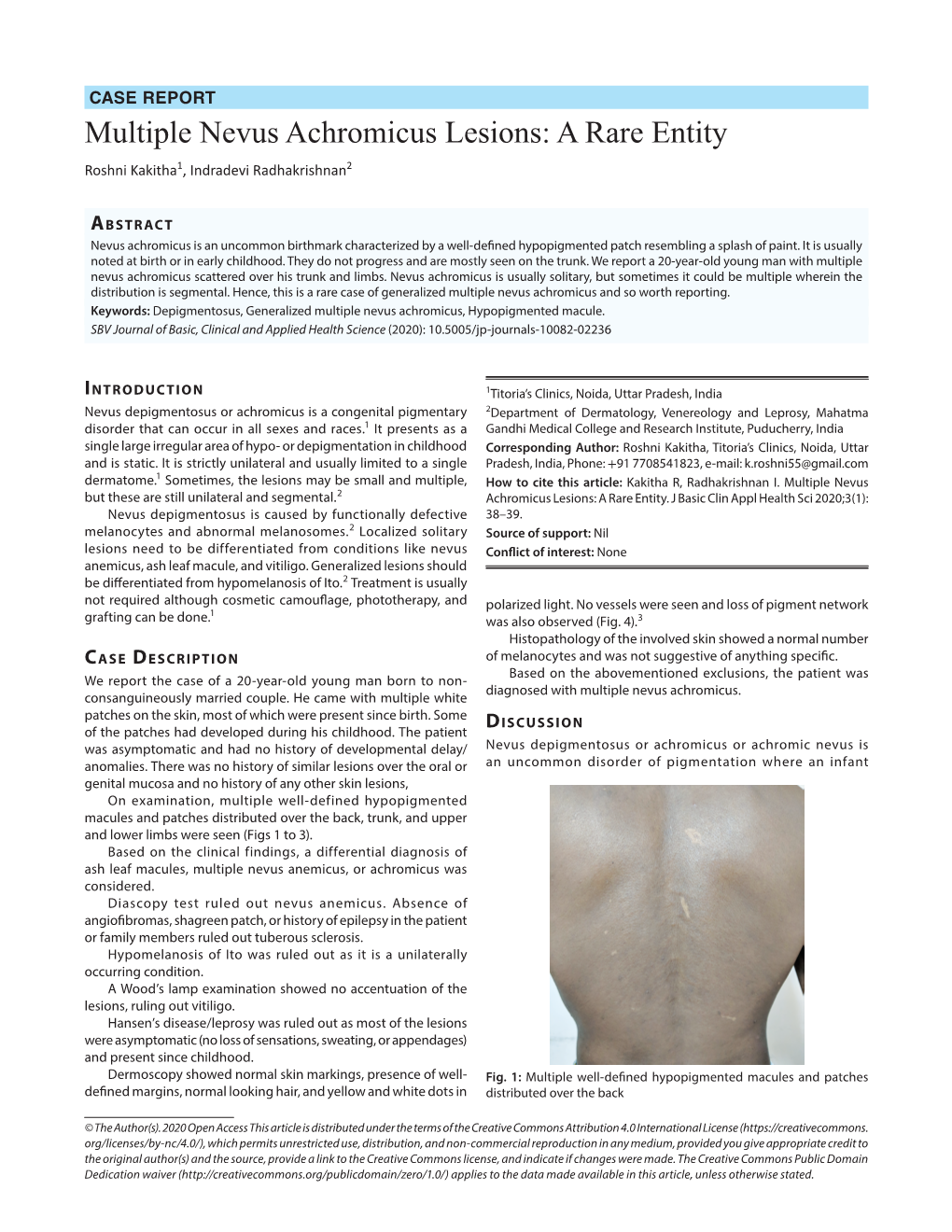
Multiple Nevus Achromicus Lesions: a Rare Entity Roshni Kakitha1, Indradevi Radhakrishnan2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Melanocytes and Their Diseases
Downloaded from http://perspectivesinmedicine.cshlp.org/ on October 2, 2021 - Published by Cold Spring Harbor Laboratory Press Melanocytes and Their Diseases Yuji Yamaguchi1 and Vincent J. Hearing2 1Medical, AbbVie GK, Mita, Tokyo 108-6302, Japan 2Laboratory of Cell Biology, National Cancer Institute, National Institutes of Health, Bethesda, Maryland 20892 Correspondence: [email protected] Human melanocytes are distributed not only in the epidermis and in hair follicles but also in mucosa, cochlea (ear), iris (eye), and mesencephalon (brain) among other tissues. Melano- cytes, which are derived from the neural crest, are unique in that they produce eu-/pheo- melanin pigments in unique membrane-bound organelles termed melanosomes, which can be divided into four stages depending on their degree of maturation. Pigmentation production is determined by three distinct elements: enzymes involved in melanin synthesis, proteins required for melanosome structure, and proteins required for their trafficking and distribution. Many genes are involved in regulating pigmentation at various levels, and mutations in many of them cause pigmentary disorders, which can be classified into three types: hyperpigmen- tation (including melasma), hypopigmentation (including oculocutaneous albinism [OCA]), and mixed hyper-/hypopigmentation (including dyschromatosis symmetrica hereditaria). We briefly review vitiligo as a representative of an acquired hypopigmentation disorder. igments that determine human skin colors somes can be divided into four stages depend- Pinclude melanin, hemoglobin (red), hemo- ing on their degree of maturation. Early mela- siderin (brown), carotene (yellow), and bilin nosomes, especially stage I melanosomes, are (yellow). Among those, melanins play key roles similar to lysosomes whereas late melanosomes in determining human skin (and hair) pigmen- contain a structured matrix and highly dense tation. -

Uniform Faint Reticulate Pigment Network - a Dermoscopic Hallmark of Nevus Depigmentosus
Our Dermatology Online Letter to the Editor UUniformniform ffaintaint rreticulateeticulate ppigmentigment nnetworketwork - A ddermoscopicermoscopic hhallmarkallmark ooff nnevusevus ddepigmentosusepigmentosus Surit Malakar1, Samipa Samir Mukherjee2,3, Subrata Malakar3 11st Year Post graduate, Department of Dermatology, SUM Hospital Bhubaneshwar, India, 2Department of Dermatology, Cloud nine Hospital, Bangalore, India, 3Department of Dermatology, Rita Skin Foundation, Kolkata, India Corresponding author: Dr. Samipa Samir Mukherjee, E-mail: [email protected] Sir, ND is a form of cutaneous mosaicism with functionally defective melanocytes and abnormal melanosomes. Nevus depigmentosus (ND) is a localized Histopathologic examination shows normal to hypopigmentation which most of the time is congenital decreased number of melanocytes with S-100 stain and and not uncommonly a diagnostic challenge. ND lesions less reactivity with 3,4-dihydroxyphenylalanine reaction are sometimes difficult to differentiate from other and no melanin incontinence [2]. Electron microscopic hypopigmented lesions like vitiligo, ash leaf macules and findings show stubby dendrites of melanocytes nevus anemicus. Among these naevus depigmentosus containing autophagosomes with aggregates of poses maximum difficulty in differentiating from ash melanosomes. leaf macules because of clinical as well as histological similarities [1]. Although the evolution of newer diagnostic For ease of understanding the pigmentary network techniques like dermoscopy has obviated the -

