| Megaloblastic Anemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Hematological Complications of Alcoholism
The Hematological Complications of Alcoholism HAROLD S. BALLARD, M.D. Alcohol has numerous adverse effects on the various types of blood cells and their functions. For example, heavy alcohol consumption can cause generalized suppression of blood cell production and the production of structurally abnormal blood cell precursors that cannot mature into functional cells. Alcoholics frequently have defective red blood cells that are destroyed prematurely, possibly resulting in anemia. Alcohol also interferes with the production and function of white blood cells, especially those that defend the body against invading bacteria. Consequently, alcoholics frequently suffer from bacterial infections. Finally, alcohol adversely affects the platelets and other components of the blood-clotting system. Heavy alcohol consumption thus may increase the drinker’s risk of suffering a stroke. KEY WORDS: adverse drug effect; AODE (alcohol and other drug effects); blood function; cell growth and differentiation; erythrocytes; leukocytes; platelets; plasma proteins; bone marrow; anemia; blood coagulation; thrombocytopenia; fibrinolysis; macrophage; monocyte; stroke; bacterial disease; literature review eople who abuse alcohol1 are at both direct and indirect. The direct in the number and function of WBC’s risk for numerous alcohol-related consequences of excessive alcohol increases the drinker’s risk of serious Pmedical complications, includ- consumption include toxic effects on infection, and impaired platelet produc- ing those affecting the blood (i.e., the the bone marrow; the blood cell pre- tion and function interfere with blood cursors; and the mature red blood blood cells as well as proteins present clotting, leading to symptoms ranging in the blood plasma) and the bone cells (RBC’s), white blood cells from a simple nosebleed to bleeding in marrow, where the blood cells are (WBC’s), and platelets. -

©Ferrata Storti Foundation
550 scientific correspondence trophoresis. The patients’ mean age was 51.7±20.1 years (range The characteristics of megaloblastic anemia associated 23-89 years). We also randomly selected age-matched subjects with thalassemia with complete enough data to rule out any complicated condi- tions to fit the criteria of the other 3 groups. Group B contained 10 patients with uncomplicated megaloblastic anemia. Group C Combined megaloblastic anemia with thalassemia is easily contained 12 patients with uncomplicated thalassemia minor masked because of the loss of macrocytosis. We performed a without any previous transfusion. Group D contained 11 healthy retrospective study to compare the major parameters in 4 controls without any history of anemia and with normal CBC and groups of subjects in order to show the characteristics of vitamin levels. Mann-Whitney’s U test was used to test the sig- patients with megaloblastic anemia and thalassemia. Group A nificance of each main parameter. comprised 9 patients with megaloblastic anemia and tha- Table 1 shows the various parameters in the 4 groups of sub- lassemia, group B comprised 10 patients with uncomplicated jects. There was no age difference between groups. The MCV in megaloblastic anemia. Group C comprised 12 uncomplicated group A patients with megaloblastic anemia and thalassemia thalassemia trait and group D was formed of 11 healthy con- was not significantly different from that in the normal subjects, trols. The mean corpuscolar volume (MCV) in group A patients but was significantly lower and higher than that in patients with was not significantly different from that in normal subjects, megaloblastic anemia and with thalassemia, respectively. -

Chapter 03- Diseases of the Blood and Certain Disorders Involving The
Chapter 3 Diseases of the blood and blood-forming organs and certain disorders involving the immune mechanism (D50- D89) Excludes2: autoimmune disease (systemic) NOS (M35.9) certain conditions originating in the perinatal period (P00-P96) complications of pregnancy, childbirth and the puerperium (O00-O9A) congenital malformations, deformations and chromosomal abnormalities (Q00-Q99) endocrine, nutritional and metabolic diseases (E00-E88) human immunodeficiency virus [HIV] disease (B20) injury, poisoning and certain other consequences of external causes (S00-T88) neoplasms (C00-D49) symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified (R00-R94) This chapter contains the following blocks: D50-D53 Nutritional anemias D55-D59 Hemolytic anemias D60-D64 Aplastic and other anemias and other bone marrow failure syndromes D65-D69 Coagulation defects, purpura and other hemorrhagic conditions D70-D77 Other disorders of blood and blood-forming organs D78 Intraoperative and postprocedural complications of the spleen D80-D89 Certain disorders involving the immune mechanism Nutritional anemias (D50-D53) D50 Iron deficiency anemia Includes: asiderotic anemia hypochromic anemia D50.0 Iron deficiency anemia secondary to blood loss (chronic) Posthemorrhagic anemia (chronic) Excludes1: acute posthemorrhagic anemia (D62) congenital anemia from fetal blood loss (P61.3) D50.1 Sideropenic dysphagia Kelly-Paterson syndrome Plummer-Vinson syndrome D50.8 Other iron deficiency anemias Iron deficiency anemia due to inadequate dietary -

