Back Pain and Common Musculoskeletal Problems
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-
Olecranon Bursitis
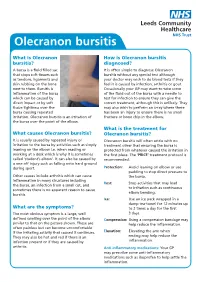
Olecranon bursitis What is Olecranon How is Olecranon bursitis bursitis? diagnosed? A bursa is a fluid filled sac It is often simple to diagnose Olecranon that stops soft tissues such bursitis without any special test although as tendons, ligaments and your doctor may wish to do blood tests if they skin rubbing on the bone feel it is caused by infection, arthritis or gout. next to them. Bursitis is Occasionally your GP may want to take some inflammation of the bursa of the fluid out of the bursa with a needle to which can be caused by test for infection to ensure they can give the direct impact or by soft correct treatment, although this is unlikely. They tissue tightness over the may also wish to perform an x-ray where there bursa causing repeated has been an injury to ensure there is no small irritation. Olecranon bursitis is an irritation of fracture or bone chip in the elbow. the bursa over the point of the elbow. What is the treatment for What causes Olecranon bursitis? Olecranon bursitis? It is usually caused by repeated injury or Olecranon bursitis will often settle with no irritation to the bursa by activities such as simply treatment other that ensuring the bursa is leaning on the elbow i.e. when reading or protected from whatever caused the irritation in working at a desk which is why it is sometimes the first place. The ‘PRICE’ treatment protocol is called ‘student’s elbow’. It can also be caused by recommended: a one off injury such as falling onto hard ground during sport. -

OES Site Color Scheme 1
Nuisance Problems You will Grow to Love Thomas V Gocke, MS, ATC, PA-C, DFAAPA President & Founder Orthopaedic Educational Services, Inc. Boone, NC [email protected] www.orthoedu.com Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Faculty Disclosures • Orthopaedic Educational Services, Inc. Financial Intellectual Property No off label product discussions American Academy of Physician Assistants Financial PA Course Director, PA’s Guide to the MSK Galaxy Urgent Care Association of America Financial Intellectual Property Faculty, MSK Workshops Ferring Pharmaceuticals Consultant Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. 2 LEARNING GOALS At the end of this sessions you will be able to: • Recognize nuisance conditions in the Upper Extremity • Recognize nuisance conditions in the Lower Extremity • Recognize common Pediatric Musculoskeletal nuisance problems • Recognize Radiographic changes associates with common MSK nuisance problems • Initiate treatment plans for a variety of MSK nuisance conditions Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. all rights reserved. Inflammatory Response* When does the Inflammatory response occur: • occurs when injury/infection triggers a non-specific immune response • causes proliferation of leukocytes and increase in blood flow secondary to trauma • increased blood flow brings polymorph-nuclear leukocytes (which facilitate removal of the injured cells/tissues), macrophages, and plasma proteins to injured tissues *Knight KL, Pain and Pain relief during Cryotherapy: Cryotherapy: Theory, Technique and Physiology, 1st edition, Chattanooga Corporation, Chattanooga, TN 1985, p 127-137 Orthopaedic Educational Services, Inc. © 2016 Orthopaedic Educational Services, Inc. -

Sports Medicine Examination Outline
Sports Medicine Examination Content I. ROLE OF THE TEAM PHYSICIAN 1% A. Ethics B. Medical-Legal 1. Physician responsibility 2. Physician liability 3. Preparticipation clearance 4. Return to play 5. Waiver of liability C. Administrative Responsibilities II. BASIC SCIENCE OF SPORTS 16% A. Exercise Physiology 1. Training Response/Physical Conditioning a.Aerobic b. Anaerobic c. Resistance d. Flexibility 2. Environmental a. Heat b.Cold c. Altitude d.Recreational diving (scuba) 3. Muscle a. Contraction b. Lactate kinetics c. Delayed onset muscle soreness d. Fiber types 4. Neuroendocrine 5. Respiratory 6. Circulatory 7. Special populations a. Children b. Elderly c. Athletes with chronic disease d. Disabled athletes B. Anatomy 1. Head/Neck a.Bone b. Soft tissue c. Innervation d. Vascular 2. Chest/Abdomen a.Bone b. Soft tissue c. Innervation d. Vascular 3. Back a.Bone b. Soft tissue c. Innervation 1 d. Vascular 4. Shoulder/Upper arm a. Bone b. Soft tissue c. Innervation d. Vascular 5. Elbow/Forearm a. Bone b. Soft tissue c. Innervation d. Vascular 6. Hand/Wrist a. Bone b. Soft tissue c. Innervation d. Vascular 7. Hip/Pelvis/Thigh a. Bone b. Soft tissue c. Innervation d. Vascular 8. Knee a. Bone b. Soft tissue c. Innervation d. Vascular 9. Lower Leg/Foot/Ankle a. Bone b. Soft tissue c. Innervation d. Vascular 10. Immature Skeleton a. Physes b. Apophyses C. Biomechanics 1. Throwing/Overhead activities 2. Swimming 3. Gait/Running 4. Cycling 5. Jumping activities 6. Joint kinematics D. Pharmacology 1. Therapeutic Drugs a. Analgesics b. Antibiotics c. Antidiabetic agents d. Antihypertensives e. -

