to describe how food is rearranged through chemical reactions forming new molecules that support growth and/or release energy as this matter moves through an organism. Introduction: I. Background Information. Cellular respiration (see chemical reaction below) is a chemical reaction that occurs in your cells to create energy; when you are exercising your muscle cells are creating ATP to contract. Cellular respiration requires oxygen (which is breathed in) and creates carbon dioxide (which is breathed out). This lab will address how exercise (increased muscle activity) affects the rate of cellular respiration. You will measure 3 different indicators of cellular respiration: breathing rate, heart rate, and carbon dioxide production. You will measure these indicators at rest (with no exercise) and after 1 and 2 minutes of exercise. Breathing rate is measured in breaths per minute, heart rate in beats per minute, and carbon dioxide in the time it takes bromothymol blue to change color. Carbon dioxide production can be measured by breathing through a straw into a solution of bromothymol blue (BTB). BTB is an acid indicator; when it reacts with acid it turns from blue to yellow. When carbon dioxide reacts with water, a weak acid (carbonic acid) is formed (see chemical reaction below). The more carbon dioxide you breathe into the BTB solution, the faster it will change color to yellow. The purpose of this lab activity is to analyze the effect of exercise on cellular respiration. Background: I. -

Pneumoconiosis
Prim Care Respir J 2013; 22(2): 249-252 PERSPECTIVE Pneumoconiosis *Paul Cullinan1, Peter Reid2 1 Consultant Physician, Royal Brompton and Harefield NHS Foundation Trust, London, UK 2 Consultant Physician, Western General Hospital, Edinburgh, UK Introduction Figure 1. Asbestosis; the HRCT scan shows the typical The pneumoconioses are parenchymal lung diseases that arise from picture of subpleural fibrosis (solid arrow); in addition inhalation of (usually) inorganic dusts at work. Some such dusts are there is diffuse, left-sided pleural thickening (broken biologically inert but visible on a chest X-ray or CT scan; thus, while arrow), characteristic too of heavy asbestos exposure they are radiologically alarming they do not give rise to either clinical disease or deficits in pulmonary function. Others – notably asbestos and crystalline silica – are fibrogenic so that the damage they cause is through the fibrosis induced by the inhaled dust rather than the dust itself. Classically these give rise to characteristic radiological patterns and restrictive deficits in lung function with reductions in diffusion capacity; importantly, they may progress long after exposure to the causative mineral has finished. In the UK and similar countries asbestosis is the commonest form of pneumoconiosis but in less developed parts of the world asbestosis is less frequent than silicosis; these two types are discussed in detail below. Other, rarer types of pneumoconiosis include stannosis (from tin fume), siderosis (iron), berylliosis (beryllium), hard metal disease (cobalt) and coal worker’s pneumoconiosis. Asbestosis Clinical scenario How is the diagnosis made? Asbestosis is the ‘pneumoconiosis’ that arises from exposure to A man of 78 reports gradually worsening breathlessness; he has asbestos in the workplace.1 The diagnosis is made when, on the no relevant medical history of note and has never been a regular background of heavy occupational exposure to any type of asbestos, smoker. -
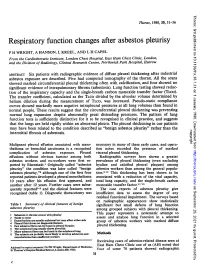
Respiratory Function Changes After Asbestos Pleurisy
Thorax: first published as 10.1136/thx.35.1.31 on 1 January 1980. Downloaded from Thorax, 1980, 35, 31-36 Respiratory function changes after asbestos pleurisy P H WRIGHT, A HANSON, L KREEL, AND L H CAPEL From the Cardiothoracic Institute, London Chest Hospital, East Ham Chest Clinic, London, and the Division of Radiology, Clinical Research Centre, Northwick Park Hospital, Harrow ABSTRACT Six patients with radiographic evidence of diffuse pleural thickening after industrial asbestos exposure are described. Five had computed tomography of the thorax. All the scans showed marked circumferential pleural thickening often with calcification, and four showed no significant evidence of intrapulmonary fibrosis (asbestosis). Lung function testing showed reduc- tion of the inspiratory capacity and the single-breath carbon monoxide transfer factor (TLco). The transfer coefficient, calculated as the TLCO divided by the alveolar volume determined by helium dilution during the measurement of TLco, was increased. Pseudo-static compliance curves showed markedly more negative intrapleural pressures at all lung volumes than found in normal people. These results suggest that the circumferential pleural thickening was preventing normal lung expansion despite abnormally great distending pressures. The pattern of lung function tests is sufficiently distinctive for it to be recognised in clinical practice, and suggests that the lungs are held rigidly within an abnormal pleura. The pleural thickening in our patients may have been related to the condition described as "benign asbestos pleurisy" rather than the copyright. interstitial fibrosis of asbestosis. Malignant pleural effusion associated with meso- necessary in many of these early cases, and opera- thelioma or bronchial carcinoma is a recognised tion notes recorded the presence of marked http://thorax.bmj.com/ complication of asbestos exposure. -

