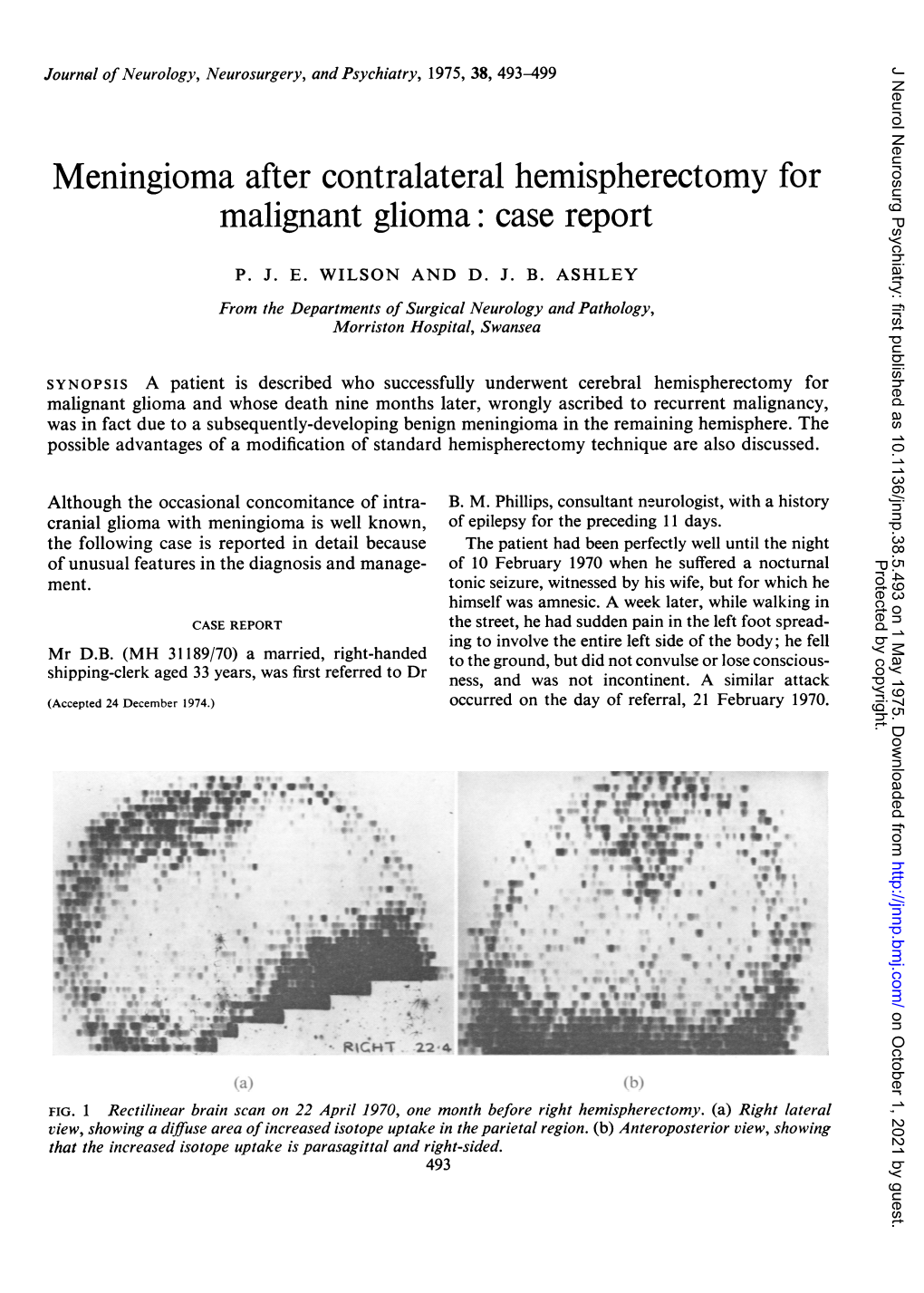
Meningioma After Contralateral Hemispherectomy for Malignant Glioma: Case Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Late Complications of Hemispherectomy: Report of a Case Relieved by Surgery
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.33.3.372 on 1 June 1970. Downloaded from J. Neurol. Neurosurg. Psychiat., 1970, 33, 372-375 Late complications of hemispherectomy: report of a case relieved by surgery NINAN T. MATHEW, JACOB ABRAHAM, AND JACOB CHANDY From the Department of Neurological Sciences, Christian Medical College Hospital, Vellore, S. India SUM M A RY A case of Sturge-Weber disease treated with left hemispherectomy presented, 11 years later, with complications related to delayed intracranial haemorrhage. A loculation syndrome of the right lateral ventricle was detected and it was corrected by a ventriculoatrial shunt operation. The side of the hemispherectomy was evacuated of all the chronic products of haemorrhage, including the subdural membrane. The patient was relieved of her symptoms. It is considered that compli- cations related to delayed haemorrhage after hemispherectomy are remediable. Immediate and delayed complications occur after 10 July 1969, with persistent headache, vomiting, and hemispherectomy. Early complications include ob- increasing drowsiness of three weeks' duration. She was structive hydrocephalus and herniations of the born with a Sturge-Weber syndrome and had had a leftProtected by copyright. remaining hemisphere (Cabieses, Jeri, and Landa, hemispherectomy performed in another country 11 years before. She was free from seizures and major behavioural 1957; Laine, Pruvot, and Osson, 1964). A syndrome problems and was attending a school for backward of delayed intracranial haemorrhage was reported by children till November 1968, when she developed severe Oppenheimer and Griffith (1966). The essential constant headache, vomiting, and drowsiness. She was features of the syndrome are (I) an infantile hemi- admitted elsewhere in early December 1968, where plegia treated by hemispherectomy; (2) a trouble- browniish yellow fluid with a protein content of 1,150 mg/ free period lasting for some years; (3) a period of 100 nil. -

This Article Appeared in a Journal Published by Elsevier. the Attached
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright Author's personal copy Neuropsychologia 48 (2010) 1683–1688 Contents lists available at ScienceDirect Neuropsychologia journal homepage: www.elsevier.com/locate/neuropsychologia Cerebral lateralization of vigilance: A function of task difficulty a, b b c William S. Helton ∗, Joel S. Warm , Lloyd D. Tripp , Gerald Matthews , Raja Parasuraman e, Peter A. Hancock d a Department of Psychology, University of Canterbury, Private Bag 4800, Christchurch, New Zealand b Air Force Research Laboratory, Wright Patterson Air Force Base, Dayton, OH, USA c Department of Psychology, University of Cincinnati, OH, USA d Department of Psychology, University of Central Florida, Orlando, FL, USA e Department of Psychology, George Mason University, VA, USA article info a b s t r a c t Article history: Functional near infrared spectroscopy (fNIRS) measures of cerebral oxygenation levels were collected Received 6 July 2009 from participants performing difficult and easy versions of a 12 min vigilance task and for controls who Received in revised form 10 February 2010 merely watched the displays without a work imperative. -