Brachial-Plexopathy.Pdf
Brachial Plexopathy, an overview Learning Objectives: The brachial plexus is the network of nerves that originate from cervical and upper thoracic nerve roots and eventually terminate as the named nerves that innervate the muscles and skin of the arm. Brachial plexopathies are not common in most practices, but a detailed knowledge of this plexus is important for distinguishing between brachial plexopathies, radiculopathies and mononeuropathies. It is impossible to write a paper on brachial plexopathies without addressing cervical radiculopathies and root avulsions as well. In this paper will review brachial plexus anatomy, clinical features of brachial plexopathies, differential diagnosis, specific nerve conduction techniques, appropriate protocols and case studies. The reader will gain insight to this uncommon nerve problem as well as the importance of the nerve conduction studies used to confirm the diagnosis of plexopathies. Anatomy of the Brachial Plexus: To assess the brachial plexus by localizing the lesion at the correct level, as well as the severity of the injury requires knowledge of the anatomy. An injury involves any condition that impairs the function of the brachial plexus. The plexus is derived of five roots, three trunks, two divisions, three cords, and five branches/nerves. Spinal roots join to form the spinal nerve. There are dorsal and ventral roots that emerge and carry motor and sensory fibers. Motor (efferent) carries messages from the brain and spinal cord to the peripheral nerves. This Dorsal Root Sensory (afferent) carries messages from the peripheral to the Ganglion is why spinal cord or both. A small ganglion containing cell bodies of sensory NCS’s sensory fibers lies on each posterior root. -

Piriformis Syndrome Is Overdiagnosed 11 Robert A
American Association of Neuromuscular & Electrodiagnostic Medicine AANEM CROSSFIRE: CONTROVERSIES IN NEUROMUSCULAR AND ELECTRODIAGNOSTIC MEDICINE Loren M. Fishman, MD, B.Phil Robert A.Werner, MD, MS Scott J. Primack, DO Willam S. Pease, MD Ernest W. Johnson, MD Lawrence R. Robinson, MD 2005 AANEM COURSE F AANEM 52ND Annual Scientific Meeting Monterey, California CROSSFIRE: Controversies in Neuromuscular and Electrodiagnostic Medicine Loren M. Fishman, MD, B.Phil Robert A.Werner, MD, MS Scott J. Primack, DO Willam S. Pease, MD Ernest W. Johnson, MD Lawrence R. Robinson, MD 2005 COURSE F AANEM 52nd Annual Scientific Meeting Monterey, California AANEM Copyright © September 2005 American Association of Neuromuscular & Electrodiagnostic Medicine 421 First Avenue SW, Suite 300 East Rochester, MN 55902 PRINTED BY JOHNSON PRINTING COMPANY, INC. ii CROSSFIRE: Controversies in Neuromuscular and Electrodiagnostic Medicine Faculty Loren M. Fishman, MD, B.Phil Scott J. Primack, DO Assistant Clinical Professor Co-director Department of Physical Medicine and Rehabilitation Colorado Rehabilitation and Occupational Medicine Columbia College of Physicians and Surgeons Denver, Colorado New York City, New York Dr. Primack completed his residency at the Rehabilitation Institute of Dr. Fishman is a specialist in low back pain and sciatica, electrodiagnosis, Chicago in 1992. He then spent 6 months with Dr. Larry Mack at the functional assessment, and cognitive rehabilitation. Over the last 20 years, University of Washington. Dr. Mack, in conjunction with the Shoulder he has lectured frequently and contributed over 55 publications. His most and Elbow Service at the University of Washington, performed some of the recent work, Relief is in the Stretch: End Back Pain Through Yoga, and the original research utilizing musculoskeletal ultrasound in order to diagnose earlier book, Back Talk, both written with Carol Ardman, were published shoulder pathology. -

