Optic Disc Pit Maculopathy: When and How to Treat?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gas Tamponade Combined with Laser Photocoagulation Therapy
Eye (2015) 29, 106–114 & 2015 Macmillan Publishers Limited All rights reserved 0950-222X/15 www.nature.com/eye 1,4 1,4 1,4 1 1 2 CLINICAL STUDY Gas tamponade L Lei ,TLi , X Ding ,WMa, X Zhu , A Atik , YHu1 and S Tang1,3 combined with laser photocoagulation therapy for congenital optic disc pit maculopathy Abstract Purpose To evaluate the long-term clinical Introduction efficacy and safety of gas tamponade Optic disc pit (ODP) is part of a spectrum of combined with laser photocoagulation for congenital cavitary optic disc anomalies which optic disc pit maculopathy. was seen in o1/11 000 patients.1 The pit lesions Methods Seven consecutive patients with are typically unilateral, oval, and gray-white unilateral maculopathy associated with 1State Key Laboratory of depressions located in the temporal segment of optic disc pit and one patient with bilateral Ophthalmology, Zhongshan the optic disc and frequently involve the macula Ophthalmic Center, Sun Yat- optic disc pit maculopathy were given via intra-retinal and sub-retinal fluid collections.2 sen University, Guangzhou, octafluoropropane (C3F8) tamponade Visual acuity and visual fields are normal unless China combined with focal laser photocoagulation associated with serous macular detachment. treatment. Patients were followed up for 2Royal Victorian Eye and Ear The mechanisms underlying this disease are 21–62 months after treatment. Main Hospital, Melbourne, VIC, unclear, especially in relation to intra-retinal Australia outcomes were determined by optical coherence tomography (OCT) and best- and sub-retinal fluid accumulation. ODP maculopathy (ODPM) was first described by 3Aier School of corrected visual acuity (BCVA). -
Optic Nerve on Sheath:
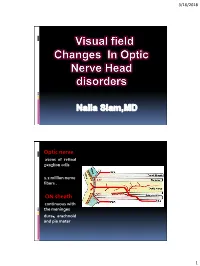
3/16/2018 < Optic nerve axons of retinal ganglion cells 1.2 million nerve fibers . ON sheath: continuous with the meninges dura、arachnoid and pia mater 1 3/16/2018 optic nerve functions 1.Visual Acuity 2.Color Vision 3.Pupil 4.Contrast sensitivity Ancillary Tests 1.Visual Field 2.Neuro-imaging 3.OCT 4.VEP Etiology:Optic nerve diseases 1.inflammation:optic neuritis 2 . ischemic optic neuropathy 3-Compression 4-Granuloma & infiltration 5-Hereditary 6-Toxic 7-Irradiation 8- Trauma . 2 3/16/2018 Optic Neuritis 3-Neuroretinitis 1-Retrobulbar neuritis 2-Papillitis Papillitis optic disc is normal hyperemia and edema with macular star . in adults common in children. least common type with multiple sclerosis. viral infections Rapid unilateral loss of vision RAPD Loss of color vision Pain in moving the eye Swollen disc with or without peripapillary flame-shaped hemorrhages. 3 3/16/2018 Fig optic neuritis Centrocecal scotoma Bilateral optic neuritis Bilateral Central scotoma 4 3/16/2018 Bilateral hemianopsia MRI demyelinating lesions multiple sclerosis Neuromylitis Optica VF showed non- central scotoma altitudinal VF an ischemic mechanism play a role in ON in NMO patients 5 3/16/2018 Optic Neuritis Follow Up Diffuse and central loss in the affected eye at baseline Follow Up : nerve fiber bundle defects were the predominant localized abnormalities in both the affected and fellow eyes physicians evaluate the characteristics of optic neuritis and other optic neuropathies in the future Ischemic optic neuropathy ( ION) 6 3/16/2018 Anterior ischemic optic neuropathy ( AION ) Arteritic Non- Arteritic GCA - vasculitis hypoperfusion of ONH transient visual loss, temporal sudden painless loss of vision pain, jaw pain, fatigue, weight loss hyperemic disc Pale disc Sectorial, diffuse edema optic disc edema splinter hemorrhages of a chalky white color Subsequent optic atrophy Nonarteritic ischemic optic neuropathy visual field altitudinal field defect 7 3/16/2018 NAION sudden, painless visual loss OS shows AION . -

Japanese Journal of Ophthalmology Vol.41 No.5