Reorganization of the Social Brain in Individuals with Only One Intact Cerebral Hemisphere
brain sciences Article Reorganization of the Social Brain in Individuals with Only One Intact Cerebral Hemisphere Dorit Kliemann 1,2,3,*, Ralph Adolphs 4,5, Lynn K. Paul 4, J. Michael Tyszka 4 and Daniel Tranel 1,3,6 1 Department of Psychological and Brain Sciences, University of Iowa, Iowa City, IA 52242, USA; [email protected] 2 Department of Psychiatry, University of Iowa, Iowa City, IA 52242, USA 3 Iowa Neuroscience Institute, University of Iowa, Iowa City, IA 52242, USA 4 Division of Humanities and Social Sciences, California Institute of Technology, Pasadena, CA 91125, USA; [email protected] (R.A.); [email protected] (L.K.P.); [email protected] (J.M.T.) 5 Division of Biology and Bioengineering, California Institute of Technology, Pasadena, CA 91125, USA 6 Department of Neurology, University of Iowa, Iowa City, IA 52242, USA * Correspondence: [email protected] Abstract: Social cognition and emotion are ubiquitous human processes that recruit a reliable set of brain networks in healthy individuals. These brain networks typically comprise midline (e.g., medial prefrontal cortex) as well as lateral regions of the brain including homotopic regions in both hemispheres (e.g., left and right temporo-parietal junction). Yet the necessary roles of these networks, and the broader roles of the left and right cerebral hemispheres in socioemotional functioning, remains debated. Here, we investigated these questions in four rare adults whose right (three cases) or left (one case) cerebral hemisphere had been surgically removed (to a large extent) to treat epilepsy. We studied four closely matched healthy comparison participants, and also compared the patient findings to data from a previously published larger healthy comparison sample (n = 33). -

Anesthesia for Anatomical Hemispherectomy, 217 Antiepileptic
Index Note: Page numbers followed by f and t indicate fi gures and tables, respectively. A Anesthesia Academic skills assessment, in neuropsychological assess- for anatomical hemispherectomy, 217 ment, 105 antiepileptic drugs and, 114 Acid-base status, perioperative management of, 114 for awake craniotomy, 116 Adaptive function assessment, in neuropsychological for corpus callosotomy, 116 assessment, 106 for hemispherectomy, 116–117, 217 After-discharges, 31 induction of, 114 Age of patient maintenance of, 115 and adaptive plasticity, 15–16 for posterior quadrantic surgery, 197–198 and cerebral blood fl ow, 113 Sturge-Weber syndrome and, 113 at lesion occurrence, and EEG fi ndings, 16 in surgery for subhemispheric epilepsy, 197–198 and pediatric epilepsy surgery, 3 tuberous sclerosis and, 113 and physiological diff erences, 113 for vagus nerve stimulation, 116 and seizure semiology, 41 Angioma(s) at surgery, and outcomes, 19 cutaneous, in Sturge-Weber syndrome, 206 Airway facial, 206 intraoperative management of, 114–115 Angular gyrus, electrical stimulation of, 48 preoperative evaluation, 113 Anterior lobe lobectomy (ATL) Alien limb phenomenon, stimulation-induced, 49 left (L-ATL), and