Sailing Injuries: a Review of the Literature
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-
Team Portraits Emirates Team New Zealand - Defender
TEAM PORTRAITS EMIRATES TEAM NEW ZEALAND - DEFENDER PETER BURLING - SKIPPER AND BLAIR TUKE - FLIGHT CONTROL NATIONALITY New Zealand HELMSMAN HOME TOWN Kerikeri NATIONALITY New Zealand AGE 31 HOME TOWN Tauranga HEIGHT 181cm AGE 29 WEIGHT 78kg HEIGHT 187cm WEIGHT 82kg CAREER HIGHLIGHTS − 2012 Olympics, London- Silver medal 49er CAREER HIGHLIGHTS − 2016 Olympics, Rio- Gold medal 49er − 2012 Olympics, London- Silver medal 49er − 6x 49er World Champions − 2016 Olympics, Rio- Gold medal 49er − America’s Cup winner 2017 with ETNZ − 6x 49er World Champions − 2nd- 2017/18 Volvo Ocean Race − America’s Cup winner 2017 with ETNZ − 2nd- 2014 A class World Champs − 3rd- 2018 A class World Champs PATHWAY TO AMERICA’S CUP Red Bull Youth America’s Cup winner with NZL Sailing Team and 49er Sailing pre 2013. PATHWAY TO AMERICA’S CUP Red Bull Youth America’s Cup winner with NZL AMERICA’S CUP CAREER Sailing Team and 49er Sailing pre 2013. Joined team in 2013. AMERICA’S CUP CAREER DEFINING MOMENT IN CAREER Joined ETNZ at the end of 2013 after the America’s Cup in San Francisco. Flight controller and Cyclor Olympic success. at the 35th America’s Cup in Bermuda. PEOPLE WHO HAVE INFLUENCED YOU DEFINING MOMENT IN CAREER Too hard to name one, and Kiwi excelling on the Silver medal at the 2012 Summer Olympics in world stage. London. PERSONAL INTERESTS PEOPLE WHO HAVE INFLUENCED YOU Diving, surfing , mountain biking, conservation, etc. Family, friends and anyone who pushes them- selves/the boundaries in their given field. INSTAGRAM PROFILE NAME @peteburling Especially Kiwis who represent NZ and excel on the world stage. -

RS100, and Thank You for Choosing an RS Product
R I G G I N G G U I D E Sail it. Live it. Love it. CONTENTS 1. INTRODUCTION 2. COMMISSIONING 2.1 Preparation 2.2 Rigging the Mast 2.3 Stepping the Mast 2.4 Rigging the Boom 2.5 Hoisting the Mainsail 2.6 Rigging the Gennaker 2.7 Attaching sail numbers 2.8 Completion 3. SAILING HINTS 3.1 Tacking 3.2 Gybing (mainsail only) 3.3 Sailing With the Assymetric Spinnaker 4. TUNING GUIDE 5. MAINTENANCE 5.1 Boat care 5.2 Foil care 5.3 Spar care, and access to bowsprit. 5.4 Sail care 6. WARRANTY 7. APPENDIX 7.1 Useful Websites and Recommended Reading 7.2 Three Essential Knots All terms highlighted in blue throughout the Manual can be found in the Glossary of Terms Warnings, Top Tips, and Important Information are displayed in a yellow box. 1. INTRODUCTION Congratulations on the purchase of your new RS100, and thank you for choosing an RS product. We are confident that you will have many hours of great sailing and racing in this truly excellent design. The RS100 is an exciting boat to sail and offers fantastic performance. This manual has been compiled to help you to gain the maximum enjoyment from your RS100, in a safe manner. It contains details of the craft, the equipment supplied or fitted, its systems, and information on its safe operation and maintenance. Please read this manual carefully and be sure that you understand its contents before using your RS100. This manual will not instruct you in boating safety or seamanship. -
Creating Future Generations of Champions
Skiff Regatta Featuring 49er US National Championship 29erxx US National Championship August 5-7, 2011 Columbia Gorge Racing Association, Cascade Locks, Oregon Notice of Race 1. Rules 1.1. The regatta will be governed by the Racing Rules of Sailing (RRS), the prescriptions of the United States Sailing Association (US SAILING), the rules of the participating Class Associations and this Notice of Race, except as any of these are changed by the Sailing Instructions or any appendices to the Sailing Instructions. 1.2. The organizing authority is the Columbia Gorge Racing Association. 2. Eligibility and Entry 2.1. The Regatta is open to I-14, 29erXX, and 49er class boats. 2.2. The 29erXX and 49er US National Championships are open to all boats that meet the obligations of the Class Rules and the governing National Authority. Participants in the 29erXX and 49er classes must be current members of their respective, recognized national class association. 