Chapter 3 Bacterial and Viral Infections
GBB03 10/4/06 12:20 PM Page 19 Chapter 3 Bacterial and viral infections A mighty creature is the germ gain entry into the skin via minor abrasions, or fis- Though smaller than the pachyderm sures between the toes associated with tinea pedis, His customary dwelling place and leg ulcers provide a portal of entry in many Is deep within the human race cases. A frequent predisposing factor is oedema of His childish pride he often pleases the legs, and cellulitis is a common condition in By giving people strange diseases elderly people, who often suffer from leg oedema Do you, my poppet, feel infirm? of cardiac, venous or lymphatic origin. You probably contain a germ The affected area becomes red, hot and swollen (Ogden Nash, The Germ) (Fig. 3.1), and blister formation and areas of skin necrosis may occur. The patient is pyrexial and feels unwell. Rigors may occur and, in elderly Bacterial infections people, a toxic confusional state. In presumed streptococcal cellulitis, penicillin is Streptococcal infection the treatment of choice, initially given as ben- zylpenicillin intravenously. If the leg is affected, Cellulitis bed rest is an important aspect of treatment. Where Cellulitis is a bacterial infection of subcutaneous there is extensive tissue necrosis, surgical debride- tissues that, in immunologically normal individu- ment may be necessary. als, is usually caused by Streptococcus pyogenes. A particularly severe, deep form of cellulitis, in- ‘Erysipelas’ is a term applied to superficial volving fascia and muscles, is known as ‘necrotiz- streptococcal cellulitis that has a well-demarcated ing fasciitis’. This disorder achieved notoriety a few edge. -

Skin Pigmentary Variants in Rana Nigromaculata
Original Article J. Clin. Biochem. Nutr., 38, 195–203, May 2006 Skin Pigmentary Variants in Rana Nigromaculata Ichiro Tazawa, Hitoshi Okumoto, and Akihiko Kashiwagi* Division of Embryology and Genetics, Institute for Amphibian Biology, Graduate School of Science, Hiroshima University, 1-3-1 Kagamiyama, Higashihiroshima, Hiroshima 739-8526, Japan Received 22 December, 2005; Accepted 26 January, 2006 Summary Because there is mounting evidence to suggest that oxidative stress is involved in the pathophysiology of albinism, albino amphibians are useful tools for studies on imbalances in the oxidant-antioxidant system. In the course of maintaining albino mutant frog strains it was found that crosses between albino males and heterozygous females of Rana nigromaculata sometimes produce offspring displaying pigmentary mosaicism. After hatching hypopigmented portions appear on the left or right side of the body, and this is accompanied by such abnormalities as poor viability, asymmetrical curvature of the body toward the hypopigmented side, and limb deformity. Histological examination of mosaics showed the cells of various tissues (except kidney) to be smaller on the hypopigmented side and larger on the pigmented side compared to corresponding cells in wild type offspring. Cytogenetic analysis of cultured skin cells revealed that wild type and albino individuals were diploidal with 26 chromosomes, the same as normal R. nigromaculata. In mosaics on the other hand, cells of hypopigmented portions were almost exclusively haploidal with 13 chromosomes, while pigmented portions were a mixture of roughly 75% triploidal, 39 chromosome cells and roughly 25% haploidal, 13 chromosome cells. Key Words: albino, unilateral pigmentation, pigmentary mosaicism, chromosomal mosaicism, mixoploidy, haploid, triploid, Rana one means of assessing the involvement of reactive oxygen Introduction species (ROS) in biological processes such as aging. -

