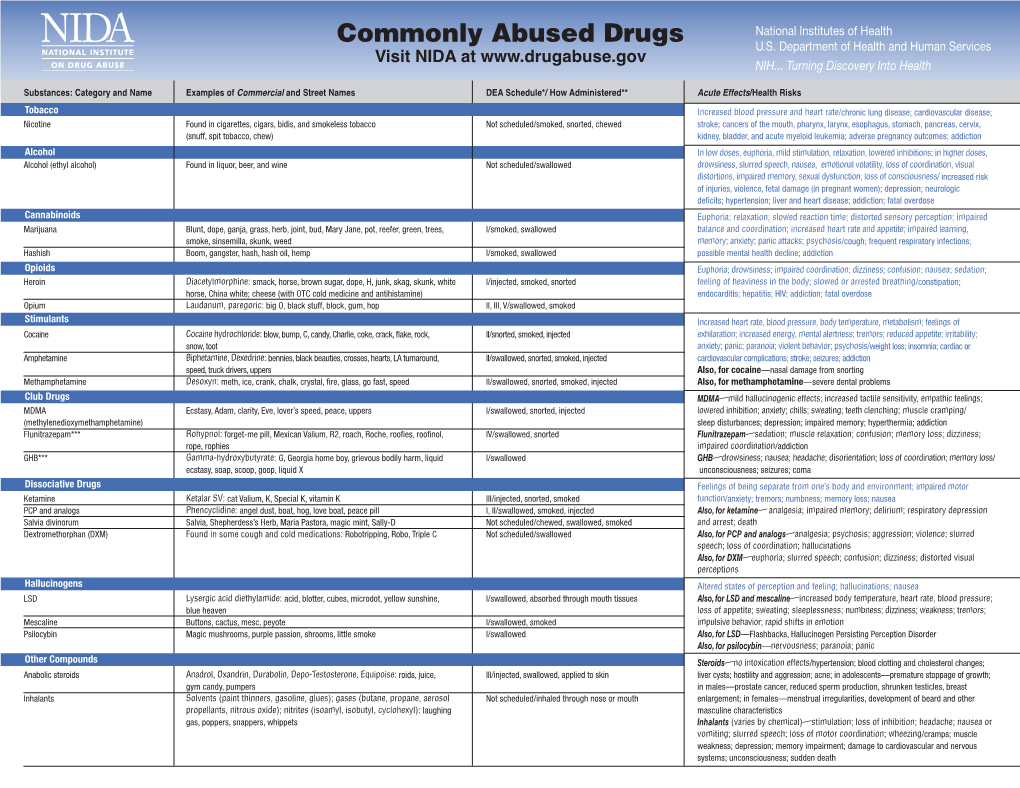
Commonly Abused Drugs Chart
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Drug Prohibition and the Weakness of Public Policy
Georgetown University Law Center Scholarship @ GEORGETOWN LAW 1994 Bad Trip: Drug Prohibition and the Weakness of Public Policy Randy E. Barnett Georgetown University Law Center, [email protected] This paper can be downloaded free of charge from: https://scholarship.law.georgetown.edu/facpub/1252 103 Yale L.J. 2593-2630 (1994) (reviewing Steven B. Duke & Albert C. Gross, AMERICA'S LONGEST WAR: RETHINKING OUR TRAGIC CRUSADE AGAINST DRUGS (1993)) This open-access article is brought to you by the Georgetown Law Library. Posted with permission of the author. Follow this and additional works at: https://scholarship.law.georgetown.edu/facpub Part of the Criminal Law Commons, Legislation Commons, and the Public Policy Commons Book Review Bad Trip: Drug Prohibition and the Weakness of Public Policy America's Longest War: Rethinking Our Tragic Crusade Against Drugs. By Steven B. Duke & Albert C. Gross. New York: G.P. Putnam's Sons, 1993. Pp. xix, 348. $26.95. Randy E. Barnettt INTRODUCTION Popular support for drug prohibition-especially among those who have given the matter any thought-is like support for George Bush just after Operation Desert Storm: very broad and very thin. Perhaps some personal experiences of mine will illustrate why. Personal Anecdote Number One: In the early morning hours of February 24, 1979, Michael Salcedo, his brother Arthur, and their friend Frank Mussa decided to buy some marijuana. Because marijuana is illegal, they could not go to the same legitimate businesses that sell tobacco or alcohol. So the three young men set out for Latin Eagles territory on the north side of Chicago; specifically to King Kastle, a hamburger stand that gang members were known t Professor of Law, Boston University School of Law. -