2.3. Eligible boats may enter by completing the entry form on line at www.cgra.org and paying the appropriate, non-refundable entry fee as directed in the on-line registration instructions. 2.4. Crew substitution of the registered sailors is not permitted except with the permission of the Race Chairman. 2.5. All participants (or their parent/guardian is under age 18) will be required to sign and submit a waiver of liability before competing in the regatta. 3. Classification 3.1. This event is open to sailors of all classifications as described in the ISAF Regulation 22, ISAF Sailor Classification Code. 4. -

Safety and Rescue
SAFETY AND RESCUE Ventilation and Fueling everyone on your boat knows the location of the fire the tide changes direction is known as “slack water.” extinguisher and its use. Operation of a fire extinguish- “High tide” is the highest level a tide reaches during Gasoline fumes are heavier than air and will er is rather simple. Just remember PASS. ascending waters, and “low tide” is the lowest level a settle to the lowest part of the boat’s interior hull, tide reaches during descending waters. the bilge. All motorboats, except open boats, must The tidal cycle is the high tide followed approxi- have at least two ventilator ducts with cowls (intake Running Aground mately 6 hours later by low tide (two highs and two and exhaust). Exhaust blowers are part of most boat Keep a sharp lookout when traveling on waters lows per day). The tidal range is the vertical distance ventilation systems. Permanently installed fuel that have shallow areas to avoid running aground. between high and low tides. The tidal range varies tanks must be vented. Navigational charts, buoys, and depth finders can from 1 to 11 feet in Pennsylvania on the Delaware Most boat explosions occur from improper fuel- assist in this task. If you run aground and the impact River. Boaters should consult tide tables for times of ing. Portable gas tanks should be filled on the dock does not appear to cause a leak, follow these steps to high and low tides. or pier, not on board. The vent on the tank should refloat the boat: be closed and the gas pumped carefully, maintain- • Do not put the boat in reverse. -

Cruising History
Portland Yacht Club A History of Cruising Activity The Portland Yacht Club traces its routes to a weekend cruise to Boothbay Harbor by several Portlanders in the mid 1860's. This venture was the impetus that began a discussion about forming a yacht club. This was followed by a meeting in June 1868, at which time they decided if they could sign 100 members they would move forward. On April 26, 1869 their initiative was rewarded with the creation of the Portland Yacht Club. During the first year, the club held another cruise to Boothbay Harbor. Departing Boothbay, they went up the Sasanoa (hopefully with the tide) to Bath. The next day they sailed down the Kennebec River (again hopefully with a fair tide) to Jewel Island where “a Grand Clam Bake” was held. The entire three day cruise was enshrouded in fog and supposedly continued for the next 34 years (some things never change). But, think of the seamanship and navigation skills required to ply those waters in a vessel with no power other than the wind while using less than reliable charts, compass, watch and taffrail log. Present day cruisers are now quite spoiled with the electronics available. In 1873 the club held both a spring and fall cruise along with 30 boats participating in Portland's July 4th Celebration. The spring cruise of 1879 included 4 schooners and 2 sloops. They departed the club at 1000 and arrived in Wiscasset at 1620. The sloop Vif went aground on Merrill's Ledge in the Sheepscot. As the saying goes, “There are two types of sailors in Maine, those that have been aground and those that will go aground”. -
2020 Fall Dinghy Series Notice of Race