An Unusual Klebsiella Septic Bursitis Mimicking a Soft Tissue Tumor
Case Report Eur J Gen Med 2013;10(1):47-50 An Unusual Klebsiella Septic Bursitis Mimicking a Soft Tissue Tumor Mehmet Ali Acar1, Nazım Karalezli2, Ali Güleç3 ABSTRACT Because of its subcutaneous location prepatellar bursitis is frequently complicated by an infection. Gram-positive organisms, primarily Staphylococcus aureus account for the majority of cases of septic bursitis. Local cutaneous trauma can lead to direct inoculation of the bursa with normal skin flora in patients with occupations, such as mechanics, carpenters and farmers. A 71-year- old male was admitted to our department with a history of pain and swelling of his right knee over a 20 year period. Physical examination revealed a swollen, suppurative mass with ulceration of the skin and local erythema which mimicked a soft tissue tumor at first sight. Magnetic resonance imaging of the knee revealed a 13*12*10cm well-circumscribed, septated, capsulated, fluid-filled prepatellar bursa without evidence of tendinous or muscular invasion. The mass was excised en bloc, including the bursa and the overlying skin. The defect was closed with a split thickness skin graft. The patient had 100 degrees flexion and full extension after 45 days postoperatively, and he continued to work as a farmer. Key words: Klebsiella, septic bursitis, haemorrhage, mass Yumuşak Doku Tümöre Benzeyen Nadir Klebsiella Septik Bursiti ÖZET ilt altı yerleşiminden dolayı prepatellar bursitlerde enfeksiyon görülmesi sık olur. Gram pozitif mikroorganizmalar, özellikle stafilokokkus aureus en sık etkendir. Tamirciler, halıcılar ve çiftçiler gibi travmaya çok maruz kalan meslek gruplarında direk olarak etken cilt florasından bursaya ulaşabilir. 71 yaşında erkek hasta 20 yılı aşan ağrı ve şişlik nedeni ile kliniğimize başvurdu. -
The Efficacy and Safety of Gabapentin in Carpal Tunnel Patients: Open Label Trial
Original Article The efficacy and safety of gabapentin in carpal tunnel patients: Open label trial A. Kemal Erdemoglu Ayhan Varlibas, Kirikkale University, Faculty of Medicine, Department of Neurology, Kirikkale, 07100, Turkey Abstract Background: Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy caused by median nerve compression at the wrist. It results in loss of considerable man days and the effectiveness the various treatment modalities are still debated. Aim: To study the efficacy of gabapentin in patients with CTS. The study aim is to investigate the efficacy of gabapentin in patients with CTS patients who were refractory to the other conservative measures or unwilling for the surgical procedure. Materials and Methods: Forty one patients diagnosed as idiopathic CTS were included in the study. Patients were assessed with symptom severity scale (SSS) and functional status scale (FSS) scores of Boston Carpal Tunnel Questionnaire (BCTQ) before and at 1, 3, and 6 months of the treatment. Response to therapy was determined by using SSS and FSS scores of Address for correspondence: BCTQ. Results: The median dosage of gabapentin was 1800 mg/daily. Side effects Dr. A. Kemal Erdemoglu were mild and transient. There was a statistically significant difference in both symptom Kirikkale University, Faculty of Medicine, SSS and FSS scores between before and after treatment in patient groups at the end Department of Neurology, of six months (P < 0.001). According to grading the changes in subscales of BCTQ, Kirikkale, 07100, TURKEY. of 41 patients, 34.1 and 29.3 had a ≥ 40% decrease in SSS and FSS, respectively. E-mail: [email protected] Conclusion: Gabapentin was found to be partially effective and safe in symptomatic treatment of CTS patients. -