General Refugee Health Guidelines
GENERAL REFUGEE HEALTH GUIDELINES U.S. Department of Health and Human Services Centers for Disease Control and Prevention National Center for Emerging and Zoonotic Infectious Diseases Division of Global Migration and Quarantine August 6, 2012 Background On average, more than 50,000 refugees relocate to the United States annually. 1 They come from diverse regions of the world and bring with them health risks and diseases common to all refugee populations as well as some that may be unique to specific populations. The purpose of this document is to describe general and optional testing components that do not fall into the specific disease categories of these guidelines. These guidelines are based upon principles of best practices, with references to primary published reports when available. This document differs from others in the guidelines, which recommend screening for specific disorders. The guidelines in this document include testing for abnormalities or clinical conditions that are not specific disorders but are suggestive of underlying disorders. The tests in this document may indicate either acute or chronic disorders and generally indicate the need for further testing and evaluation to identify the condition causing the abnormality. Testing for chronic health conditions is important, since these conditions are common in newly arriving refugees, both children and adults. 2 Since refugee populations are diverse and are predisposed to diseases that may differ from those found in the U.S. population, the differential diagnosis and initial evaluation of abnormalities are discussed to assist the clinician. General and Optional Tests Many disorders may be detected by using general, nonspecific testing modalities. -

Sulfamethoxazole and Trimethoprim (Double Strength) Tablets, USP
Sulfamethoxazole and Trimethoprim (Double Strength) Tablets, USP To reduce the development of drug-resistant bacteria and maintain the effectiveness of sulfamethoxazole and trimethoprim tablets and other antibacterial drugs. Sulfamethoxazole and trimethoprim tablets should be used only to treat or prevent infections that are proven or strongly suspected to be caused by bacteria. DESCRIPTION Sulfamethoxazole and trimethoprim tablets are a synthetic antibacterial combination product. Sulfamethoxazole is N1-(5-methyl-3-isoxazolyl) sulfanilamide. It is almost white, odorless, tasteless compound with a molecular weight of 253.28 and the following structural formula: Trimethoprim is 2,4-diamino-5-(3,4,5-trimethoxybenzyl) pyrimidine. It occurs as a white to light yellow, odorless, bitter compound with a molecular weight of 290.32 and the following structural formula: Reference ID: 4487013 Each tablet, for oral administration, contains 800 mg sulfamethoxazole and 160 mg trimethoprim plus magnesium stearate, pregelatinized starch and sodium starch glycolate. CLINICAL PHARMACOLOGY Sulfamethoxazole and trimethoprim is rapidly absorbed following oral administration. Both sulfamethoxazole and trimethoprim exist in the blood as unbound, protein-bound and metabolized forms; sulfamethoxazole also exists as the conjugated form. The metabolism of sulfamethoxazole occurs predominately by N4-acetylation, although the glucuronide conjugate has been identified. The principal metabolites of trimethoprim are the 1- and 3-oxides and the 3'- and 4'-hydroxy derivatives. The free forms of sulfamethoxazole and trimethoprim are considered to be the therapeutically active forms. Approximately 70% of sulfamethoxazole and 44% of trimethoprim are bound to plasma proteins. The presence of 10 mg percent sulfamethoxazole in plasma decreases the protein binding of trimethoprim by an insignificant degree; trimethoprim does not influence the protein binding of sulfamethoxazole. -
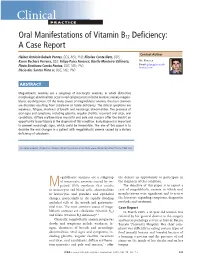
Oral Manifestations of Vitamin B12 Deficiency: a Case Report
Clinical P RACTIC E Oral Manifestations of Vitamin B12 Deficiency: A Case Report Contact Author Hélder Antônio Rebelo Pontes, DDS, MSc, PhD; Nicolau Conte Neto, DDS; Karen Bechara Ferreira, DDS; Felipe Paiva Fonseca; Gizelle Monteiro Vallinoto; Mr. Fonseca Flávia Sirotheau Corrêa Pontes, DDS, MSc, PhD; Email: felipepfonseca@ hotmail.com Décio dos Santos Pinto Jr, DDS, MSc, PhD ABSTRACT Megaloblastic anemias are a subgroup of macrocytic anemias, in which distinctive morphologic abnormalities occur in red cell precursors in bone marrow, namely megalo- blastic erythropoiesis. Of the many causes of megaloblastic anemia, the most common are disorders resulting from cobalamin or folate deficiency. The clinical symptoms are weakness, fatigue, shortness of breath and neurologic abnormalities. The presence of oral signs and symptoms, including glossitis, angular cheilitis, recurrent oral ulcer, oral candidiasis, diffuse erythematous mucositis and pale oral mucosa offer the dentist an opportunity to participate in the diagnosis of this condition. Early diagnosis is important to prevent neurologic signs, which could be irreversible. The aim of this paper is to describe the oral changes in a patient with megaloblastic anemia caused by a dietary deficiency of cobalamin. For citation purposes, the electronic version is the definitive version of this article: www.cda-adc.ca/jcda/vol-75/issue-7/533.html egaloblastic anemias are a subgroup the dentist an opportunity to participate in of macrocytic anemias caused by im- the diagnosis of this condition. Mpaired DNA synthesis that results The objective of this paper is to report a in macrocytic red blood cells, abnormalities case of megaloblastic anemia in which oral in leukocytes and platelets and epithelial manifestations were significant and to review changes, particularly in the rapidly dividing the literature regarding symptoms, diagnostic epithelial cells of the mouth and gastrointes- methods and treatment. -

