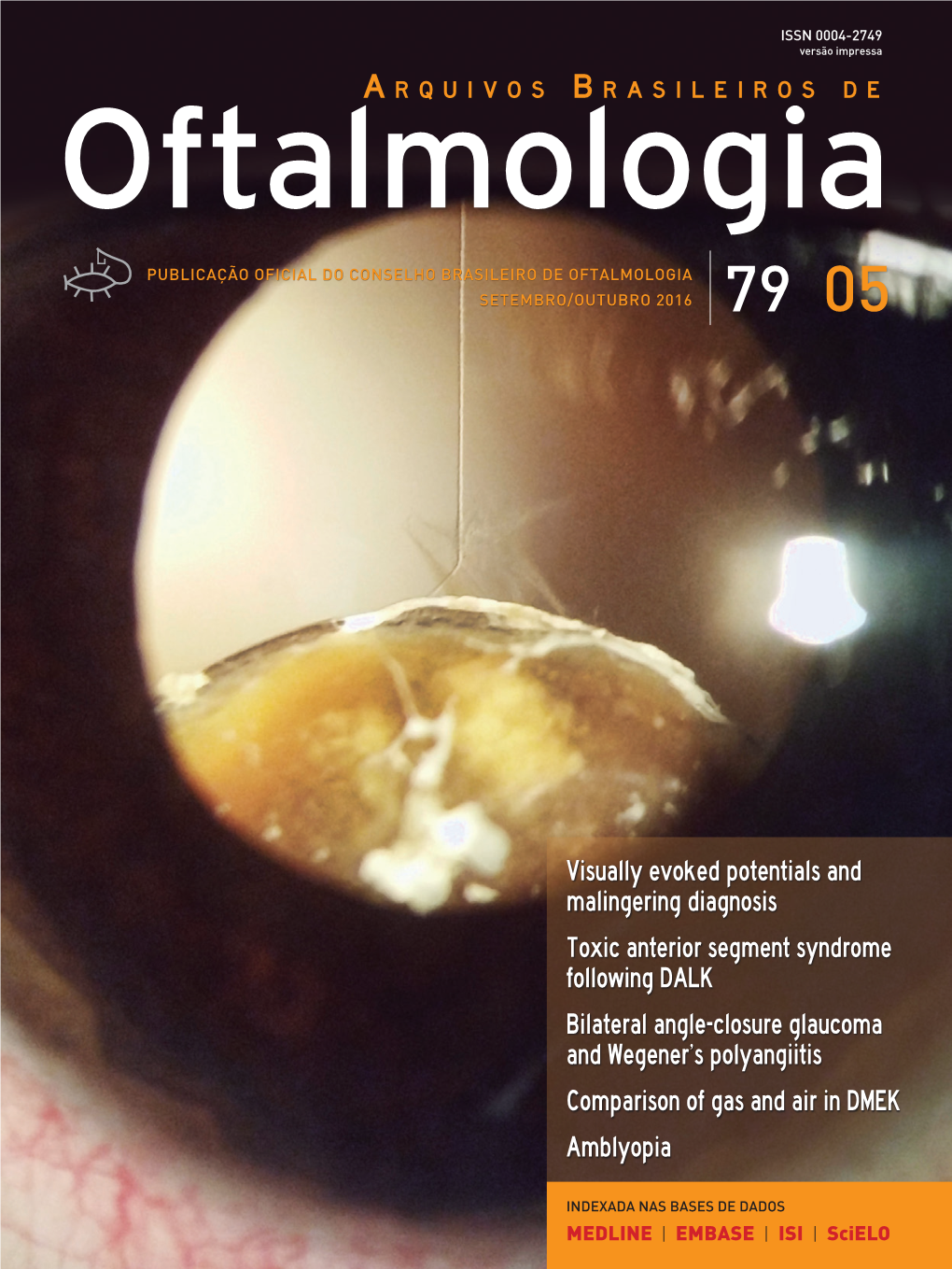
Visually Evoked Potentials and Malingering Diagnosis Toxic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