ELSEVIER Abnormal Vitreous Structure in Optic Nerve Pit Tomoki Hasegawa, Jun Akiba, Satoshi Ishiko, Taiichi Hikichi, Akihiro Kakehashi, Hiroyuki Hirokawa and Akitoshi Yoshida Department of Ophthalmology, Asahikawa Medical College, Asahikawa, Japan Abstract: A 37-year-old man presented with an optic nerve pit and serous macular detach- ment of the left eye. Scanning laser ophthalmoscopy revealed a cyst-like structure terminat- ing at the pit in the premacular vitreous. During ocular movement, this structure moved vig- orously and seemed to exert traction on the pit. We believe that it is part of an anomalous Cloquet’s canal, and that traction on the pit may be a significant factor in the development of serous macular detachment in this patient. Jpn J Ophtbalmol 1997;41:32&327 0 1997 Japanese Ophthalmological Society Key Words: Cloquet’s canal, optic nerve pit, scanning laser ophthalmoscope, serous macu- lar detachment, vitreous. Introduction ular detachment in this patient. This case has been included in previously published reports on SLO An optic nerve pit is a rare congenital anomaly images.8,g that occurs in approximately 1 in 10 000 eyes.’ In early adulthood, half of the patients with this condi- tion develop a serous macular detachment;2,3 the mechanism of this development is not yet clear. Al- Case Report though several theories on the origin of subretinal A 37-year-old man visited our ophthalmology de- fluid have been proposed, the currently favored un- partment on February 15,1996 with blurred vision in derstanding is that fluid from the vitreous leaks the left eye. Initial examination found best-corrected through the optic pit, filling the subretinal space.’ visual acuities of 1.0 OD and 0.2 OS. -

Resolution Ofan External Layer Macular Hole Associated with An
BritishJournal ofOphthalmology 1993; 77: 457-459 457 Resolution of an external layer macular hole associated with an optic nerve pit after laser Br J Ophthalmol: first published as 10.1136/bjo.77.7.457 on 1 July 1993. Downloaded from photocoagulation Philip M Falcone, Peter L Lou Optic nerve pits are estimated to occur in 1 in 11000 patients.'2 Maculopathy associated with optic nerve pits occurs in 30%-63%23 and is characteristically described as a serous retinal detachment. Brown et al3 reviewed 75 patients with optic nerve pits and found that 24 of the 38 patients with macular detachments had cystic changes in the macula. Lamellar macular holes were present in the outer layer of the retina in 10 ofthe 24 eyes. Lincoff et al noted an associated retinoschisis in patients with optic pits. A macular hole was observed in the outer retinal layer in 14 out ofthe 15 eyes examined and was associated with severely diminished visual acuity. We now present a case of an optic nerve pit Figure 2 Earlyframefluorescein angiography discloses with retinoschisis and a outer layer detachment hypofluorescence ofthe optic nerve pit with an RPE with an external layer macular hole that was transmission defect in thefovea. treated promptly with krypton red barrier photocoagulation. The marked visual improve- had a 0-2 cup/disc ratio with a optic pit at the ment seen in our patient corresponded to the temporal border. A schisis-like elevation of the resolution of the external layer macular hole retina was observed extending temporally from observed clinically and on fluorescein the optic pit to the macula area. -

Challenges in Optic Disc Pit Maculopathy Treatment
Challenges in Optic Disc Pit Maculopathy Treatment Many techniques have been described; choose the best one for the individual patient. BY BARBARA PAROLINI, MD; AND MICHELE PALMIERI, MD ptic disc pit (ODP) is a rare congenital abnormality ODP MACULOPATHY of the optic nerve head, first described by Wiethe in ODP is usually asymptomatic, but a percentage of affected 1882.1 ODP usually appears as a grayish-whitish, round patients (25%-75% depending on the report) may develop a or oval depression of the optic disc (Figure 1A), and it macular serous detachment or a retinoschisis-like maculopa- may have different levels of severity. It is a spectrum of thy due to the presence, respectively, of subretinal or intra- Ocongenital cavitary anomalies of the optic disc, ranging from retinal fluid.3,6,9 This condition, known as ODP maculopathy the more common optic pit to the so-called morning glory (ODPM), causes visual impairment, especially in long-stand- syndrome (Figure 1B) to coloboma not only of the optic ing cases, in which lamellar or full-thickness macular holes nerve but also of the choroid (Figure 1C). It is also found in and retinal pigment epithelium atrophy may appear.10-12 the papillorenal syndrome determined by a mutation of the The exact mechanism of the pathophysiology of ODPM PAX2 gene. and the origin of the fluid remain unclear. It has been pro- ODP is bilateral in 15% of cases (Figure 2) and occurs posed that vitreous or cerebrospinal fluid (CSF) may be the equally in men and women with an estimated incidence of origin of the fluid -

