Squamous Cell Carcinoma Including Actinic Keratosis, Bowen's Disease
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

In Dermatology Visit with Me to Discuss
From time to time new treatments surface for any medical field, and the last couple of years have seen new treatments emerge, or new applications for familiar treatments. I wanted to summarize some of these New Therapies widely available remedies and encourage you to schedule a in Dermatology visit with me to discuss. Written by Board Certified Dermatologist James W. Young, DO, FAOCD Nicotinamide a significant reduction in melanoma in Antioxidants Nicotinamide (niacinamide) is a form high risk skin cancer patients at doses Green tea, pomegranate, delphinidin of vitamin B3. The deficiency of vitamin more than 600 and less than 4,000 IU and fisetin are all under current study for daily. B3 causes pellagra, a condition marked either oral or topical use in the reduction by 4D’s – (photo) Dermatitis, Dementia, Polypodium Leucotomos of the incidence of skin cancer, psoriasis Diarrhea and (if left untreated) Death. and other inflammatory disorders. I’ll be Polypodium leucotomos is a Central This deficiency is rare in developed sure to keep patients updated. countries, but is occasionally seen America fern that is available in several in alcoholism, dieting restrictions, or forms, most widely as Fernblock What Are My Own Thoughts? malabsorption syndromes. Nicotinamide (Amazon) or Heliocare (Walgreen’s and I take Vitamin D 1,000 IU and Heliocare does not cause the adverse effects of Amazon) and others. It is an antioxidant personally. Based on new research, I Nicotinic acid and is safe at doses up to that reduces free oxygen radicals and have also added Nicotinamide which 3,000mg daily. may reduce inflammation in eczema, dementia, sunburn, psoriasis, and vitiligo. -

Pilar Sheath Acanthoma Presenting As a Nevus
Letter to Editor Pilar Sheath Acanthoma Presenting as a Nevus Sir, Pilar sheath acanthoma (PSA) is a rare benign follicular neoplasm, which was first described by Mehregan and Brownstein in 1978.[1] PSA usually presents as an asymptomatic, flesh colored papule with a central opening localized at the lower lip with exceptional presentations such as ear lobe, postauricular region, or cheek.[1‑3] A 42‑year‑old female referred with a solitary, slow‑growing nodular lesion at the upper lip region for 6 months. Physical exam revealed a 4 mm, pink‑brown colored nodule with a central opening [Figure 1]. Under clinical prediagnosis of melanocytic nevus, an excisional biopsy Figure 1: Physical examination of the nodule in the upper lip region was performed. In a microscopic examination, a cystic cavity that communicated with surface epidermis has been observed. The wall of the cystic cavity was composed of solid tumor islands extending in the deep dermis [Figure 2]. The cavity was lined with stratified squamous epithelium filled with keratin [Figure 3]. PSA is an uncommon, benign follicular tumor occurring in the faces of middle‑aged and elderly patients. These lesions can present at any location such as cheek, ear lobe on the head, and neck. In our case, a 42‑year‑old female was presented with a pink‑brown colored nodular lesion opening at the upper lip region. The differential diagnosis includes trichofolliculoma and dilated pore of Winer. Trichofolliculomas contain many seconder hair follicles Figure 2: A central cavity with keratin in the dermis which is continuous radiating from the wall of the primary follicle with outer with the surface epithelium (H and E, ×40) and inner root sheaths in a well‑formed stroma which are absent in PSA. -

Actinic Keratoses Final Report
Actinic Keratoses Final Report Mark Helfand, MD, MPH Annalisa K. Gorman, MD Susan Mahon, MPH Benjamin K.S. Chan, MS Neil Swanson, MD Submitted to the Agency for Healthcare Research and Quality under contract 290-97-0018, task order no. 6 Oregon Health & Science University Evidence-based Practice Center 3181 SW Sam Jackson Park Road Portland, Oregon 97201 May 19, 2001 Actinic Keratoses Structured Abstract Objective: To examine evidence about the natural history and management of actinic keratoses (AKs). Search Strategy: We searched the MEDLINE database from January 1966 to January 2001, the Cochrane Controlled Trials Registry, and a bibliographic database of articles about skin cancer. We identified additional articles from reference lists and experts. Selection Criteria: We selected 45 articles that contained original data relevant to treatment of actinic keratoses, progression of AKs to squamous cell cancer (SCC ), means of identifying a high-risk group, or surveillance of patients with AKs to detect and treat SCCs early in their course. Data Collection and Analysis: We abstracted information from these studies to construct evidence tables. We also developed a simple mathematical model to examine whether estimates of the rate of progression of AK to SCC were consistent among studies. Finally, we analyzed data from the Medicare Statistical System to estimate the frequency of procedures attributable to AK among elderly beneficiaries. Main Results: The yearly rate of progression of an AK in an average-risk person in Australia is between 8 and 24 per 10,000. High-risk individuals with multiple AKs have progression rates as high as 12-30 percent over 3 years. -