Lepromatous Leprosy with Erythema Nodosum Leprosum Presenting As
Lepromatous Leprosy with Erythema Nodosum Leprosum Presenting as Chronic Ulcers with Vasculitis: A Case Report and Discussion Anny Xiao, DO,* Erin Lowe, DO,** Richard Miller, DO, FAOCD*** *Traditional Rotating Intern, PGY-1, Largo Medical Center, Largo, FL **Dermatology Resident, PGY-2, Largo Medical Center, Largo, FL ***Program Director, Dermatology Residency, Largo Medical Center, Largo, FL Disclosures: None Correspondence: Anny Xiao, DO; Largo Medical Center, Graduate Medical Education, 201 14th St. SW, Largo, FL 33770; 510-684-4190; [email protected] Abstract Leprosy is a rare, chronic, granulomatous infectious disease with cutaneous and neurologic sequelae. It can be a challenging differential diagnosis in dermatology practice due to several overlapping features with rheumatologic disorders. Patients with leprosy can develop reactive states as a result of immune complex-mediated inflammatory processes, leading to the appearance of additional cutaneous lesions that may further complicate the clinical picture. We describe a case of a woman presenting with a long history of a recurrent bullous rash with chronic ulcers, with an evolution of vasculitic diagnoses, who was later determined to have lepromatous leprosy with reactive erythema nodosum leprosum (ENL). Introduction accompanied by an intense bullous purpuric rash on management of sepsis secondary to bacteremia, Leprosy is a slowly progressive disease caused by bilateral arms and face. For these complaints she was with lower-extremity cellulitis as the suspected infection with Mycobacterium leprae (M. leprae). seen in a Complex Medical Dermatology Clinic and source. A skin biopsy was taken from the left thigh, Spread continues at a steady rate in several endemic clinically diagnosed with cutaneous polyarteritis and histopathology showed epidermal ulceration countries, with more than 200,000 new cases nodosa. -

Leprosy in Two Patients with Relapsing Remitting Multiple Sclerosis Treated with Fingolimod Alfred Balasa, M.D.1 and George J
Leprosy in Two Patients with Relapsing Remitting Multiple Sclerosis Treated with Fingolimod Alfred Balasa, M.D.1 and George J. Hutton, M.D.2 1 Department of Pediatrics, Section of Pediatric Neurology and Developmental Neuroscience; 2 Department of Neurology; Baylor College of Medicine, Houston, Texas Background A B Leprosy (Hansen’s disease) is a chronic infection caused by Mycobacterium leprae. The disease develops over months to years and may cause extensive damage to the skin and peripheral nervous system. A B In multiple sclerosis (MS), fingolimod treatment is Figure 3. Immune response in the polar clinical forms of leprosy. known to increase the risk for infections. There is one prior reported case of leprosy while on [A] In tuberculoid leprosy (TT) patients, the innate immune response is activated by M. leprae through toll-like receptors (TLR2/1). IL-15 fingolimod for relapsing remitting multiple sclerosis stimulates the vitamin D-dependent antimicrobial program in macrophages and inhibits phagocytosis of mycobacteria. These events (RRMS). We report two further cases of leprosy in promote a Th1 T-cell cytokine response (IFN-γ, IL-2, TNF, and IL-15) that contains the infection in well-formed granulomas, and a Th17 patients with RRMS and treated with fingolimod. C D response (IL-17A, IL-17F, IL-21 and IL-22) that leads to tissue inflammation and destruction, neutrophil recruitment, macrophage activation, and enhancement of Th1 effector cells. [B] In lepromatous leprosy (LL) patients, IL-4, IL-10, leukocyte immunoglobulin-like receptor subfamily A member 2 (LILRA2), and oxidized phospholipids inhibit TLR2/1-induced cytokine responses but preserve IL-10 release. -