language function, 76 [11C]Alphamethyl-L-tryptophan (AMT), as PET radiotracer, and memory function, 77–78 83–84, 86 Anteromesial temporal lobectomy (AMTL), 136–146 in extratemporal lobe epilepsy, 86–87, 175 complications of, 144–145 in postsurgical evaluation, 90 craniotomy in, 138, 139f in temporal lobe epilepsy, 86 historical perspective on, 136–137 in tuberous -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Non-Invasive Alternatives to the Wada Test in the Presurgical Evaluation of Language and Memory Functions in Epilepsy Patients
Special article Epileptic Disord 2007; 9 (2): 111-26 Non-invasive alternatives to the Wada test in the presurgical evaluation of language and memory functions in epilepsy patients Isabelle Pelletier1,2, Hannelore C. Sauerwein1,2, Franco Lepore1,2, Dave Saint-Amour1,3, Maryse Lassonde1,2 1 Centre de recherche du Centre Hospitalier Universitaire Mère-Enfant (Sainte-Justine) 2 Centre de Recherche en Neuropsychologie et Cognition, Département de psychologie 3 Département d’ophtalmologie, Université de Montréal, Canada Received December 4, 2006; Accepted March 26, 2007 ABSTRACT – The cognitive outcome of the surgical removal of an epileptic focus depends on the assessment of the localisation and functional capacity of language and memory areas which need to be spared by the neurosurgeon. Traditionally, presurgical evaluation of epileptic patients has been achieved by means of the intracarotid amobarbital test assisted by neuropsychological measures. However, the advent of neuroimaging techniques has provided new ways of assessing these functions by means of non-invasive or minimally invasive methods, such as anatomical and functional magnetic resonance imaging, positron emission tomography, single-photon emission computed tomography, transcranial magnetic stimulation, functional transcranial Doppler monitoring, magnetoencephalography and near infrared spectroscopy. This paper aims at comparing and evaluating the traditional and recent preoperative approaches from a neuropsychological perspective. Key words: epilepsy surgery, neuroimaging technique, intracarotid amobarbital test, language, memory Surgery to remove epileptic brain tis- providing complete seizure control sue (i.e., lobectomy, lesionectomy, and improved quality of life. The out- hemispherectomy) is a widely used come of the surgery depends on accu- and effective treatment for patients rate localization and lateralization of Correspondence: suffering from intractable seizures the epileptogenic zone as well as on Maryse Lassonde (Gates and Dunn 1999). -

1 Annex 2. AHRQ ICD-9 Procedure Codes 0044 PROC-VESSEL
Annex 2. AHRQ ICD-9 Procedure Codes 0044 PROC-VESSEL BIFURCATION OCT06- 0201 LINEAR CRANIECTOMY 0050 IMPL CRT PACEMAKER SYS 0202 ELEVATE SKULL FX FRAGMNT 0051 IMPL CRT DEFIBRILLAT SYS 0203 SKULL FLAP FORMATION 0052 IMP/REP LEAD LF VEN SYS 0204 BONE GRAFT TO SKULL 0053 IMP/REP CRT PACEMAKR GEN 0205 SKULL PLATE INSERTION 0054 IMP/REP CRT DEFIB GENAT 0206 CRANIAL OSTEOPLASTY NEC 0056 INS/REP IMPL SENSOR LEAD OCT06- 0207 SKULL PLATE REMOVAL 0057 IMP/REP SUBCUE CARD DEV OCT06- 0211 SIMPLE SUTURE OF DURA 0061 PERC ANGIO PRECEREB VES (OCT 04) 0212 BRAIN MENINGE REPAIR NEC 0062 PERC ANGIO INTRACRAN VES (OCT 04) 0213 MENINGE VESSEL LIGATION 0066 PTCA OR CORONARY