Multicenter Study of Pars Plana Vitrectomy for Optic Disc Pit
Eye (2017) 31, 1266–1273 © 2017 Macmillan Publishers Limited, part of Springer Nature. All rights reserved 0950-222X/17 www.nature.com/eye 1 2 3 4 5 CLINICAL STUDY Multicenter study of R Avci , Z Kapran ,S¸ Ozdek , MY Teke ,OOz, D Guven6, S Yilmaz1, B Kaderli7, AH Durukan8, pars plana vitrectomy G Sobaci9, YB Unver10, L Akduman11, for optic disc pit S Kaynak12, I Dogan13 and UU Inan14 maculopathy: MACPIT study Abstract 1Department of Ophthalmology, Retina Eye Hospital, Bursa, Turkey Purpose To evaluate surgical intervention except an arcuate scotoma or enlarged blind spot 2Department of Ophthalmology, Maltepe University Medical School, with pars plana vitrectomy (PPV) for in some cases. However, vision deteriorates if Istanbul, Turkey correction of optic disc pit maculopathy optic disc pit maculopathy (ODP-M) consisted 3Department of Ophthalmology, Gazi (ODP-M). mainly of serous macular detachment or University Medical School, Ankara, – Turkey Patients and methods Retrospective chart macular schisis develops.2 6 4Department of Ophthalmology, review from 13 centres of 51 eyes of 50 Although pars plana vitrectomy (PPV) is Ulucanlar Eye Education and Research Hospital, Ankara, Turkey patients with ODP-M who underwent PPV generally accepted as the standard procedure for – fi 5Department of Ophthalmology, Adana between 2002 2014. Anatomic and nal best- the management of ODP-M, the need for various – Retina Eye Center, Adana, Turkey corrected visual acuity (BCVA) outcomes adjuvant therapies has not been well studied.4 10 6Department of Ophthalmology, Sisli were evaluated for all cases with different Etfal Education and Research Hospital, The current study was designed in an attempt to Istanbul, Turkey adjuvant techniques. -

An Insight Into the Pathogenesis of Optic Disc Pit–Associated Maculopathy with Enhanced Depth Imaging
Research Brief Report An Insight Into the Pathogenesis of Optic Disc Pit–Associated Maculopathy With Enhanced Depth Imaging Jaitra P. Gowdar, DNB; Bindu Rajesh, MS; Anantharaman Giridhar, MS; Mahesh Gopalakrishnan, MS; Rameez Hussain, MS; Thomas Thachil, MS IMPORTANCE Optic disc pit with associated maculopathy is a known entity. However, controversy exists regarding the source of subretinal fluid in these cases. In our series, we attempted to analyze the morphologic changes seen in the optic disc pit and evaluate the source of subretinal fluid. OBSERVATIONS In this prospective observational case series of 4 patients with optic pit maculopathy, a complete ophthalmic evaluation, with fundus color photography and enhanced depth imaging spectral-domain optical coherence tomography scanning of the optic disc, was carried out between January 2013 and November 2013. The optical coherence tomographic section was mapped with infrared image and color photography, and the characteristics of the retina and optic nerve head were analyzed. All the cases had outer layer retinal schisis; 2 of them had associated serous macular detachment while inner retinal schisis was present in 3 cases. A hyporeflective tract was observed in our study connecting the retinal schisis cavity and gap in the lamina cribrosa corresponding to the optic pit. CONCLUSIONS AND RELEVANCE In our study, we demonstrated the connectivity between retinal schisis and the gap in the lamina cribrosa present in the optic disc pit, supporting the Author Affiliations: Giridhar Eye hypothesis of cerebrospinal fluid as the source of subretinal fluid. Institute, Kerala, India. Corresponding Author: Bindu Rajesh, MS, Giridhar Eye Institute, JAMA Ophthalmol. 2015;133(4):466-469. -

Optic Nerve Cyst Associated with Optic Disc Pit in a Child with Multi-Cystic Kidney