Severe Megaloblastic Anemia: Vitamin Deficiency and Other Causes
REVIEW CME MOC Daniel S. Socha, MD Sherwin I. DeSouza, MD Aron Flagg, MD Department of Laboratory Medicine, Department of Hematology and Medical Oncology, Department of Pediatric Hematology and Oncology, Robert J. Tomsich Pathology and Laboratory Taussig Cancer Institute, Cleveland Clinic Yale School of Medicine, New Haven, CT Medicine Institute, Cleveland Clinic Mikkael Sekeres, MD, MS Heesun J. Rogers, MD, PhD Department of Hematology and Medical Oncology and Department Department of Laboratory Medicine, Robert J. Tomsich Pathology and of Translational Hematology and Oncology Research, Taussig Laboratory Medicine Institute,Cleveland Clinic; Assistant Professor, Cancer Institute, Cleveland Clinic; Professor, Cleveland Clinic Lerner Cleveland Clinic Lerner College of Medicine of Case Western Reserve College of Medicine of Case Western Reserve, Cleveland, OH University, Cleveland, OH Severe megaloblastic anemia: Vitamin defi ciency and other causes ABSTRACT ot all megaloblastic anemias result N from vitamin defi ciency, but most do. De- Megaloblastic anemia causes macrocytic anemia from termining the underlying cause and initiating ineffective red blood cell production and intramedullary prompt treatment are critical, as prognosis and hemolysis. The most common causes are folate (vitamin management differ among the various condi- B9 ) defi ciency and cobalamin (vitamin B12) defi ciency. tions. Megaloblastic anemia can be diagnosed based on char- This article describes the pathobiology, acteristic morphologic and laboratory fi ndings. However, presentation, evaluation, and treatment of se- other benign and neoplastic diseases need to be con- vere megaloblastic anemia and its 2 most com- sidered, particularly in severe cases. Therapy involves mon causes: folate (vitamin B9) and cobalamin treating the underlying cause—eg, with vitamin supple- (vitamin B12) defi ciency, with 2 representative mentation in cases of defi ciency, or with discontinuation case studies. -