Wrist and Hand Examina[On
Wrist and Hand Examinaon Daniel Lueders, MD Assistant Professor Physical Medicine and Rehabilitaon Objecves • Understand the osseous, ligamentous, tendinous, and neural anatomy of the wrist and hand • Outline palpable superficial landmarks in the wrist and hand • Outline evaluaon of and differen.aon between nerves to the wrist and hand • Describe special tes.ng of wrist and hand Wrist Anatomy • Radius • Ulna • Carpal bones Wrist Anatomy • Radius • Ulna • Carpal bones Wrist Anatomy • Radius • Ulna • Carpal bones Wrist Anatomy • Radius • Ulna • Carpal bones Inspec.on • Ecchymosis • Erythema • Deformity • Laceraon Inspec.on • Common Finger Deformies • Swan Neck Deformity • Boutonniere Deformity • Hypertrophic nodules • Heberden’s, Bouchard’s Inspec.on • Swan Neck Deformity • PIP hyperextension, DIP flexion • Pathology is at PIP joint • Insufficiency of volar/palmar plate and suppor.ng structures • Distally, the FDP tendon .ghtens from PIP extension causing secondary DIP flexion • Alternavely, extensor tendon rupture produces similar deformity Inspec.on • Boutonniere Deformity • PIP flexion, DIP hyperextension • Pathology is at PIP joint • Commonly occurs from insufficiency of dorsal and lateral suppor.ng structures at PIP joint • Lateral bands migrate volar/palmar, creang increased flexion moment • Results in PIP “buTon hole” effect dorsally Inspec.on • Nodules • Osteoarthri.c • Hypertrophic changes of OA • PIP - Bouchard’s nodule • DIP - Heberden’s nodule • Rheumatoid Arthri.s • MCP joints affected most • Distal radioulnar joint can also be affected -

ICD9 & ICD10 Neuromuscular Codes
ICD-9-CM and ICD-10-CM NEUROMUSCULAR DIAGNOSIS CODES ICD-9-CM ICD-10-CM Focal Neuropathy Mononeuropathy G56.00 Carpal tunnel syndrome, unspecified Carpal tunnel syndrome 354.00 G56.00 upper limb Other lesions of median nerve, Other median nerve lesion 354.10 G56.10 unspecified upper limb Lesion of ulnar nerve, unspecified Lesion of ulnar nerve 354.20 G56.20 upper limb Lesion of radial nerve, unspecified Lesion of radial nerve 354.30 G56.30 upper limb Lesion of sciatic nerve, unspecified Sciatic nerve lesion (Piriformis syndrome) 355.00 G57.00 lower limb Meralgia paresthetica, unspecified Meralgia paresthetica 355.10 G57.10 lower limb Lesion of lateral popiteal nerve, Peroneal nerve (lesion of lateral popiteal nerve) 355.30 G57.30 unspecified lower limb Tarsal tunnel syndrome, unspecified Tarsal tunnel syndrome 355.50 G57.50 lower limb Plexus Brachial plexus lesion 353.00 Brachial plexus disorders G54.0 Brachial neuralgia (or radiculitis NOS) 723.40 Radiculopathy, cervical region M54.12 Radiculopathy, cervicothoracic region M54.13 Thoracic outlet syndrome (Thoracic root Thoracic root disorders, not elsewhere 353.00 G54.3 lesions, not elsewhere classified) classified Lumbosacral plexus lesion 353.10 Lumbosacral plexus disorders G54.1 Neuralgic amyotrophy 353.50 Neuralgic amyotrophy G54.5 Root Cervical radiculopathy (Intervertebral disc Cervical disc disorder with myelopathy, 722.71 M50.00 disorder with myelopathy, cervical region) unspecified cervical region Lumbosacral root lesions (Degeneration of Other intervertebral disc degeneration, -