Central JSM Clinical Case Reports Case Report *Corresponding author Verlyn Yang, Department of Ophthalmology, Gold Coast University Hospital, Australia, Email: yangverlyn@ Optic Nerve Cyst Associated gmail.com Submitted: 16 August, 2020 with Optic Disc Pit in a Child Accepted: 08 September, 2020 Published: 09 September, 2020 Copyright © 2020 Yang V, et al. with Multi-Cystic Kidney ISSN: 2373-9819 OPEN ACCESS Verlyn Yang1*, Sandeep Bhuta2, and Aditi Kirpalani1 1Department of Ophthalmology, Gold Coast University Hospital, Australia Keywords 2Department of Radiology, Gold Coast University Hospital, Australia • Optic nerve cys • Optic disc pit • Coloboma Abstract • ODP-M In this case report, we present an unusual case of a 7-year-old female who came to the attention of the Ophthalmology department for reduced vision in the right eye 6/18 (LogMAR 0.4) with normal vision in the left eye. Fundoscopic examination revealed signs of an optic disc coloboma associated with an optic disc pit with adjacent sub-retinal fluid extending to the macula. She was born with a left multi-cystic kidney. Further work-up in the form of MRI and USG Orbits demonstrated a well-defined optic pit at the optic nerve head and a tubular channel extending to a 6-7mm multi-cystic lesion. ABBREVIATIONS mother had been diagnosed with Stragardt’s disease. There were no other systemic, familial or genetic conditions of note. Optic disc pit maculopathy (ODP-M); Magnetic Resonance Imaging (MRI) On examination, her visual acuity was noted to be right eye: INTRODUCTION Congenital optic disc pit is an uncommon congenital nerve6/18 (LogMAR appearance 0.4), in left the eye: right 6/9 eye (LogMAR on fundus 0.1), examination. -
Glaucoma and the Optic Nerve Naida Jakirlic, OD, FAAO Western University of Health Sciences College of Optometry
Glaucoma and the Optic Nerve Naida Jakirlic, OD, FAAO Western University of Health Sciences College of Optometry September 13, 2015 Learning objectives • Review the anatomy of the optic nerve • Recognize the appearance of the healthy optic nerve • Ascertain the critical components of optic nerve assessment • Identify possible glaucomatous changes of the optic nerve, peripapillary region, and RNFL • Identify the cardinal features of glaucomatous optic neuropathy • Analyze optic nerve images to solidify today’s discussion What is glaucoma? . A progressive optic nerve disease characterized by retinal ganglion cell death and resultant axon loss seen as excavation of the optic nerve head with consequent defects in retinal sensitivity that can be measured with visual field tests What is glaucoma? • Optic neuropathy • Axon loss • Excavation of the optic nerve • Resultant VF defects Glaucomatous damage may be due to • Elevated IOP • Poor perfusion pressure to the ONH • Obstruction of axoplasmic flow within the ganglion cell axons • Anatomic weakening of the lamina cribrosa ▫ Myopia ▫ Optic nerve pits • Programmed cell death of the ganglion cell axons (apoptosis) Pre-perimetric glaucoma? 20-40% of ganglion cells are lost before VF defects are detected on standard automated perimetry So what? Assessment of the ONH is critical for early diagnosis and management to prevent VF defects before they occur Optic Nerve Head (ONH) • Careful evaluation of the ONH has high specificity and good precision for glaucoma diagnosis • It is one of the most important -

Congenital Anomalies of the Optic Nerve
Saudi Journal of Ophthalmology (2015) 29, 32–38 Neuro-ophthalmology Update Congenital anomalies of the optic nerve ⇑ Manuel J. Amador-Patarroyo, Mario A. Pérez-Rueda , Carlos H. Tellez Abstract Congenital optic nerve head anomalies are a group of structural malformations of the optic nerve head and surrounding tissues, which may cause congenital visual impairment and blindness. Each entity in this group of optic nerve anomalies has individually become more prevalent as our ability to differentiate between them has improved due to better characterization of cases. Access to better medical technology (e.g., neuroimaging and genetic analysis advances in recent years) has helped to expand our knowl- edge of these abnormalities. However, visual impairment may not be the only problem in these patients, some of these entities will be related to ophthalmologic, neurologic and systemic features that will help the physician to identify and predict possible out- comes in