What Does the Dominant Eye Dominate? a Brief and Somewhat Contentious Review
Perception & Psychophysics 2003, 65 (2), 310-317 What does the dominant eye dominate? A brief and somewhat contentious review ALISTAIR P. MAPP, HIROSHI ONO, and RAPHAEL BARBEITO York University, Toronto, Ontario, Canada We examine a set of implicit and explicit claims about the concept of eye dominance that have been made over the years and note that the new literature on eye dominance does not reflect the old litera- ture from the first half of the last century. We argue that the visual and oculomotor function of the dom- inant eye—defined by such criteria as asymmetry in acuity, rivalry, or sighting—remains unknown and that the usefulness of the concept for understanding its function is yet to be determined. We suggest that the sighting-dominant eye is the eye used for monocular tasks and has no unique functional role in vision. Interest in eye dominance has a long and rich history. Coren and Kaplan’sfinding discussed in Claim 2, below. Coren and Porac (1975) published an annotated bibliog- The three defining criteria are raphy of 235 articles on this topic. Their search began with (a) the eye with better visual acuity, contrast sensitivity, the original article on eye dominanceby Porta (1593) and or other measure of visual functioning . ., (b) the eye in extended to 1975. Recently, we searched the 1975–2002 which a rivalingstimulusis most often dominant,and (c) the PsychINFO database and found an additional 340 arti- eye used for sighting when, for instance, one looks at a cles. (This paper is not intended to be a review of the en- distant object through a ring held in both hands at arm’s tire ocular dominance literature. -

Role of Primary Care Optometrists in the Assessment and Management of Patients with Traumatic Brain Injuries in Canada
CANADIAN JOURNAL of OPTOMETRY | REVUE CANADIENNE D’OPTOMÉTRIE EST. 1939 VOLUME 80 NUMBER 1 CLINICAL RESEARCH Role of Primary Care Optometrists in the Assessment and Management of Patients with Traumatic Brain Injuries in Canada CLINICAL RESEARCH INNOVATIONS PRACTICE MANAGEMENT Pituitary Tumor Associated The Model T Trends in Health Professions: with Situs Inversus of and a Peek Behind Disclosure of Records the Optic Nerve Head the Curtain? to Third Parties Publications Mail Agreement No. 40063055 CANADIAN JOURNAL of OPTOMETRY REVUE CANADIENNE D’OPTOMÉTRIE Vol 80, No 1 CANADIAN JOURNAL of OPTOMETRY | REVUE CANADIENNE D’OPTOMÉTRIE Spring/Printemps 2018 EST. 1939 VOLUME 80 NUMBER 1 ISSN 0045-5075 The Canadian Journal of Optometry is the official CONTENTS publication of the Canadian Association of EDITORIAL/ÉDITORIAL Optometrists (CAO) / La Revue canadienne 5 Stanley Woo, OD, MS, MBA, FAAO, Director d’optométrie est la publication officielle de 9 Stanley Woo, D.O., M.Sc., M.B.A., F.A.A.O., Directeur l’Association canadienne des optométristes (ACO) : 234 Argyle Avenue, Ottawa ON, K2P 1B9. Phone 613 C CLINICAL RESEARCH 235-7924 / 888 263-4676, fax 613 235-2025, e-mail [email protected], website www.opto.ca. Publications RESEARCH/RECHERCHE Mail Registration No. 558206 / Envoi de publication 13 – Enregistrement no 558206. Role of Primary Care Optometrists in the Assessment and The Canadian Journal of Optometry / La Revue Management of Patients with Traumatic Brain Injuries in Canada canadienne d’optométrie (USPS#0009-364) is Zoe Lacroix, O.D., Susan J. Leat, PhD, FCOptom, F.A.A.O., published four times per year. Lisa W. -