London's Swine Flu Pandemic
Central and North West London NHS Foundation Trust Executive Office Tel: 020 3214 5760 Fax: 020 3214 5761 4 February 2010 Sarah Hurcombe Assistant Scrutiny Manager Post Point 10 City Hall The Queen's Walk London SE1 2AA Dear Ms Hurcombe, I am responding to your request for feedback in relation to London's response to Swine Flu. !asked my Director of Nursing Practice, who is our Infection Control lead, to consider the questions you asked and he has provided me with the following comments: 1. Communication was a bit of an issue at first but this improved rapidly in time. I generally found that staff at NHS London were doing their best to advise where they could. Teleconferencing was a big help and saved a lot of travel time. One final point is that there wasn't any panic at any time when it was declared to be a pandemic. 2. At some of the meetings members of NHS London could become rather defensive to constructive comments. They appeared to take these as personal attacks. A more open debate on the challenges we were all facing would have been helpful. I hope that the above comments are useful. We look forward to viewing others views and feedback when published on your web-site. Yours sincerely, Claire Murdoch Chief Executive Trust Headquarters, Greater London House, Hampstead Road, London NWl 7QY Tel: 020 3214 5700 Fax: 020 3214 5701 www.cnwi.nhs.uk Dear Sarah, Further to the letter from James Cleverly, Chair of Health and Public Services Committee, and in answer to the questions posed: The Ealing Hospital NHS Trust has yet to complete its local debrief, but in general we believe we responded well to the challenge. -

Brownie's THIRD LUNG
BrMARINEownie GROUP’s Owner’s Manual Variable Speed Hand Carry Hookah Diving System ADVENTURE IS ALWAYS ON THE LINE! VSHCDC Systems This manual is also available online 3001 NW 25th Avenue, Pompano Beach, FL 33069 USA Ph +1.954.462.5570 Fx +1.954.462.6115 www.BrowniesMarineGroup.com CONGRATULATIONS ON YOUR PURCHASE OF A BROWNIE’S SYSTEM You now have in your possession the finest, most reliable, surface supplied breathing air system available. The operation is designed with your safety and convenience in mind, and by carefully reading this brief manual you can be assured of many hours of trouble-free enjoyment. READ ALL SAFETY RULES AND OPERATING INSTRUCTIONS CONTAINED IN THIS MANUAL AND FOLLOW THEM WITH EACH USE OF THIS PRODUCT. MANUAL SAFETY NOTICES Important instructions concerning the endangerment of personnel, technical safety or operator safety will be specially emphasized in this manual by placing the information in the following types of safety notices. DANGER DANGER INDICATES AN IMMINENTLY HAZARDOUS SITUATION WHICH, IF NOT AVOIDED, WILL RESULT IN DEATH OR SERIOUS INJURY. THIS IS LIMITED TO THE MOST EXTREME SITUATIONS. WARNING WARNING INDICATES A POTENTIALLY HAZARDOUS SITUATION WHICH, IF NOT AVOIDED, COULD RESULT IN DEATH OR INJURY. CAUTION CAUTION INDICATES A POTENTIALLY HAZARDOUS SITUATION WHICH, IF NOT AVOIDED, MAY RESULT IN MINOR OR MODERATE INJURY. IT MAY ALSO BE USED TO ALERT AGAINST UNSAFE PRACTICES. NOTE NOTE ADVISE OF TECHNICAL REQUIREMENTS THAT REQUIRE PARTICULAR ATTENTION BY THE OPERATOR OR THE MAINTENANCE TECHNICIAN FOR PROPER MAINTENANCE AND UTILIZATION OF THE EQUIPMENT. REGISTER YOUR PRODUCT ONLINE Go to www.BrowniesMarineGroup.com to register your product. -

Pathological Aspects of Asbestosis
POSTGRAD. MED. J. (1966), 42, 613. Postgrad Med J: first published as 10.1136/pgmj.42.492.613 on 1 October 1966. Downloaded from PATHOLOGICAL ASPECTS OF ASBESTOSIS D. O'B. HOURIHANE, M.D., M.C.Path., D.C.P.(Lond.), M.R.C.P.I. W. T. E. MCCAUGHEY, M.D., M.C.Path. School ofPathology, Trinity College, Dublin WIDESPREAD recognition of asbestosis dates from the work of Merewether and Price in 1930. They investigated 363 asbestos workers and concluded that there was a pneumoconiosis resulting from asbestos inhalation, that this condition shortened life, and that measures to diminish the atmospheric concentration of asbestos dust would reduce the incidence of the disease. In 1931 asbestosis was accepted as a compensatable disease in Great Britain and steps were taken to reduce the risk in the asbestos industry. 18 years later Wyers (1949) found that the age at death in this disorder had Protected by copyright. increased and that finger-clubbing had become more common. He suggested that these changes were due to a more chronic form of the disease resulting from improved dust control in the industry following the legislation of 1931. Currently however, the number of new cases of asbestosis in Great Britain is increasing, their frequency suggesting an incidence rate of at least five per thousand of those occupation- ally exposed (McVittie, 1965). Though earlier reports indicated that tuberculosis was common in asbestosis (Wyers, 1949; Gloyne, 1951; Bonser, Foulds and Stewart, 1955) it appears to be a rare I 0 n < ,. ' complication at the present time (Buchanan, 1965). -