these patients, which sometimes may be life-threatening. Herein we present helpful hints, associations and management (when plausible) for them. Keywords: Coloboma, Congenital, Optic disc excavation, Systemic anomalies, Optic nerve malformations Ó 2014 Production and hosting by Elsevier B.V. on behalf of Saudi Ophthalmological Society, King Saud University. http://dx.doi.org/10.1016/j.sjopt.2014.09.011 Introduction However, visual impairment may not be the only problem in these patients, some of these entities will be related to oph- Congenital malformations of the optic nerve, especially thalmologic, neurologic and systemic features (especially those involving the optic nerve head and surrounding tissues, endocrinologic disturbances) that will help the physician to include a broad spectrum of malformations frequently associ- identify and predict possible outcomes in these patients, ated with congenital blindness or significant visual impair- which sometimes may be life-threatening.4–6 ment. -
Coexistence of Optic Pit and Coloboma of Iris, Lens, and Choroid
CASE REPORT Coexistence of optic pit and coloboma of iris, lens, and choroid: a case report Coexistência de fosseta óptica e coloboma de íris, cristalino e coroide: um primeiro relato de caso RAMAZAN ÖZELCE1, VUSLAT GÜRLÜ1, HANDE GÜÇLÜ1, Sadık ALTAN ÖZAL1 ABSTRACT RESUMO A 42-year-old woman was admitted to our clinic with a complaint of glare in both Uma mulher de 42 anos de idade foi internada em nossa clínica com queixa de ofus- eyes. Biomicroscopic examination of both the eyes revealed iris and lens colobomas camento em ambos os olhos. O exame biomicroscópico revelou coloboma de íris e in the inferior quadrant. Fundus examination of the right eye revealed an oval and cristalino no quadrante inferior em ambos os olhos. O exame de fundo do olho direito gray inferotemporal optic pit and two choroid colobomas in the inferior quadrant. revelou um fosseta óptica oval e acinzentada na região inferotemporal e dois colobomas In the left eye, two choroid colobomas were detected that were inferior to the coroide no quadrante inferior. No olho esquerdo, dois colobomas de coroide foram optic nerve head. Furthermore, a 21-year-old man presented to our clinic for a detectados inferiormente à da cabeça do nervo óptico. Outro homem de 21 anos routine ophthalmologic examination. Bilateral biomicroscopic examination was apresentou-se em nossa clínica para um exame oftalmológico de rotina. O exame normal. Fundus examination of the left eye revealed an oval and gray inferotem- bio microscópico foi normal, bilateralmente. O exame de fundo do olho esquerdo poral optic pit and a choroid coloboma that was inferior to the optic nerve head. -

Double Optic Discs, Optic Disc Coloboma, And
Figure 2. Optical coherence tomographic image of the right eye Figure 3. Microperimetry of the right eye with a scanning laser corresponding to the scan line indicated by the arrow. Some of the outer ophthalmoscope. (size, Goldmann I; brightness, −15 dB; background, 10 retinal layers other than the nerve fiber layer appear to be absent in the areas candelas/m2). The patient did not recognize the stimulus at the positions of the cleavages. indicated by the red P s. profile of the inner retinal cleavages never see small bundles of nerve fi- (Figure 2). The mean±SD thick- ber passing across the RNFL de- Double Optic Discs, Optic ness of the retina at the site of the fect. However, there should be many Disc Coloboma, and Pit: cleavages was 106.4±17.7 m and that cases in which we cannot make a Spectrum of Hybrid Disc of the adjacent unaffected retina was clear distinction between them just Anomalies in a Single Eye 254.2±25.8 m. The mean thickness by fundoscopic appearance. Opti- of the retina at the site of the cleav- cal coherence tomographic imag- ages was significantly thinner than ing should be very useful in such Doubling of the optic disc is rare and that of the adjacent unaffected retina cases in making a correct diagnosis. is seen as true doubling or pseudo- (PϽ.001, Mann-Whitney U test). The The optical coherence tomo- doubling. We describe a peculiar case with multiple anomalies involv- fluorescein angiograms showed no graphic images showed the cleav- ing a single optic disc: a coloboma abnormalities.