An Exceedingly Rare Presentation of Severe Folate Deficiency-Induced Non-Immune Hemolytic Anemia
Thomas Jefferson University Jefferson Digital Commons Abington Jefferson Health Papers Abington Jefferson Health 6-11-2020 An Exceedingly Rare Presentation of Severe Folate Deficiency- Induced Non-Immune Hemolytic Anemia. Qian Zhang Khine S. Shan Babatunde A. Ogunnaike Atsoufi Amewuame-Kpehor Travis Nace Follow this and additional works at: https://jdc.jefferson.edu/abingtonfp Part of the Internal Medicine Commons Let us know how access to this document benefits ouy This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in Abington Jefferson Health Papers by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Open Access Case Report DOI: 10.7759/cureus.8570 An Exceedingly Rare Presentation of Severe Folate Deficiency-Induced Non-Immune Hemolytic Anemia Qian Zhang 1 , Khine S. Shan 2 , Babatunde A. Ogunnaike 1 , Atsoufui Amewuame-Kpehor 1 , Travis Nace 3 1. Internal Medicine, Abington Hospital-Jefferson Health, Abington, USA 2. Internal Medicine, University of Maryland Medical Center, Baltimore, USA 3. Library Science, Abington Hospital-Jefferson Health, Abington, USA Corresponding author: Qian Zhang, [email protected] Abstract Macrocytic anemia is usually associated with vitamin B12 or folate deficiency. -

The Chemistry of Hematology
The Chemistry of Hematology Gary L. Horowitz, MD Beth Israel Deaconess Medical Center Boston, MA Objectives • Explain how methylmalonic acid and homocysteine are related to B12 and folate deficiencies • List the common laboratory findings in iron deficiency anemia • Describe the chemical and molecular approaches to screening for Hereditary Hemochromatosis Topics to be Covered • Oxygen Concentration – Hemoglobin Species • D-Dimer – Separate talk later in course • Anemia – Hemolysis – Macrocytic Anemia – Microcytic Anemia Analytes • Hemoglobins • Vitamin B12 (cobalamin) – Oxyhemoglobin • Folic Acid – Reduced (Deoxy) • Homocysteine Hemoglobin • Methylmalonic Acid – Methemoglobin – Carboxyhemoglobin • D-Dimer • Iron • Transferrin/TIBC • LD (LD isoenzymes) • Ferritin • Haptoglobin Topics to be Covered • Oxygen Concentration – Hemoglobin Species • D-Dimer – Separate talk later in course • Anemia – Hemolysis – Macrocytic Anemia – Microcytic Anemia O2 Concentration in Blood • not simply PaO2 • not simply Hct (or, more precisely, Hgb) • not simply O2 saturation • rather, a combination of all 3, “O2 content” mm Hg g/dL = 0.003 * PO2 + 1.4 * [Hgb] * [%O2sat] = 0.0225 * PO2 + 1.4 * [Hgb] * [%O2sat] kPa g/dL Different Scenarios Illustrating Oxygen Content Concepts Hgb- Dissolved O2 comments PaO2 %O2Sat Hgb Hct Bound Oxygen Content O2 Normal 100 100 14 42 0.3 19.6 19.9 Low Hct 100 100 7 21 0.3 9.8 10.1 Low PaO2 25 50 14 42 0.1 9.8 9.9 (lung disease) 50% 100 50 14 42 0.3 9.8 10.1 Methemoglobin Very Low Hct 100 100 2 6 0.3 2.8 3.1 No Transfusion Hyperbaric -