The Tamilnadu Dr. M.G.R. Medical University Chennai, Tamil Nadu
CLINICO-PATHOLOGICAL STUDY OF SKIN SURFACE EPIDERMAL AND APPENDAGEAL TUMOURS Dissertation Submitted in partial fulfillment of university regulations for M.D. DEGREE IN DERMATOLOGY, VENEREOLOGY AND LEPROSY BRANCH XII – A THE TAMILNADU DR. M.G.R. MEDICAL UNIVERSITY CHENNAI, TAMIL NADU SEPTEMBER 2006 CERTIFICATE This is to certify that this Dissertation entitled “CLINICO-PATHOLOGICAL STUDY OF SKIN SURFACE EPIDERMAL AND APPENDAGEAL TUMOURS” is a bonafide work done by DR.G.BALAJI, Postgraduate student of Department of Dermatology, Leprosy and Institute of STD, Madras Medical College and Government General Hospital, Chennai – 3 for the award of Degree of M.D.( Dermatology, Venereology and Leprosy ) Branch XII – A during the academic year of 2003-2006. This work has not previously formed in the basis for the award of any degree or diploma. Prof. Dr. B. Parveen, MD., DD., Professor & Head, Dept. of Dermatology and Leprosy, Madras Medical College & Govt. General Hospital, Chennai – 3. Prof. Dr. Kalavathy Ponniraivan, MD., The Dean Madras Medical College & Govt. General Hospital, Chennai – 3. SPECIAL ACKNOWLEDGEMENT I sincerely thank Prof. Dr. Kalavathy Ponniraivan, MD., Dean, Madras Medical College & Govt. General Hospital, Chennai – 3, for granting me permission to use the resources of this institution for my study. ACKNOWLEDGEMENT I sincerely thank Prof. B.Parveen MD.,DD, Professor and Head of Department of Dermatology for her invaluable guidance and encouragement for the successful completion of this study. I express my heart felt gratitude to Dr.N.Gomathy MD.,DD, former Head of department of Dermatology who was instrumental in the initiation of this project, giving constant guidance throughout my work. -

What Are Basal and Squamous Cell Skin Cancers?
cancer.org | 1.800.227.2345 About Basal and Squamous Cell Skin Cancer Overview If you have been diagnosed with basal or squamous cell skin cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to start. ● What Are Basal and Squamous Cell Skin Cancers? Research and Statistics See the latest estimates for new cases of basal and squamous cell skin cancer and deaths in the US and what research is currently being done. ● Key Statistics for Basal and Squamous Cell Skin Cancers ● What’s New in Basal and Squamous Cell Skin Cancer Research? What Are Basal and Squamous Cell Skin Cancers? Basal and squamous cell skin cancers are the most common types of skin cancer. They start in the top layer of skin (the epidermis), and are often related to sun exposure. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Cancer starts when cells in the body begin to grow out of control. Cells in nearly any part of the body can become cancer cells. To learn more about cancer and how it starts and spreads, see What Is Cancer?1 Where do skin cancers start? Most skin cancers start in the top layer of skin, called the epidermis. There are 3 main types of cells in this layer: ● Squamous cells: These are flat cells in the upper (outer) part of the epidermis, which are constantly shed as new ones form. When these cells grow out of control, they can develop into squamous cell skin cancer (also called squamous cell carcinoma). -