Palliative Care Case of the Month
PALLIATIVE CARE CASE OF THE MONTH “Treating Non-Infectious Diarrhea” by Robert Arnold, MD Volume 19, No. 98 August, 2019 Case 1: Mr. Jones is a 58-year-old man with short gut Three drugs are used because of their ability to slow down the syndrome. Palliative Care was consulted for goals of care, gut, allowing for more time for absorption of intestinal fluids a however quickly it became clear uncontrolled diarrhea was a decrease of diarrhea. The most well-know is loperamide, a larger priority. He said having to change the bag every few hours synthetic opiate which has minimal absorption. The dosing is 4 completely interfered with his living a normal life. He said, “I’d mg after one’s first bowel movement and then 2 mg after every rather die than have all of this diarrhea.” unformed stool, up to 16 mg (in palliative care patients there is some data for use up to 54 mg).9, 10 Loperamide should be Case 2: A 62-year-old woman with non-small cell lung cancer continued for 12 hours after diarrhea is stopped. Adverse effects is receiving immunotherapy. She has done quite well but is include mostly constipation, abdominal cramps, nausea and distressed by her diarrhea. She tried Lomotil and Imodium but rarely CNS effects like fatigue or dizziness. Cases of torsades de neither worked. When seeing her palliative care doctor, she said, pointes and death have been reported with higher than “It isn’t worth treating my cancer if I can’t live a normal life.” 9 recommended doses. -

Guidelines for the Forensic Analysis of Drugs Facilitating Sexual Assault and Other Criminal Acts
Vienna International Centre, PO Box 500, 1400 Vienna, Austria Tel.: (+43-1) 26060-0, Fax: (+43-1) 26060-5866, www.unodc.org Guidelines for the Forensic analysis of drugs facilitating sexual assault and other criminal acts United Nations publication Printed in Austria ST/NAR/45 *1186331*V.11-86331—December 2011 —300 Photo credits: UNODC Photo Library, iStock.com/Abel Mitja Varela Laboratory and Scientific Section UNITED NATIONS OFFICE ON DRUGS AND CRIME Vienna Guidelines for the forensic analysis of drugs facilitating sexual assault and other criminal acts UNITED NATIONS New York, 2011 ST/NAR/45 © United Nations, December 2011. All rights reserved. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. This publication has not been formally edited. Publishing production: English, Publishing and Library Section, United Nations Office at Vienna. List of abbreviations . v Acknowledgements .......................................... vii 1. Introduction............................................. 1 1.1. Background ........................................ 1 1.2. Purpose and scope of the manual ...................... 2 2. Investigative and analytical challenges ....................... 5 3 Evidence collection ...................................... 9 3.1. Evidence collection kits .............................. 9 3.2. Sample transfer and storage........................... 10 3.3. Biological samples and sampling ...................... 11 3.4. Other samples ...................................... 12 4. Analytical considerations .................................. 13 4.1. Substances encountered in DFSA and other DFC cases .... 13 4.2. Procedures and analytical strategy...................... 14 4.3. Analytical methodology .............................. 15 4.4. -
Anti-Diarrheal Activity and Brine Shrimp Lethality Bioassay of Methanolic Extract of Cordyline Fruticosa (L.) A
Naher et al. Clinical Phytoscience (2019) 5:15 https://doi.org/10.1186/s40816-019-0109-z ORIGINAL CONTRIBUTION Open Access Anti-diarrheal activity and brine shrimp lethality bioassay of methanolic extract of Cordyline fruticosa (L.) A. Chev. leaves Sharmin Naher1*, Md. Abdullah Aziz1, Mst. Irin Akter2, S. M. Mushiur Rahman1, Sadiur Rahman Sajon1 and Kishor Mazumder1,3 Abstract Background: Cordyline fruticosa (L.) A. Chev. (Asparagaceae) is a plant which is traditionally used for the treatment of cough, bloody cough, diarrhea, dysentery, high fever, difficulties in urine, bloody urine, small pox, madness, skin eruptions, joint pains, rheumatic bone pains, sore throat, neck pain, bleeding hemorrhoids and inflammation in the digestive tract. Therefore, the present work aims to investigate the antidiarrheal and cytotoxic activities of methanolic extract of Cordyline fruticosa leaves in mice and brine shrimp, respectively. Methods: The effects of the methanol extract of Cordyline fruticosa leaves (MCFL) on castor oil-induced diarrhea, magnesium sulphate induced diarrhea and charcoal meal test in mice were investigated. In addition, brine shrimp lethality bioassay method was used to evaluate cytotoxic activity of MCFL. Results: In castor oil induced diarrheal test, MCFL at the dose of 200, 400 and 800 mg/kg body weight significantly (∗P< 0.05, versus control) and dose-dependently reduced the frequency of diarrhea. The frequency of magnesium sulphate-induced diarrhea was significantly reduced by MCFL at the dose of with 800 mg/kg. In the charcoal meal test, the extract at the dose of 400 and 800 mg/kg body weight significantly (∗P< 0.05) reduced the distance travelled by charcoal along the intestinal tract when compare with control. -