Effect of Interaction Between Eye-Hand Dominance on Dart Skill
Journal of Neuroscience and Behavioural Health Vol. 4(2), pp. 6-12, February 2012 Available online at http://www.academicjournals.org/JNBH DOI:10.5897/JNBH11.027 ISSN 2141-2286 ©2012 Academic Journals Full Length Research Paper Effect of interaction between eye-hand dominance on dart skill Rahil Razeghi, Parvaneh Shafie Nia, Nahid Shebab bushehri and Farzad Maleki* Department of Sport Psychology, Faculty of Physical Education and Sport Science, Shahid Chamran University of Ahvaz, Iran. Accepted 9 November, 2011 The purpose of this research was surveying the effect of interaction between eye hand dominance on dart skill. Twenty healthy male subjects (age: 21.43±1.33) from University of Shahid Chamran were served as the participants for this study. Subjects were divided into two groups: unilateral (right eye and right hand or left eye and left hand) group (10 subjects) and cross lateral (right eye and left hand or left eye and right hand) group (10 subjects). Each group trained for 12 sessions in the same condition. The acquisition test was made after the last training session and the retention test was made 1 week later. The scores of pre-test, acquisition and retention were recorded. Subjects threw 60 darts in each training session. Porta (Roth, 2002) and Hole in the card test (Sage, 1984) was used to select eye dominance and Edinburgh questionnaire (Oldfield, 1971) was used to determine handedness. Values of p<0.05 were chosen as significant. The results of dependent t-test (paired t-test) analysis showed that there was a significant difference between the pre-test, acquisition and retention between two groups that showed both groups learn dart skill. -

Increased Prevalence of Left-Handedness in Hemifacial Microsomia
ORIGINAL ARTICLE Increased Prevalence of Left-Handedness in Hemifacial Microsomia Gary F. Rogers, MD, JD, MBA, MPH,* Stephen R. Sullivan, MD,* John B. Mulliken, MD,* Arin K. Greene, MD, MMSc,* and Albert K. Oh, MDÞ he body plan for humans is essentially symmetric around the Abstract: Ten percent of people are left handed, but a higher Tmidaxis. Nevertheless, asymmetric arrangement of organs in the frequency has been associated with certain craniofacial malforma- thoracoabdominal cavities indicates that cellular functions become tions, such as cleft lip and unilateral coronal synostosis. The purpose unequal early in development. Cellular symmetry persists through- of this study was to determine the frequency of left-handedness in out the gastrula stage and, thereafter, differential cascades of gene patients with hemifacial microsomia (HFM). Patients with HFM expression break the otherwise symmetrical internal structure.1 were identified in our craniofacial database. Normal controls were Animal models have provided some insight into the molecular and recruited by local pediatricians. Data gathered included age, sex, developmental mechanisms by which right-left symmetry is 1,2 and handedness (determined by writing and/or drawing); the orbit, altered. Nevertheless, investigators are still unclear why these mandible, ear, nerve, and soft tissue (OMENS)Yplus score and side structural asymmetries occur in a nonrandom, or unequal, distribu- tion. Nonrandom laterality is seen in the human brain, face, heart, of involvement were tabulated for patients with HFM. Hand pre- 2 great vessels, lungs, liver, gallbladder, biliary tract, gastrointestinal ference was compared between the groups using # analysis; pos- tract, spleen, and male genitalia.3,4 All but 0.01% of humans exhibit sible correlations were analyzed between handedness and age, the same asymmetric arrangement of their internal organs (situs or sex, the OMENS score, extracraniofacial findings, and side of in- situs solitus).5,6 Nevertheless, in extremely rare instances, the volvement. -

Handedness of a Motor Program in C. Elegans Is Independent of Left-Right Body Asymmetry
Handedness of a Motor Program in C. elegans Is Independent of Left-Right Body Asymmetry Joanna C. Downes¤, Bilge Birsoy, Kyle C. Chipman, Joel H. Rothman* Department of Molecular, Cellular and Developmental Biology and Neuroscience Research Institute, University of California Santa Barbara, Santa Barbara, California, United States of America Abstract Complex animals display bilaterally asymmetric motor behavior, or ‘‘motor handedness,’’ often revealed by preferential use of limbs on one side. For example, use of right limbs is dominant in a strong majority of humans. While the mechanisms that establish bilateral asymmetry in motor function are unknown in humans, they appear to be distinct from those for other handedness asymmetries, including bilateral visceral organ asymmetry, brain laterality, and ocular dominance. We report here that a simple, genetically homogeneous animal comprised of only ,1000 somatic cells, the nematode C. elegans, also shows a distinct motor handedness preference: on a population basis, males show a pronounced right-hand turning bias during mating. The handedness bias persists through much of adult lifespan, suggesting that, as in more complex animals, it is an intrinsic trait of each individual, which can differ from the population mean. Our observations imply that the laterality of motor handedness preference in C. elegans is driven by epigenetic factors rather than by genetic variation. The preference for right-hand turns is also seen in animals with mirror-reversed anatomical handedness and is not attributable to stochastic asymmetric loss of male sensory rays that occurs by programmed cell death. As with C. elegans, we also observed a substantial handedness bias, though not necessarily the same preference in direction, in several gonochoristic Caenorhabditis species. -