Carpal Tunnel Syndrome: a Review of the Recent Literature I
The Open Orthopaedics Journal, 2012, 6, (Suppl 1: M8) 69-76 69 Open Access Carpal Tunnel Syndrome: A Review of the Recent Literature I. Ibrahim*,1, W.S. Khan1, N. Goddard2 and P. Smitham1 1University College London Institute of Orthopaedics and Musculoskeletal Sciences, Royal National Orthopaedic Hospital, Brockley Hill, Stanmore, HA7 4LP, UK 2 Department of Trauma & Orthopaedics, Royal Free Hospital, Pond Street, London, NW3 2QG, UK Abstract: Carpal Tunnel Syndrome (CTS) remains a puzzling and disabling condition present in 3.8% of the general population. CTS is the most well-known and frequent form of median nerve entrapment, and accounts for 90% of all entrapment neuropathies. This review aims to provide an overview of this common condition, with an emphasis on the pathophysiology involved in CTS. The clinical presentation and risk factors associated with CTS are discussed in this paper. Also, the various methods of diagnosis are explored; including nerve conduction studies, ultrasound, and magnetic resonance imaging. Keywords: Carpal tunnel syndrome, median nerve, entrapment neuropathy, pathophysiology, diagnosis. WHAT IS CARPAL TUNNEL SYNDROME? EPIDEMIOLOGY First described by Paget in 1854 [1], Carpal Tunnel CTS is the most frequent entrapment neuropathy [2], Syndrome (CTS) remains a puzzling and disabling condition believed to be present in 3.8% of the general population [14]. 1 commonly presented to Rheumatologists and Orthopaedic in every 5 subjects who complains of symptoms such as pain, Hand clinicians. It is a compressive neuropathy, which is numbness and a tingling sensation in the hands is expected to defined as a mononeuropathy or radiculopathy caused by have CTS based on clinical examination and electrophysio- mechanical distortion produced by a compressive force [2]. -

Download Versus Arthritis
Elbow pain Elbow pain information booklet Contents How does the elbow work? 4 What causes elbow pain and stiffness? 6 Should I see a healthcare professional? 8 What can I do to help myself? 9 How are elbow problems diagnosed? 12 What treatments are there for elbow pain? 14 Specific elbow conditions 18 Glossary 26 Research and new developments 27 Keeping active with elbow pain 28 Where can I find out more? 32 We’re the 10 million people living with arthritis. We’re the carers, researchers, health professionals, friends and parents all united in Talk to us 33 our ambition to ensure that one day, no one will have to live with the pain, fatigue and isolation that arthritis causes. We understand that every day is different. We know that what works for one person may not help someone else. Our information is a collaboration of experiences, research and facts. We aim to give you everything you need to know about your condition, the treatments available and the many options you can try, so you can make the best and most informed choices for your lifestyle. We’re always happy to hear from you whether it’s with feedback on our information, to share your story, or just to find out more about the work of Versus Arthritis. Contact us at [email protected] Words shown are explained in the glossary on p.26. Registered office: Versus Arthritis, Copeman House, St Mary’s Gate, Chesterfield S41 7TD in bold Registered Charity England and Wales No. 207711, Scotland No. SC041156. -

Chapter 30 When It Is Not Cervical Radiculopathy: Thoracic Outlet Syndrome—A Prospective Study on Diagnosis and Treatment
Chapter 30 When it is Not Cervical Radiculopathy: Thoracic Outlet Syndrome—A Prospective Study on Diagnosis and Treatment J. Paul Muizelaar, M.D., Ph.D., and Marike Zwienenberg-Lee, M.D. Many neurosurgeons see a large number of patients with some type of discomfort in the head, neck, shoulder, arm, or hand, most of which are (presumably) cervical disc problems. When there is good agreement between the history, physical findings, and imaging (MRI in particular), the diagnosis of cervical disc disease is easily made. When this agreement is less than ideal, we usually get an electromyography (EMG), which in many cases is sufficient to confirm cervical radiculopathy or establish another diagnosis. However, when an EMG does not provide too many clues as to the cause of the discomfort, serious consideration must be given to other painful syndromes such as thoracic outlet syndrome (TOS) and some of its variants, occipital or C2 neuralgia, tumors of or affecting the brachial plexus, and orthopedic problems of the shoulder (Table 30.1). Of these, TOS is the most controversial and difficult to diagnose. Although the neurosurgeons Adson (1–3) and Naffziger (10,11) are well represented as pioneers in the literature on TOS, this condition has received only limited attention in neurosurgical circles. In fact, no original publication in NEUROSURGERY or the Journal of Neurosurgery has addressed the issue of TOS, except for an overview article in NEUROSURGERY (12). At the time of writing of this paper, two additional articles have appeared in Neurosurgery: one general review article and another strictly surgical series comprising 33 patients with a Gilliatt-Sumner hand (7).