Prior Authorization Criteria
PRIOR AUTHORIZATION CRITERIA Last Updated 09/01/2021 This is a complete list of drugs that have written coverage determination policies. Drugs on this list do not indicate that this particular drug will be covered under your medical or prescription drug benefit. Please verify drug coverage by checking your formulary and member handbook. Additional restrictions and exclusions may apply. If you have questions, please contact Providence Health Plan Customer Service at 503-574-7500 or 1-800-878-4445 (TTY: 711). Service is available five days a week, Monday through Friday, between 8 a.m. and 6 p.m. ACTINIC KERATOSIS AGENTS MEDICATION(S) CARAC, FLUOROURACIL 0.5% CREAM, IMIQUIMOD 3.75% CREAM, IMIQUIMOD 3.75% CREAM PUMP, KLISYRI, PICATO, TOLAK, ZYCLARA COVERED USES N/A EXCLUSION CRITERIA • Treatment of basal cell carcinoma or other skin cancers REQUIRED MEDICAL INFORMATION 1. For the treatment of Actinic Keratosis (AK): Documentation of trial and failure*, contraindication or intolerance to two of the following formulary, generic topical agents: a. Diclofenac 3% gel b. 5-fluorouracil 2% or 5% cream/solution c. Imiquimod 5% cream *An adequate trial and failure is defined as failure to achieve clearance of AK lesion(s) after adherence to recommended treatment dosing and duration Reauthorization: Requires documentation of a reduction in the number and/or size of lesions of AK and medical rationale for continuing therapy beyond recommended treatment course. 1. For the treatment of external genital and perianal warts/condyloma acuminate (Zyclara® 3.75% only): Documentation of trial and failure*, contraindication, or intolerance to formulary, generic imiquimod 5% cream. -

What to Expect Following Cryosurgery “Freezing”
What to Expect Following CryoSurgery “Freezing” What is Cryosurgery? Cryosurgery is a technique for removing skin lesions that primarily involve the surface of the skin, such as warts, seborrheic keratosis, or actinic keratosis. It is a quick method of removing the lesions with minimal scarring. The liquid nitrogen needs to be applied long enough to freeze the affected skin. By freezing the skin, a blister is created underneath the lesion. Ideally, as the new skin forms underneath the blister, the abnormal skin on the roof of the blister peels off. Occasionally if the lesion is very thick (such as a large wart), only the surface is blistered off. The base or residual lesion may need to be frozen at another visit. What to Expect Over the Next Few Weeks? During Treatment – Area being treated will sting, burn and then possibly itch. Immediately After Treatment – Area will be red sore and swollen. Next Day- Blister or blood blister has formed, tenderness starts to subside. Apply a Band-Aid if necessary. 7 Days- Surface is dark red/brown and scab-like. Apply Vaseline or an antibacterial ointment if necessary. 2 to 4 Weeks- The surface starts to peel off. This may be encouraged gently during bathing, when the scab is softened. No makeup should be applied until area is fully healed. How to Take care of the Skin after Cryosurgery A Band-Aid can be used for larger blisters or blisters in areas that are more likely to be traumatized- such as fingers and toes. If the area becomes dry or crusted, an ointment (Vaseline, Aquaphor) can also be applied. -

Hair Follicle Tumors
Hair Follicle Tumors 803-808-7387 www.gracepets.com These notes are provided to help you understand the diagnosis or possible diagnosis of cancer in your pet. For general information on cancer in pets ask for our handout “What is Cancer”. Your veterinarian may suggest certain tests to help confirm or eliminate diagnosis, and to help assess treatment options and likely outcomes. Because individual situations and responses vary, and because cancers often behave unpredictably, science can only give us a guide. However, information and understanding for tumors in animals is improving all the time. We understand that this can be a very worrying time. We apologize for the need to use some technical language. If you have any questions please do not hesitate to ask us. What is this tumor? This is one of many similar tumors that arise by disordered growth of the hair follicles. These tumors are almost all benign and can be permanently cured by total surgical removal. Some occur at multiple sites within the same animal. This family of tumors grade into each other. Precise nomenclature is usually irrelevant as almost all are benign. What do we know about the cause? The reason why a particular pet may develop this, or any cancer, is not straightforward. Cancer is often seemingly the culmination of a series of circumstances that come together for the unfortunate individual. Cross Section of Skin & Hair Follicle B-catenin is required for differentiation of skin cells into hair follicles. If there is over-production of this chemical in the body, hair follicle tumors develop. -