How Ocular Dominance and Binocularity Are Reflected by the Population Receptive Field Properties
Visual Neuroscience How Ocular Dominance and Binocularity Are Reflected by the Population Receptive Field Properties Pieter B. de Best,1 Noa Raz,1 Serge O. Dumoulin,2 and Netta Levin1 1fMRI lab, Neurology Department, Hadassah Hebrew University Medical Center Jerusalem, Israel 2Spinoza Centre for Neuroimaging, Amsterdam, The Netherlands Correspondence: Netta Levin, fMRI PURPOSE. The neural substrate of binocularity and sighting ocular dominance in humans is not Unit, Neurology Department, Hadas- clear. By utilizing the population receptive field (pRF) modeling technique, we explored sah Hebrew University Medical Cen- whether these phenomena are associated with amplitude and pRF size differences. ter, POB 12,000, Jerusalem 91120, Israel; METHODS. The visual field maps of 13 subjects were scanned (3-T Skyra) while viewing drifting [email protected]. bar stimuli. Both eyes (binocular condition), the dominant eye and the nondominant eye (two Submitted: March 5, 2018 monocular conditions) were stimulated in separate sessions. For each condition, pRF size and Accepted: October 1, 2018 amplitude were assessed. Binocular summation ratios were calculated by dividing binocular by mean monocular values (amplitude and pRF size). Citation: de Best PB, Raz N, Dumoulin S, Levin N. How ocular dominance RESULTS. No differences in pRF size were seen between the viewing conditions within each and binocularity are reflected by the region, that is, either between binocular and monocular or between dominant and population receptive field properties. nondominant viewing conditions. Binocular amplitudes were higher than the monocular Invest Ophthalmol Vis Sci. amplitudes, but similar among the dominant and nondominant eyes. Binocular summation 2018;59:5301–5311. https://doi.org/ ratios derived from amplitudes were significantly higher than one (~1.2), while those ratios 10.1167/iovs.18-24161 derived from pRF size were not. -

DOMENT RESLNE ED 033 018 24 RE 002 287 By-Boos
)j DOMENT RESLNE ED 033 018 24 RE 002 287 By-Boos. Robert-W.; Hillerich. Robert L.- A Study of the Possible Distinction Between 'Controlling Eye' and 'Dominant Eye' and the Effect of Both. with Hand Dominance. on Reading Achievement. Community Consolidated School District 34. Glenview. III. Spons Agency-Office of Education (DHEW). Washington. DC. Bureau of Research. Bureau No-BR -7 -E -046 Pub Date Nov 67 Grant -0EC -3 -7 -700046.2896 Note -61 p. EDRS Price ME -$0.50 HC -S3.15 Descriptors -*Eye Hand Coordination. Grade 7. Grade 8. Lateral Dominance. Longitudinal Studies. Perceptual Motor Coordination. *Reading Achievement. Reading Difficulty. Reading Research This longitudinal study was a replication of two disparate studies.one of dominance and one of control. which had as subjects 277 seventh- and eighth-grade pupils remaining from an original dominance study of over 500. Eye dominancewas determined through hole-in-paper and V-scope; eye control at near and far point. through the telebinocular; hand dominance. through tapping. connecting dots. and a variety of performed acts; reading achievement. through the California Achievement Test; and reading differential. through a formula utilizing IQ's from the California Test of Mental Maturity. While controlling eye and dominanteye were found to be unrelated to each other. no significant difference was observed in reading achievement or reading differential regardless of the dominance or controc characteristics of the subjects. A strong tendency was observed for subjectso exhibit more mixed dominance at eight grade than they had at grade 2. Finally. observingno significant difference in dominance patterns of male as compared with female subjects. -