Pityriasis Alba Revisited: Perspectives on an Enigmatic Disorder of Childhood
Pediatric ddermatologyermatology Series Editor: Camila K. Janniger, MD Pityriasis Alba Revisited: Perspectives on an Enigmatic Disorder of Childhood Yuri T. Jadotte, MD; Camila K. Janniger, MD Pityriasis alba (PA) is a localized hypopigmented 80 years ago.2 Mainly seen in the pediatric popula- disorder of childhood with many existing clinical tion, it primarily affects the head and neck region, variants. It is more often detected in individuals with the face being the most commonly involved with a darker complexion but may occur in indi- site.1-3 Pityriasis alba is present in individuals with viduals of all skin types. Atopy, xerosis, and min- all skin types, though it is more noticeable in those with eral deficiencies are potential risk factors. Sun a darker complexion.1,3 This condition also is known exposure exacerbates the contrast between nor- as furfuraceous impetigo, erythema streptogenes, mal and lesional skin, making lesions more visible and pityriasis streptogenes.1 The term pityriasis alba and patients more likely to seek medical atten- remains accurate and appropriate given the etiologic tion. Poor cutaneous hydration appears to be a elusiveness of the disorder. common theme for most riskCUTIS factors and may help elucidate the pathogenesis of this disorder. The Epidemiology end result of this mechanism is inappropriate mel- Pityriasis alba primarily affects preadolescent children anosis manifesting as hypopigmentation. It must aged 3 to 16 years,4 with onset typically occurring be differentiated from other disorders of hypopig- between 6 and 12 years of age.5 Most patients are mentation, such as pityriasis versicolor alba, vitiligo, younger than 15 years,3 with up to 90% aged 6 to nevus depigmentosus, and nevus anemicus. -

Colocalized Nevus Depigmentosus and Lentigines Prashansa Jaiswal, Sundeep Chowdhry, Paschal D’ Souza
2XU'HUPDWRORJ\2QOLQH Case Report Colocalized nevus depigmentosus and lentigines Prashansa Jaiswal, Sundeep Chowdhry, Paschal D’ Souza Department of Dermatology, Venereology and Leprology, Employees’ State Insurance Corporation Post Graduate Institute of Medical Sciences & Research, Basaidarapur, New Delhi - 110 015, India Corresponding author: Assist. Prof. Sundeep Chowdhry, E-mail: [email protected] ABSTRACT Nevus depigmentosus (ND)is classically defined as a congenital nonprogressive hypopigmented macule, stable in size and distribution. A 17 year girl presented with hypopigmented patch with indented borders, present on the right side of face and neck since 3 years of age. Later on at the age of 5, numerous hyperpigmented punctiform spots appeared exclusively on the hyperpigmented area. On sun exposure, the hypopigmented area neither reddened nor burnt. On diascopy the margin of the hypopigmented lesion remained delineated. The dermoscopic examination showed 1-4 millimeters sized hyperpigmented lesions with a barely visible pseudonet, leading to the final diagnosis of colocalized nevus depigmentosus and lentigines. Key words: Nevus; Hypopigmentation; Reverse; Mutation; Pigmentation INTRODUCTION 25 X 8 centimeters was present at the angle of mouth on right side, further extending to lateral side of right ear, Nevus depigmentosus (ND)is a rare, congenital, right angle of jaw, lateral right side of neck to about 6 stable hypomelanosis first described by Lesser in centimeters below the clavicle. It was irregular in shape 1884 [1]. The lesions usually present as dermatomal with serrated irregular margins. The surface was smooth or quasidermatomal macules commonly on the trunk, and had multiple oval dark brown coloured macules of lower abdomen, or proximal extremities. They are off- 1 to 4 mm in size (Fig. -