Ecstasy Or Molly (MDMA) (Canadian Drug Summary)
www.ccsa.ca • www.ccdus.ca November 2017 Canadian Drug Summary Ecstasy or Molly (MDMA) Key Points Ecstasy and molly are street names for pills or tablets that are assumed to contain the active ingredient 3,4-methylenedioxy-N-methamphetamine (MDMA). Although most people consuming ecstasy or molly expect the main psychoactive ingredient to be MDMA, pills, capsules and powder sold as ecstasy or molly frequently contain other ingredients (such as synthetic cathinones or other adulterants) in addition to MDMA and sometimes contain no MDMA at all. The prevalence of Canadians aged 15 and older reporting past-year ecstasy use is less than 1%. 1 in 25 Canadian youth in grades 10–12 have reported using ecstasy in the past 12 months. Introduction Ecstasy and molly are street names for pills, capsules or powder assumed to contain MDMA (3,4- methylenedioxy-N-methamphetamine), a synthetically derived chemical that is used recreationally as a party drug. Pills are typically coloured and stamped with a logo. These drugs are made in illegal laboratories, often with a number of different chemicals, so they might not contain MDMA or contain MDMA in amounts that vary significantly from batch to batch. Other active ingredients found in tablets sold as ecstasy or molly in Canada in 2016–2017 include synthetic cathinones or “bath salts” such as ethylone, methylenedioxyamphetamine (MDA) and its precursor methylenedioxyphenylpropionamide (MMDPPA). Other adulterants reported were caffeine, procaine, methylsulfonylmethane (MSA)and methamphetamine.1 In 2011–2012, paramethoxymethamphetamine (PMMA) was present in pills sold as ecstasy in Canada. This adulteration resulted in the deaths of 27 individuals in Alberta and British Columbia over an 11-month period.2 Effects of Ecstasy Use The effects of ecstasy are directly linked to the active ingredients in the pill. -

Benzodiazepines: Uses and Risks Charlie Reznikoff, MD Hennepin Healthcare
Benzodiazepines: Uses and Risks Charlie Reznikoff, MD Hennepin healthcare 4/22/2020 Overview benzodiazepines • Examples of benzos and benzo like drugs • Indications for benzos • Pharmacology of benzos • Side effects and contraindications • Benzo withdrawal • Benzo tapers 12/06/2018 Sedative/Hypnotics • Benzodiazepines • Alcohol • Z-drugs (Benzo-like sleeping aids) • Barbiturates • GHB • Propofol • Some inhalants • Gabapentin? Pregabalin? 12/06/2018 Examples of benzodiazepines • Midazolam (Versed) • Triazolam (Halcion) • Alprazolam (Xanax) • Lorazepam (Ativan) • Temazepam (Restoril) • Oxazepam (Serax) • Clonazepam (Klonopin) • Diazepam (Valium) • Chlordiazepoxide (Librium) 4/22/2020 Sedatives: gaba stimulating drugs have incomplete “cross tolerance” 12/06/2018 Effects from sedative (Benzo) use • Euphoria/bliss • Suppresses seizures • Amnesia • Muscle relaxation • Clumsiness, visio-spatial impairment • Sleep inducing • Respiratory suppression • Anxiolysis/disinhibition 12/06/2018 Tolerance to benzo effects? • Effects quickly diminish with repeated use (weeks) • Euphoria/bliss • Suppresses seizures • Effects incompletely diminish with repeated use • Amnesia • Muscle relaxation • Clumsiness, visio-spatial impairment • Seep inducing • Durable effects with repeated use • Respiratory suppression • Anxiolysis/disinhibition 12/06/2018 If you understand this pharmacology you can figure out the rest... • Potency • 1 mg diazepam <<< 1 mg alprazolam • Duration of action • Half life differences • Onset of action • Euphoria, clinical utility in acute -