Drugs for Parasitic Infections (2013 Edition)
The Medical Letter publications are protected by US and international copyright laws. Forwarding, copying or any other distribution of this material is strictly prohibited. For further information call: 800-211-2769 Drugs for Parasitic Infections With increasing travel, immigration, use of immunosuppressive drugs and the spread of HIV, physicians anywhere may see infections caused by parasites. The table below lists first- choice and alternative drugs for most parasitic infections. The principal adverse effects of these druugs are listed on pages e24-27. The table that begins on page e28 summarizes the known pre- natal risks of antiparasitic drugs. The brand names and manufacturers of the drugs are listed on pages e30-31. ACANTHAMOEBA keratitis Drug of choice: Keratitis is typically associated with contact lens use.1 A topical biguanide, 0.02% chlorhexi- dine or polyhexamethylene biguanide (PHMB, 0.02%), either alone or combined with a diami- dine, propamidine isethionate (Brolene) or hexamidine (Desomodine), have been used suc- cessfully.2 They are administered hourly (or alternating every half hour) day and night for the first 48 hours and then continued on a reduced schedule for days to months.3 None of these drugs is commercially available or approved for use in the US, but they can be obtained from compounding pharmacies. Leiter’s Park Avenue Pharmacy, San Jose, CA (800-292-6773; www.leiterrx.com) is a compounding pharmacy that specializes in ophthalmic drugs. Expert Compounding Pharmacy, 6744 Balboa Blvd., Lake Balboa, CA 91406 (800-247-9767) and Medical Center Pharmacy, New Haven, CT (203-688-7064) are also compounding pharmacies. -
Hematology for Family Practice When to Treat and When to Refer
Hematology for Family Practice When to treat and when to refer Karen deGenevieve MSN, FNP,BC OCN Objectives: 1. Identify types of anemia's by analyzing indices, and appropriate tests. 2. Understand manual differential and terminology. 3. Discuss abnormalities in platelets and white cells, and determine appropriate testing. Objectives continued: 4. Discuss treatment options for hematologic conditions and medication management. 5. Know when to refer. 1. Anemia's and Erythrocytosis 2. Low platelets and High platelets 3. Leukopenia's and Leukocytosis How long do cells live? • Red blood cells live approximately 120 days. • Platelets live 8 -11 days. • White blood cells live about 4 days. There are millions of RBCs in just one drop of blood. People who live at higher altitudes have more (like in the mountains of Peru). They are produced in the bone marrow of large bones at a rate of 2 million per second. In the minute it took you to read this, you made 120 million of them! Anemia’s And Erythrocytosis First thing to do with an abnormal CBC is to repeat it and get a smear to pathology, manual diff, and reticulocyte count. MICROCYTOSIS: Low MCV (mean corpuscular volume) under 80. Low MCH (mean corpuscular hemoglobin) under 27. Low MCHC (mean corpuscular hemoglobin concentration) under 30. MACROCYTOSIS: High MCV over 93 High MCH over 33 High MCHC over 37 NORMOCYTIC ANEMIA: NOMAL INDICIES DEFINITIONS Reticulocyte: The youngest of the circulating red cells, normally they comprise about 1% of the red cell population. They are increased in response to bleeding, or hemolysis, or in response to treatment with B 12, iron, of folic acid. -

Diagnosis of Anemia in Pregnancy
Review Article Page 1 of 5 Diagnosis of anemia in pregnancy Ahmad Al-Khaffaf, Francesco Frattini, Roberta Gaiardoni, Elda Mimiola, Cinzia Sissa, Massimo Franchini Department of Hematology and Transfusion Medicine, Carlo Poma Hospital, Mantua, Italy Contributions: (I) Conception and design: A Al-Khaffaf, M Franchini; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: None; (V) Data analysis and interpretation: None; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Massimo Franchini, MD. Department of Hematology and Transfusion Medicine, Carlo Poma Hospital, Mantua, Italy. Email: [email protected]. Abstract: Anemia in pregnancy is a worldwide health and social problem. While some degree of dilutional anemia is very frequent and can be considered part of the normal physiology of pregnancy, iron deficiency anemia is likewise common during pregnancy but can have serious adverse health consequences for the mother and child. Thus, it is mandatory to perform a prompt diagnosis of iron deficiency anemia distinguishing it from physiologic anemia, as well as to identify other less common causes of anemia that may require treatment. In this narrative review, we summarize the main diagnostic, clinical and therapeutic characteristics of the most important types of anemia during pregnancy. Keywords: Anemia; pregnancy; iron deficiency; sickle cell anemia, diagnosis Received: 07 November 2019; Accepted: 06 December 2019; Published: 20 January 2020. doi: 10.21037/jlpm.2019.12.03 View this article at: http://dx.doi.org/10.21037/jlpm.2019.12.03 Introduction Iron deficiency anemia During normal pregnancy, the plasma volume expands Iron deficiency accounts for 75% of cases of non- by 40–60%, whereas the red blood cell mass expands physiologic anemia in pregnancy, and the incidence of iron by 20–50%.