ATHER OCT05- 0214 CHOROID PLEXECTOMY 0070 REV HIP REPL-ACETAB/FEM OCT05- 022 VENTRICULOSTOMY 0071 REV HIP REPL-ACETAB COMP OCT05- 0231 VENTRICL SHUNT-HEAD/NECK 0072 REV HIP REPL-FEM COMP OCT05- 0232 VENTRI SHUNT-CIRCULA SYS 0073 REV HIP REPL-LINER/HEAD OCT05- 0233 VENTRICL SHUNT-THORAX 0074 HIP REPL SURF-METAL/POLY OCT05- 0234 VENTRICL SHUNT-ABDOMEN 0075 HIP REP SURF-METAL/METAL OCT05- 0235 VENTRI SHUNT-UNINARY SYS 0076 HIP REP SURF-CERMC/CERMC OCT05- 0239 OTHER VENTRICULAR SHUNT 0077 HIP REPL SURF-CERMC/POLY OCT06- 0242 REPLACE VENTRICLE SHUNT 0080 REV KNEE REPLACEMT-TOTAL OCT05- 0243 REMOVE VENTRICLE SHUNT 0081 REV KNEE REPL-TIBIA COMP OCT05- 0291 LYSIS CORTICAL ADHESION 0082 REV KNEE REPL-FEMUR COMP OCT05- 0292 BRAIN REPAIR 0083 REV KNEE REPLACE-PATELLA OCT05- 0293 IMPLANT BRAIN STIMULATOR 0084 REV KNEE REPL-TIBIA LIN OCT05- 0294 INSERT/REPLAC SKULL TONG 0085 RESRF HIPTOTAL-ACET/FEM -

Hope in One Hemisphere for BIA IA Conference 2017
2/24/17 Age 5 Age 13 Presented by: Roxanne Cogil, Parent Brain Injury Alliance of Iowa Annual Conference: March 3, 2017 Disclaimer This lecture is simply the view from a parent’s perspective and not the view of the Epilepsy Foundation or the Hemispherectomy Foundation. The lecture is for informational purposes only and it is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it. Objectives Ø To share a first-hand account of various brain injuries of a child. Ø To share various rehabilitation therapies utilized to help with neuroplasticity. Ø To share various skills learned to help with independence. 1 2/24/17 Journey of Brain Trauma/Injuries Ø Apnea/Blue Spells at Birth Ø New onset seizures and epilepsy diagnosis Ø Lesions in all lobes in right hemisphere Ø Rasmussen’s Encephalitis Ø Atrophy in right hemisphere Ø Hemispherectomy Brain Surgery Ø Cortical Dysplasia Ø Asymptomatic hydrocephalus Ø Returned seizures/spells Ø 2nd Brain Surgery (ETV) Apnea at birth Twins born on time at 27 weeks Met milestones. 2nd of twins born with suction cup. Bruise on forehead Apnea/Blue spells 10 days in NICU Life is good for almost 2 ½ years. 2 2/24/17 New onset seizures and epilepsy diagnosis Four major seizures in one day on 6/16/06, including a tonic clonic in the ER. Overnight stay and inpatient MRI. -

Corpus Callosotomy: a Palliative Therapeutic Technique May Help Identify Resectable Epileptogenic Foci
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Seizure (2007) 16, 545—553 www.elsevier.com/locate/yseiz CASE REPORT Corpus callosotomy: A palliative therapeutic technique may help identify resectable epileptogenic foci Dave F. Clarke a,*, James W. Wheless a, Monica M. Chacon b, Joshua Breier c, Mary-Kay Koenig c, Mark McManis b, Edward Castillo c, James E. Baumgartner c a Department of Pediatrics, Division of Pediatric Neurology, Le Bonheur Comprehensive Epilepsy Program, University of Tennessee Health Science Center, Memphis, TN, USA b Cook Children’s Hospital, Pediatric Neurology, Fort Worth, TX, USA c The Texas Comprehensive Epilepsy Program, Department of Neurosurgery, University of Texas Health Science Center at Houston, Houston, TX, USA Received 2 March 2007; received in revised form 4 April 2007; accepted 16 April 2007 KEYWORDS Summary Corpus callosotomy has a long history as a palliative treatment for Corpus