Medications to Treat Opioid Use Disorder Research Report
Research Report Revised Junio 2018 Medications to Treat Opioid Use Disorder Research Report Table of Contents Medications to Treat Opioid Use Disorder Research Report Overview How do medications to treat opioid use disorder work? How effective are medications to treat opioid use disorder? What are misconceptions about maintenance treatment? What is the treatment need versus the diversion risk for opioid use disorder treatment? What is the impact of medication for opioid use disorder treatment on HIV/HCV outcomes? How is opioid use disorder treated in the criminal justice system? Is medication to treat opioid use disorder available in the military? What treatment is available for pregnant mothers and their babies? How much does opioid treatment cost? Is naloxone accessible? References Page 1 Medications to Treat Opioid Use Disorder Research Report Discusses effective medications used to treat opioid use disorders: methadone, buprenorphine, and naltrexone. Overview An estimated 1.4 million people in the United States had a substance use disorder related to prescription opioids in 2019.1 However, only a fraction of people with prescription opioid use disorders receive tailored treatment (22 percent in 2019).1 Overdose deaths involving prescription opioids more than quadrupled from 1999 through 2016 followed by significant declines reported in both 2018 and 2019.2,3 Besides overdose, consequences of the opioid crisis include a rising incidence of infants born dependent on opioids because their mothers used these substances during pregnancy4,5 and increased spread of infectious diseases, including HIV and hepatitis C (HCV), as was seen in 2015 in southern Indiana.6 Effective prevention and treatment strategies exist for opioid misuse and use disorder but are highly underutilized across the United States. -

Managing Anxiety Through Childhood Social-Emotional
MANAGING ANXIETY THROUGH CHILDHOOD SOCIAL-EMOTIONAL DEVELOPMENT by Adriane Hannah Dohl B.A., The University of British Columbia, 2008 A THESIS SUBMITTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF ARTS in THE FACULTY OF GRADUATE AND POSTDOCTORAL STUDIES (School Psychology) THE UNIVERSITY OF BRITISH COLUMBIA (Vancouver) October 2013 © Adriane Hannah Dohl, 2013 Abstract School professionals are implementing a universal social-emotional learning program for children in Kindergarten and Grade 1 (aged 4-6 years) in many schools across the province with training and funding provided by the government. The Fun FRIENDS (Barrett, 2007) program focuses on increasing social-emotional learning and promotes coping techniques and resiliency in order to prevent the onset of behavioural and emotional disorders (Pahl & Barrett, 2007). Preliminary results (Pahl & Barrett, 2007, 2010) have highlighted the effectiveness of the Fun FRIENDS program in reducing anxiety in children. The present study utilized a quasi-experimental design to evaluate the effectiveness of the Fun FRIENDS program in reducing anxiety and promoting social-emotional competence among a sample of Kindergarten and Grade 1 students (N = 33) in a British Columbia school district. Results revealed a significant decrease in program participants’ anxiety symptoms as rated by teachers when compared with those in the control group. Teachers also reported that children who participated in the program had significant increases in social-emotional skills, while those in the control group’s skills remained the same. However, overall, children in the control group had significantly higher social-emotional skills, as rated by teachers. No significant results were found for parent rated levels of anxiety or social-emotional skills of children enrolled in either condition. -

Social Emotional Learning Through Depression Education in a High School Setting
Illinois State University ISU ReD: Research and eData Theses and Dissertations 3-10-2019 Social Emotional Learning Through Depression Education In A High School Setting Antonette Minniti Illinois State University, [email protected] Follow this and additional works at: https://ir.library.illinoisstate.edu/etd Part of the Educational Psychology Commons, Elementary and Middle and Secondary Education Administration Commons, Public Health Education and Promotion Commons, School Psychology Commons, Secondary Education and Teaching Commons, and the Student Counseling and Personnel Services Commons Recommended Citation Minniti, Antonette, "Social Emotional Learning Through Depression Education In A High School Setting" (2019). Theses and Dissertations. 1043. https://ir.library.illinoisstate.edu/etd/1043 This Dissertation is brought to you for free and open access by ISU ReD: Research and eData. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of ISU ReD: Research and eData. For more information, please contact [email protected]. SOCIAL EMOTIONAL LEARNING THROUGH DEPRESSION EDUCATION IN A HIGH SCHOOL SETTING Antonette Minniti 125 Pages Education on depression is an important part of social emotional learning. Lacking emotion regulation skills tend to lead to larger problems, such as academic struggles, disconnect from peers, strife at home and trouble in interpersonal relationships. Research in depression education or educational programs connected to mental health literacy are minimal, especially at the high school level. The purpose of this research focused on examining the impact of one depression education program, John Hopkins Hospital’s Adolescent Depression Awareness Program (ADAP). The ADAP is a three-day program that informs students about the facts of depression, how it is treated, and what to do if the individual students or someone they know needs help with depression. -