08-0205: N.M. and DEPARTMENT of the NAVY, PUGET S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) N.M., Appellant ) ) and ) Docket No. 08-205 ) Issued: September 2, 2008 DEPARTMENT OF THE NAVY, PUGET ) SOUND NAVAL SHIPYARD, Bremerton, WA, ) Employer ) __________________________________________ ) Appearances: Oral Argument July 16, 2008 John Eiler Goodwin, Esq., for the appellant No appearance, for the Director DECISION AND ORDER Before: DAVID S. GERSON, Judge COLLEEN DUFFY KIKO, Judge JAMES A. HAYNES, Alternate Judge JURISDICTION On October 30, 2007 appellant filed a timely appeal from a November 17, 2006 decision of the Office of Workers’ Compensation Programs denying his occupational disease claim. Pursuant to 20 C.F.R. §§ 501.2(c) and 501.3, the Board has jurisdiction over the merits of the claim. ISSUE The issue is whether appellant has established that he sustained occupational asthma in the performance of duty due to accepted workplace exposures. On appeal, he, through his attorney, asserts that the Office did not provide Dr. William C. Stewart, the impartial medical examiner, with a complete, accurate statement of accepted facts. FACTUAL HISTORY On December 8, 2004 appellant, then a 57-year-old insulator, filed an occupational disease claim (Form CA-2) asserting that he sustained occupational asthma and increasing shortness of breath due to workplace exposures to fiberglass, silicates, welding smoke, polychlorobenzenes, rubber, dusts, gases, fumes and smoke from “burning out” submarines from 1991 through January -

Affinity of Small-Molecule Solutes to Hydrophobic, Hydrophilic, and Chemically Patterned Interfaces in Aqueous Solution
Affinity of small-molecule solutes to hydrophobic, hydrophilic, and chemically patterned interfaces in aqueous solution Jacob I. Monroea, Sally Jiaoa, R. Justin Davisb, Dennis Robinson Browna, Lynn E. Katzb, and M. Scott Shella,1 aDepartment of Chemical Engineering, University of California, Santa Barbara, CA 93106; and bDepartment of Civil, Architectural and Environmental Engineering, University of Texas at Austin, Austin, TX 78712 Edited by Peter J. Rossky, Rice University, Houston, TX, and approved November 17, 2020 (received for review September 30, 2020) Performance of membranes for water purification is highly influ- However, a molecular understanding that links membrane enced by the interactions of solvated species with membrane surface chemistry to solute affinity and hence membrane func- surfaces, including surface adsorption of solutes upon fouling. tional properties remains incomplete, due in part to the complex Current efforts toward fouling-resistant membranes often pursue interplay among specific interactions (e.g., hydrogen bonds, surface hydrophilization, frequently motivated by macroscopic electrostatics, dispersion) and molecular morphology (e.g., sur- measures of hydrophilicity, because hydrophobicity is thought to face and polymer configurations) that are difficult to disentangle increase solute–surface affinity. While this heuristic has driven di- (11–14). Chemically heterogeneous surfaces are even less un- verse membrane functionalization strategies, here we build on derstood but can affect fouling in complex ways. -

The Hydrophobic Effect Oil and Water Do Not Mix. This Fact Is So Well
The hydrophobic effect Oil and water do not mix. This fact is so well engrained in our ever-day experience that we never ask “why”. Well, today we are going to ask just this question: “why do oil and water not mix?” At the end of the class you will hopefully see that the reason oil and water do not mix is quite distinct from the reason many other substance do not mix. You will also see that the hydrophobic effect is part of a family of processes called “entropy driven ordering” and that the hydrophobic effect has nothing to do with bonds between hydrophobic molecules. This should sound a bit strange to you right now, but I am sure that at the end of the class it will all make sense to you. Why most liquids mix or do not mix (the generic case) What would our physico-chemical intuition tell us about the process of mixing two liquids? Lets think of a simple lattice model for the two solutions. If we call the substances A and B, the energy for mixing should then be the energy of interaction that are made between A and B, minus the energy of interactions that A made with A, and B made with B, plus the entropy of mixing. "Gmixing = "Hmixing # T"Smixing where "Hmixing = 2"Ha#b # "Ha#a # "Hb#b What predictions would this simple model for solutions make for the energetics of mixing? First, mixing should be favored by entropy and therefore the tendency to mix ! should increase with temperature.