callosotomy; intractable epilepsy. Identification of a single epileptogenic zone is critical to Epilepsy surgery; performing successful resective surgery. We describe three patients in which corpus Pediatric epilepsy; callosotomy allowed recognition of unapparent seizure foci, leading to subsequent Seizure; successful resection. Intractable epilepsy We retrospectively reviewed our epilepsy surgery database from 2003 to 2005 for children who had a prior callosotomy and were candidates for focal resection. All underwent magnetic resonance imaging and scalp video electroencephalograph monitoring, and two had magnetoencephalography, electrocorticography and/or intracranial video electroencephalograph monitoring. The children were 8 and 9 years old, and seizure onset varied from early infancy to early childhood. -

Stability and Plasticity of Functional Brain Networks After Hemispherectomy: Implications for Consciousness Research
1412 Editorial Commentary Stability and plasticity of functional brain networks after hemispherectomy: implications for consciousness research Lucina Q. Uddin1,2^ 1Department of Psychology, University of Miami, Coral Gables, Florida, USA; 2Neuroscience Program, University of Miami Miller School of Medicine, Miami, Florida, USA Correspondence to: Lucina Q. Uddin, PhD. University of Miami, P.O. Box 248185-0751, Coral Gables, FL 33124, USA. Email: [email protected]. Provenance and Peer Review: This article was commissioned by the editorial office, Quantitative Imaging in Medicine and Surgery. The article did not undergo external peer review. Comment on: Kliemann D, Adolphs R, Tyszka JM, Fischl B, Yeo BTT, Nair R, Dubois J, Paul LK. Intrinsic Functional Connectivity of the Brain in Adults with a Single Cerebral Hemisphere. Cell Rep 2019;29:2398-407.e4. Submitted Apr 09, 2020. Accepted for publication Apr 22, 2020. doi: 10.21037/qims-20-554 View this article at: http://dx.doi.org/10.21037/qims-20-554 Cerebral hemispherectomy, or surgical removal of an entire Functional hemispherectomy is a procedure in which the hemisphere of the brain, is performed in cases of severe affected hemisphere is isolated by severing all connections and intractable epilepsy (1). Surprisingly, despite deficits to the functional hemisphere. Two of the patients including hemiparesis and hemianopsia post-surgery, studied by Kliemann and colleagues had undergone left patients are often able to recover a remarkable degree of hemispherectomy, and the remaining four had undergone cognitive and sensorimotor function in the long term using right hemispherectomy. the remaining hemisphere (2-4). The neural plasticity that An innovation of the study design was the inclusion underlies this functional recovery is a topic of ongoing of two healthy control cohorts for comparison. -

THE EFFECTS of HEMISPHERECTOMY on INTELLECTUAL FUNCTIONING in CASES of INFANTILE HEMIPLEGIA by JOHN Mcfle from the National Hospital, Queen Square, London