Phacomatosis Spilorosea Versus Phacomatosis Melanorosea
Acta Dermatovenerologica 2021;30:27-30 Acta Dermatovenerol APA Alpina, Pannonica et Adriatica doi: 10.15570/actaapa.2021.6 Phacomatosis spilorosea versus phacomatosis melanorosea: a critical reappraisal of the worldwide literature with updated classification of phacomatosis pigmentovascularis Daniele Torchia1 ✉ 1Department of Dermatology, James Paget University Hospital, Gorleston-on-Sea, United Kingdom. Abstract Introduction: Phacomatosis pigmentovascularis is a term encompassing a group of disorders characterized by the coexistence of a segmental pigmented nevus of melanocytic origin and segmental capillary nevus. Over the past decades, confusion over the names and definitions of phacomatosis spilorosea, phacomatosis melanorosea, and their defining nevi, as well as of unclassifi- able phacomatosis pigmentovascularis cases, has led to several misplaced diagnoses in published cases. Methods: A systematic and critical review of the worldwide literature on phacomatosis spilorosea and phacomatosis melanorosea was carried out. Results: This study yielded 18 definite instances of phacomatosis spilorosea and 14 of phacomatosis melanorosea, with one and six previously unrecognized cases, respectively. Conclusions: Phacomatosis spilorosea predominantly involves the musculoskeletal system and can be complicated by neuro- logical manifestations. Phacomatosis melanorosea is sometimes associated with ancillary cutaneous lesions, displays a relevant association with vascular malformations of the brain, and in general appears to be a less severe syndrome. -

Immunological Aspects of Leprosy with Special Reference to Autoimmune Diseases 0
'Bull. Org. mond. Sante 1969, 41, 793-804 Bull. Wld Hlth Org. Immunological Aspects of Leprosy with Special Reference to Autoimmune Diseases 0. WAGER1 Leprosy, particularly lepromatous leprosy, is associated with a multitude of (auto) immune aberrations, and its clinical features also have much in common with the collagen diseases. Immunopathological studies of the 2 groups of diseases may thus elucidate the basic mechanisms of both. The reported evidencefor a genetically determined hyporeactivity ofcell-mediated (CM) immunity in lepromatous subjects is reviewed; most, but not all, of the findings fit such a hypothesis well. The possibility remains that the observed hyporeactivities may be secondary to direct effects of Mycobacterium leprae. Evidencefor a general hyperreactivity of the antibody-mediated (AM) immunity in lepromatous leprosy is then reviewed and considered to be fragmentary. The concept and general criteria of autoimmunity are discussed briefly and the high incidence in lepromatous leprosy of various (auto)immune aberrations, resembling those in systemic lupus erythematosus (SLE) and in rheumatoid arthritis is reviewed. Although autoantibodies are not likely to be directly deleterious to the host, immune complexes containing autoantibodies may be pathogenic. Mixed cryoimmunoglobulins, consisting of 2 (IgG-IgM or IgG-IgA) or 3 immunoglo-. bulins, and occasionally also containing measurable amounts of complement components, have recently been encountered in SLE and its variants and also in a number of microbial diseases with autoimmune features (syphilis, streptococcal nephritis and endocarditis, mononucleosis, Mycoplasma pneumoniae pneumonia). They may represent circulating immune complexes, analogous to the IgM (IgA) rheumatoid factors in combination with their IgG reactants. In leprosy also, the existence of pathogenic immune complexes is indirectly suggested by mixed cryoglobulinemia andfurther by a number of other features reviewed in this article. -