Expert-Level Diagnosis of Nonpigmented Skin Cancer by Combined Convolutional Neural Networks
Supplementary Online Content Tschandl P, Rosendahl C, Akay BN, et al. Expert-level diagnosis of nonpigmented skin cancer by combined convolutional neural networks. JAMA Dermatol. Published online November 28, 2018. doi:10.1001/jamadermatol.2018.4378 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set eAppendix. Neural Network Training eTable 1. Complete List of Diagnoses and Their Frequencies Within the Test-Set eTable 2. Education of Users According to Their Experience Group eTable 3. Percent of Correct Prediction of the Malignancy Status for Specific Diagnoses of a CNN Using Either Close-up or Dermatoscopic Images This supplementary material has been provided by the authors to give readers additional information about their work. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eFigure. Sensitivities (Blue) and Specificities (Orange) at Different Threshold Cutoffs (Green) of the Combined Classifier Evaluated on the Validation Set A threshold cut at 0.2 (black) is found for a minimum of 51.3% specificity. © 2018 American Medical Association. All rights reserved. Downloaded From: https://jamanetwork.com/ on 09/25/2021 eAppendix. Neural Network Training We compared multiple architecture and training hyperparameter combinations in a grid-search fashion, and used only the single best performing network for dermoscopic and close-up images, based on validation accuracy, for further analyses. We trained four different CNN architectures (InceptionResNetV2, InceptionV3, Xception, ResNet50) and used model definitions and ImageNet pretrained weights as available in the Tensorflow (version 1.3.0)/ Keras (version 2.0.8) frameworks. -

Lumps & Bumps: Approach to Common Dermatologic Neoplasms
Case-Based Approach to Common Dermatologic Neoplasms Patrick Retterbush, MD, FAAD Mohs Surgery & Dermatologic Oncology Associate Member of the American College of Mohs Surgery Private Practice: Lockman Dermatology January 27th 2018 Disclosure of Relevant Financial Relationships • I do not have any relevant financial relationships, commercial interests, and/or conflicts of interest regarding the content of this presentation. Goals/Objectives • Recognize common benign growths • Recognize common malignant growths • Useful clues & examination for evaluating melanocytic nevi and when to be concerned for melanoma/atypical moles • How to perform a basic skin biopsy and which method/type to choose • Basic treatment/when to refer Key Questions & Physical Examination Findings for a Growth History Physical Examination • How long has the lesion been • Describing a growth present? – flat or raised? • flat – macule (<1cm) or patch (>1cm) – years, months, weeks • raised – papule (<1cm) or plaque (>1cm) – nodule if deep (majority of lesion in • Has it changed? dermis/SQ) – Size – secondary descriptive features • scaly (hyperkeratosis, retention of strateum – Shape corneum) – Color • crusty (dried serum, blood, or pus on surface) • eroded or ulcerated (partial vs. full thickness – Symptoms – pain, bleeding, itch? epidermal loss) – Over what time frame? • color (skin colored, red, pigmented, pearly) • feel (hard or soft, mobile or fixed) • PMH: • size: i.e. 6 x 4mm – prior skin cancers • Look at the rest of the skin/region of skin • SCC/BCCs vs. melanoma -
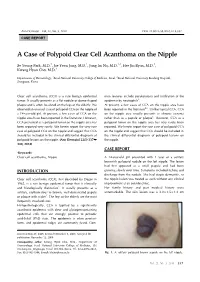
A Case of Polypoid Clear Cell Acanthoma on the Nipple
Ann Dermatol Vol. 22, No. 3, 2010 DOI: 10.5021/ad.2010.22.3.337 CASE REPORT A Case of Polypoid Clear Cell Acanthoma on the Nipple Se Young Park, M.D.1, Jae Yoon Jung, M.D.1, Jung Im Na, M.D.1,2, Hee Jin Byun, M.D.1, Kwang Hyun Cho, M.D.1 Departments of Dermatology, 1Seoul National University College of Medicine, Seoul, 2Seoul National University Bundang Hospital, Seongnam, Korea Clear cell acanthoma (CCA) is a rare benign epidermal mon features include parakeratosis and infiltration of the tumor. It usually presents as a flat nodule or dome-shaped epidermis by neutrophils3. plaque and is often localized on the legs of the elderly. We At present, a few cases of CCA on the nipple area have observed an unusual case of polypoid CCA on the nipple of been reported in the literature4-6. Unlike typical CCA, CCA a 14-year-old girl. At present, a few cases of CCA on the on the nipple area usually presents as chronic eczema nipple area have been reported in the literature. However, rather than as a papule or plaque6. However, CCA as a CCA presented as a polypoid tumor on the nipple area has polypoid tumor on the nipple area has very rarely been been reported very rarely. We herein report the very rare reported. We herein report the rare case of polypoid CCA case of polypoid CCA on the nipple and suggest that CCA on the nipple and suggest that CCA should be included in should be included in the clinical differential diagnosis of the clinical differential diagnosis of polypoid lesions on polypoid lesions on the nipple.