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.24.3.240 on 1 August 1961. Downloaded from J. Neurol. Neurosurg. Psychiat., 1961, 24, 240. THE EFFECTS OF HEMISPHERECTOMY ON INTELLECTUAL FUNCTIONING IN CASES OF INFANTILE HEMIPLEGIA BY JOHN McflE From the National Hospital, Queen Square, London The recent increase in the number of reports of In cases ofinfantile hemiplegia, on the other hand, results of hemispherectomy, after which the majority the changes reported are entirely different. Williams of patients show considerable clinical improvement, and Scott (1939) gave a brief description of a patient prompts an inquiry into the effects of this operation aged 20 years, who had suffered a left cerebral injury on the exercise of intellectual abilities, and their at the age of 3 weeks: removal of the damaged hemi- implications for the understanding of cerebral phere resulted in 'no apparent mental deterioration', organization. and two years later the patient was able to cooperate Until a decade ago, the operation was rarely intelligently as a subject in a physiological experi- performed, and then usually for the removal of ment. One of the four patients of Marshall and extensively infiltrating gliomata. Moreover, the Walker (1950) was a case of birth injury to the rightProtected by copyright. majority of these removals were of the right hemi- hemisphere; and it is interesting to note that in this sphere: of 16 cases collected by Mensh, Schwartz, patient speech was reported to be more retarded in Matarazzo, and Matarazzo (1952), only one, that of development than was walking. It was Krynauw Zollinger (1935), was of a left hemisphere. -

Upper Limb Movement After Hemispherectomy
Upper Limb Movement After Hemispherectomy David Robert Henry Nobbs UCL Thesis submitted for the degree of DOCTOR OF PHILOSOPHY 1 I, David Robert Henry Nobbs, confirm the work presented in this thesis is my own. Where information has been derived from other sources, I confirm this has been indicated in the thesis. 1st March 2018 Signed: ................................. Date: ........................................ 2 Abstract Hemispherectomy is a surgical procedure for treating intractable epilepsy, involving the removal or disconnection of a cerebral hemisphere. Prior to surgery, patients have weakness along one side of their body and disruptions to their motor control. These impairments can be further exacerbated by the operation. This thesis provides an investigation into upper limb movement after surgery in terms of gross motor control and ipsilateral descending motor pathways for distal function. A neurophysiological assessment was used to identify the pathway driving the distal muscles of the paretic upper limbs. The results support the findings of previous studies that suggest superior function is likely to be dependent on a common, branching corticospinal pathway to the left and right sides. In addition, one patient without evidence of a common pathway had some use of the paretic wrist suggesting the presence of a distinct ipsilesional – possibly corticoreticulospinal – pathway. Upper limb kinematics during functional unimanual and bimanual reaching was also assessed. Unimanual deficits were identified and abnormalities in inter-limb coordination were found. These include a tendency to perform bimanual reaches as sequential unimanual reaches and reduced spatial interference in the trajectories of the two limbs. Whilst there were significant differences between the comparison and patient groups for these measures, there was also significant variance between the patients, underlining the heterogeneity of this cohort.