HIV and Substance Use October 2016
HIV and Substance Use October 2016 Fast Facts • Alcohol and other drugs can affect a person’s judgment and increase risk of getting or transmitting HIV. • In people living with HIV, substance use can worsen the overall consequences of HIV. • Social and structural factors make it difficult to prevent HIV among people who use substances. Substance use disorders, which are problematic patterns of using alcohol or another substance, such as crack cocaine, methamphetamine (“meth”), amyl nitrite (“poppers”), prescription opioids, and heroin, are closely associated with HIV and other sexually transmitted diseases. Injection drug use (IDU) can be a direct route of HIV transmission if people share needles, syringes, or other injection materials that are contaminated with HIV. However, drinking alcohol and ingesting, smoking, or inhaling drugs are also associated with increased risk for HIV. These substances alter judgment, which can lead to risky sexual behaviors (e.g., having sex without a condom, having multiple partners) that can make people more likely to get and transmit HIV. In people living with HIV, substance use can hasten disease progression, affect adherence to antiretroviral therapy (HIV medicine), and worsen the overall consequences of HIV. Commonly Used Substances and HIV Risk • Alcohol. Excessive alcohol consumption, notably binge drinking, can be an important risk factor for HIV because it is linked to risky sexual behaviors and, among people living with HIV, can hurt treatment outcomes. • Opioids. Opioids, a class of drugs that reduce pain, include both prescription drugs and heroin. They are associated with HIV risk behaviors such as needle sharing when injected and risky sex, and have been linked to a recent HIV outbreak. -

About Emotions There Are 8 Primary Emotions. You Are Born with These
About Emotions There are 8 primary emotions. You are born with these emotions wired into your brain. That wiring causes your body to react in certain ways and for you to have certain urges when the emotion arises. Here is a list of primary emotions: Eight Primary Emotions Anger: fury, outrage, wrath, irritability, hostility, resentment and violence. Sadness: grief, sorrow, gloom, melancholy, despair, loneliness, and depression. Fear: anxiety, apprehension, nervousness, dread, fright, and panic. Joy: enjoyment, happiness, relief, bliss, delight, pride, thrill, and ecstasy. Interest: acceptance, friendliness, trust, kindness, affection, love, and devotion. Surprise: shock, astonishment, amazement, astound, and wonder. Disgust: contempt, disdain, scorn, aversion, distaste, and revulsion. Shame: guilt, embarrassment, chagrin, remorse, regret, and contrition. All other emotions are made up by combining these basic 8 emotions. Sometimes we have secondary emotions, an emotional reaction to an emotion. We learn these. Some examples of these are: o Feeling shame when you get angry. o Feeling angry when you have a shame response (e.g., hurt feelings). o Feeling fear when you get angry (maybe you’ve been punished for anger). There are many more. These are NOT wired into our bodies and brains, but are learned from our families, our culture, and others. When you have a secondary emotion, the key is to figure out what the primary emotion, the feeling at the root of your reaction is, so that you can take an action that is most helpful. . -

National Vital Statistics Report: Drugs Most Frequently Involved In
National Vital Statistics Reports Volume 67, Number 9 December 12, 2018 Drugs Most Frequently Involved in Drug Overdose Deaths: United States, 2011–2016 by Holly Hedegaard, M.D., M.S.P.H., and Brigham A. Bastian, B.S., National Center for Health Statistics; James P. Trinidad, M.P.H., M.S., U.S. Food and Drug Administration; Merianne Spencer, M.P.H., and Margaret Warner, Ph.D., National Center for Health Statistics Abstract overdose deaths involving methadone decreased from 1.4 per 100,000 in 2011 to 1.1 in 2016. The 10 most frequently Objective—This report identifies the specific drugs involved mentioned drugs often were found in combination with each most frequently in drug overdose deaths in the United States other. The drugs most frequently mentioned varied by the intent from 2011 through 2016. of the drug overdose death. In 2016, the drugs most frequently Methods—Record-level data from the 2011–2016 National mentioned in unintentional drug overdose deaths were fentanyl, Vital Statistics System–Mortality files were linked to electronic heroin, and cocaine, while the drugs most frequently mentioned files containing literal text information from death certificates. in suicides by drug overdose were oxycodone, diphenhydramine, Drug overdose deaths were identified using the International hydrocodone, and alprazolam. Classification of Diseases, Tenth Revision underlying cause- Conclusions—This report identifies patterns in the specific of-death codes X40–X44, X60–X64, X85, and Y10–Y14. Drug drugs most frequently involved in drug overdose deaths from mentions were identified by searching the literal text in three 2011 through 2016 and highlights the importance of complete fields of the death certificate: the causes of death from Part I, and accurate reporting in the literal text on death certificates.