2018 Abstract Book
CONTENTS Table of Contents INFORMATION Continuing Medical Education .................................................................................................5 Guidelines for Speakers ..........................................................................................................6 Guidelines for Poster Presentations .........................................................................................8 SPEAKER ABSTRACTS Abstracts ...............................................................................................................................9 POSTER ABSTRACTS Basic Research (Location – Room 101) ...............................................................................63 Clinical (Location – Room 8) ..............................................................................................141 2018 Joint Global Neurofibromatosis Conference · Paris, France · November 2-6, 2018 | 3 4 | 2018 Joint Global Neurofibromatosis Conference · Paris, France · November 2-6, 2018 EACCME European Accreditation Council for Continuing Medical Education 2018 Joint Global Neurofibromatosis Conference Paris, France, 02/11/2018–06/11/2018 has been accredited by the European Accreditation Council for Continuing Medical Education (EACCME®) for a maximum of 27 European CME credits (ECMEC®s). Each medical specialist should claim only those credits that he/she actually spent in the educational activity. The EACCME® is an institution of the European Union of Medical Specialists (UEMS), www.uems.net. Through an agreement between -

Preceded by Multiple Diagnostic. X-Rays One Year Prior to The
A Malformation Complex of Ectrodactyly, Clefting and Hypomelanosis of Ito (Incontinentia Pigmenti Achromians) RAY E. STEWART, D.M.D., M.S. STEVEN FUNDERBURK, M.D. YOSHIO SETOGUCHI, M.D. Torrance, California 90509 A case is described which, at birth, had a bizarre pattern of Aypopigmentation (incontinentia pigment achromians), ectrodactyly involving all four extremities, and unilateral cleft lip and palate. This patient does not have the seizures or other neurological and developmental anomalies previously described as associated with Aypopigmentation of Ito. This condition is also clearly different from the syndrome of ectrodactyly, ectodermal dysplasia, and clefting (EEC). We have recently observed four-month-old tone. The child has developed normally, Mexican-American female infant with an in- reaching all of her age-appropriate milestones teresting constellation of anomalies, including with no evidence of neurological or other _ unilateral complete clefts of the lip and pal- problems. The Denver Developmental Scales ate, ectrodactyly of the hands and feet, and yielded an intelligence quotient of 100 at 14 generalized abnormalities in skin pigmenta- months of age. tion. The association of ectodermal changes, Examination of the head and neck revealed ectrodactyly, and oralfacial clefting has been unilateral complete cleft of the lip and palate. well documented in the EEC syndrome (ec- There was mild hypoplasia of the right exter- trodactyly, ectodermal dysplasia, and clefting nal ear (Figure 1). syndrome). However, this patient clearly does Examination of the skin revealed a peculiar not fall into this classification. generalized pattern of hypopigmentation over the entire body, including the head, neck, and Clinical findings face. On the dorsum, the pigmentation as- The child was the product of a full-term, sumed a swirling pattern.