Disease Laterality, Eye Dominance, and Visual Handicap in Patients with Unilateral Full Thickness Macular Holes K Waheed,Dahlaidlaw
626 CLINICAL SCIENCE Br J Ophthalmol: first published as 10.1136/bjo.87.5.626 on 1 May 2003. Downloaded from Disease laterality, eye dominance, and visual handicap in patients with unilateral full thickness macular holes K Waheed,DAHLaidlaw ............................................................................................................................. Br J Ophthalmol 2003;87:626–628 Aim: To investigate the association between visual handicap, laterality, and historical eye dominance in patients presenting with unilateral full thickness macular holes (FTMH). Methods: Consecutive patients presenting with unilateral FTMH and no other visually significant ocu- See end of article for lar pathology including abnormalities of binocular vision were included. A questionnaire and case note authors’ affiliations review were performed to determine the mode of presentation, presence of symptomatic binocular ....................... interference, historically dominant eye, and whether they elected to undergo surgery. Correspondence to: Results: 44 eyes of 44 patients fulfilled the inclusion criteria. 21 (48%) affected eyes were right sided MrDAHLaidlaw,Vitreo and 56% of FTMH were in the historically dominant eye. 76% of FTMH in historically dominant eyes Retinal Unit, 9th Floor, presented symptomatically compared to 36% in non-dominant eyes (p= 0.003). 72% of patients with North Wing, St Thomas’s Hospital, London SE1 7EH, FTMH affecting their historically dominant eye were aware of binocular interference in day to day bin- UK; ocular viewing compared with 21% when the FTMH was in the non-dominant eye (p= 0.001). 23 [email protected] (52%) patients elected to undergo surgery, of whom 18/23(78%) had FTMH in their historically domi- Accepted for publication nant eye (p= 0.0003). 20 May 2002 Conclusion: This study suggests that eye dominance may be an important determinant of the visual ...................... -

A Study in the Comparison of Ocular and Extremity Dominance Among a Stuttering and Non-Stuttering School-Age Population Bruce Frank Brantingham
Loma Linda University TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works Loma Linda University Electronic Theses, Dissertations & Projects 8-1968 A Study in the Comparison of Ocular and Extremity Dominance Among a Stuttering and Non-Stuttering School-Age Population Bruce Frank Brantingham Follow this and additional works at: https://scholarsrepository.llu.edu/etd Part of the Speech Pathology and Audiology Commons Recommended Citation Brantingham, Bruce Frank, "A Study in the Comparison of Ocular and Extremity Dominance Among a Stuttering and Non-Stuttering School-Age Population" (1968). Loma Linda University Electronic Theses, Dissertations & Projects. 552. https://scholarsrepository.llu.edu/etd/552 This Thesis is brought to you for free and open access by TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works. It has been accepted for inclusion in Loma Linda University Electronic Theses, Dissertations & Projects by an authorized administrator of TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works. For more information, please contact [email protected]. LOMA LINDA UNIVERSITY Graduate School A Study in the Comparison of Ocular and Extremity Dominance. Iunong l\ Stuttering and Non-Stutterin~J School-age Population by Bruce E'rank Brantingham A Thesis in Partial D'ulf illment of the Requirements For the Degree Master of Science In The Field of Speech Pati'1ology and Audiology August 1968 155243 Each person whose signature appears below certifies that he has read this thesis and that in his opinion it is adequate, in scope and quality, as a thesis for the degree of Master of Science. , Chairman ., Professor m~f-~ 1~~"'cJ~9? w. Fletcher Tarr, Ph.D., Professor of Speech, Chairman, Department of Speech ~~~,-- (/ L~arburton Miller, Ph.D., Lecturer in Speech Pathology ~>;~_/ .Mo;J:;r, M.A. -

The Effects of Ocular Dominance on Visual Processing in College Students William A
James Madison University JMU Scholarly Commons Senior Honors Projects, 2010-current Honors College Summer 2017 The effects of ocular dominance on visual processing in college students William A. Holland James Madison University Follow this and additional works at: https://commons.lib.jmu.edu/honors201019 Part of the Behavioral Neurobiology Commons, and the Cognitive Neuroscience Commons Recommended Citation Holland, William A., "The effects of ocular dominance on visual processing in college students" (2017). Senior Honors Projects, 2010-current. 294. https://commons.lib.jmu.edu/honors201019/294 This Thesis is brought to you for free and open access by the Honors College at JMU Scholarly Commons. It has been accepted for inclusion in Senior Honors Projects, 2010-current by an authorized administrator of JMU Scholarly Commons. For more information, please contact [email protected]. The Effects of Ocular Dominance on Visual Processing in College Students _______________________ An Honors College Project Presented to the Faculty of the Undergraduate College of Science and Mathematics James Madison University _______________________ by William Alexander Holland May 2017 Accepted by the faculty of the Department of Biology, James Madison University, in partial fulfillment of the requirements for the Honors College. FACULTY COMMITTEE: HONORS COLLEGE APPROVAL: Project Advisor: Corey L. Cleland, Ph.D., Bradley R. Newcomer, Ph.D., Associate Professor, Biology Dean, Honors College Reader: James S. Sochacki, Ph.D., Professor, Mathematics Reader: Roger Thelwell, Ph.D., Associate Professor, Mathematics PUBLIC PRESENTATION This work is accepted for presentation, in part or in full, at [venue] The Honors Symposium on [date] 4/21/17 . II. Table of Contents I. Title page …………………………………………………………………………....1 II. -

Ocular Dominance and Handedness in Golf Putting
Ocular Dominance and Handedness in Golf Putting Appendix 1: Overview of Historical Ocular Dominance Research Roughly 60% of the population has been shown to be right handed, 30% left handed and 10% ambidextrous;1-5 similarly approximately 67% of the population has been shown to have right eye dominance.6 Originally, researchers thought that ocular dominance was related to handedness or foot dominance, especially as in both handedness and ocular dominance, there seems to be a strong predisposition towards favouring the right side of the body. Researchers have now agreed that while handedness and foot dominance have been found to be highly correlated with each other, they are neither indicative nor predictive of ocular dominance.7-10 Hand and foot dominance are thought to be related to the dominance of one cerebral hemisphere in the brain, but ocular dominance cannot be created in this way. A semi- decussation of optic nerve fibres at the optic chiasm means that visual information from the right and left eyes are represented in both hemispheres.7-9 Despite a vast amount of time and effort that has been invested in understanding the physiological basis of ocular dominance and its functional roles, little agreement between researchers has been reached. Mapp et al. went so far as to suggest that the dominant eye determined by sighting ocular dominance tests, whereby the observer is asked to align a near target with a distant target, only exists because of the sighting dominance tests are designed so that only one eye may be used or because of the ease or the habit of using a particular eye for such tasks.11 On the other hand, Valle-Inclan et al. -
Ocular Sensory Dominance and Viewing Distance Karen Squier Nova Southeastern University
Nova Southeastern University NSUWorks College of Optometry Student Theses, Dissertations College of Optometry and Capstones 1-1-2017 Ocular sensory dominance and viewing distance Karen Squier Nova Southeastern University This document is a product of extensive research conducted at the Nova Southeastern University College of Optometry. For more information on research and degree programs at the NSU College of Optometry, please click here. Follow this and additional works at: https://nsuworks.nova.edu/hpd_opt_stuetd Part of the Optometry Commons All rights reserved. This publication is intended for use solely by faculty, students, and staff of oN va Southeastern University. No part of this publication may be reproduced, distributed, or transmitted in any form or by any means, now known or later developed, including but not limited to photocopying, recording, or other electronic or mechanical methods, without the prior written permission of the author or the publisher. NSUWorks Citation Karen Squier. 2017. Ocular sensory dominance and viewing distance. Master's thesis. Nova Southeastern University. Retrieved from NSUWorks, College of Optometry. (12) https://nsuworks.nova.edu/hpd_opt_stuetd/12. This Thesis is brought to you by the College of Optometry at NSUWorks. It has been accepted for inclusion in College of Optometry Student Theses, Dissertations and Capstones by an authorized administrator of NSUWorks. For more information, please contact [email protected]. Ocular sensory dominance and viewing distance Karen Squier, OD, F.A.A.O. Submitted to the Clinical Vision Research Program, College of Optometry of Nova Southeastern University in partial fulfillment of the requirements for the degree of Master of Science in Clinical Vision Research Written under the direction of Bin Zhang, M.D., Ph.