“2020 Beaufort Yacht & Sailing Club Fall Dinghy Series” Sept 7 thru Nov 1, 2020 NOTICE OF RACE 1 RULES 1.1 The regatta will be governed by the rules as defined in The Racing Rules of Sailing. 2 SAFETY 2.1 Life jacket and shoes are required for each sailor. Juniors are required to wear life jackets while sailing. 2.2 It is anticipated that Covid 19 safety precautions will still be in place and you are expected to follow the Beaufort County Face Mask Ordinance as well as CDC recommendations. An informal social time with refreshments may be organized for after the races and/or at awards, but everyone is responsible for their own safety, including self distancing. Masks are optional while racing, but are required to be worn on shore in those situations which inherently put people within 6 feet of fellow attendees. If you are not comfortable with the social arrangements it is your responsibility to avoid the social gatherings. 2.3 US Sailing, South Atlantic Yacht Racing Association and BYSC recommend singlehanded sailing or family sailing during the Covid 19 Pandemic. The safety and health of each member (or participant, or sailor) is the responsibility of the individual member (or participant, or sailor). 2.4 The signal boat will be minimally staffed due to social distancing guidelines. Competitors are requested to take this into consideration during the course of events. 3 ELIGIBILITY AND ENTRY 3.1 The regatta is open to one-design dinghy classes. The Regatta is only open to BYSC members and students of BCSB. -
An Introduction to Canoeing/Kayaking a Teaching Module
An Introduction to Canoeing/Kayaking A Teaching Module Iowa Department of Natural Resources Des Moines, Iowa This information is available in alternative formats by contacting the DNR at 515/725-8200 (TYY users – contact Relay Iowa, 800/735-7942) or by writing the DNR at 502 East 9th Street, Des Moines, IA 50319-0034. Equal Opportunity Federal regulations prohibit discrimination on the basis of race, color, national origin, sex or handicap. State law prohibits discrimination on the basis of race, color, creed, sex, sexual orientation, gender identity, religion, national origin, or disability. If you believe you have been discriminated against in any program, activity, or facility as described above, or if you desire further information, please write to the Iowa DNR, Wallace State Office Building, 502 E. 9th Street, Des Moines, IA 50319-0034. Funding: Support for development of these materials was provided through Fish and Wildlife Restoration funding. Table of Contents Introduction ....................................................................................................................................1 Objectives........................................................................................................................................1 Materials .........................................................................................................................................1 Module Overview ...........................................................................................................................1 -
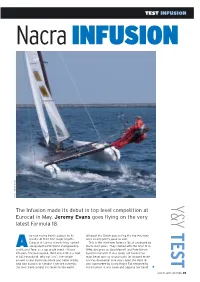
Yachts Yachting Magazine NACRA F18 Infusion Test.Pdf
TEST INFUSION Nacra INFUSION S N A V E Y M E R E J O T O H P Y The Infusion made its debut in top level competition at & Eurocat in May. Jeremy Evans goes flying on the very latest Formula 18. Y T ny new racing boat is judged by its although the Dutch guys racing the top Infusions results. At their first major regatta — were clearly pretty good as well. Eurocat in Carnac in early May, ranked This is the third new Formula 18 cat produced by E A alongside the F18 World championship Nacra in 10 years. They started with the Inter 18 in and Round Texel as a top grade event — Nacra 1996, designed by Gino Morrelli and Pete Melvin S Infusions finished second, third and sixth in a fleet based in the USA. It was quick, but having the of 142 Formula 18. Why not first? The simple main beam and rig so unusually far forward made answer is that Darren Bundock and Glenn Ashby, it tricky downwind. Five years later, the Inter 18 T who won Eurocat in a Hobie Tiger are currently was superseded by a new Nacra F18 designed by the most hard-to-beat cat racers in the world, Alain Comyn. It was quick and popular, but could L YACHTS AND YACHTING 35 S N A V E Y M E R E J S O T O H P Above The Infusion’s ‘gybing’ daggerboards have a thicker trailing edge at the top, allowing them to twist in their cases and provide extra lift upwind. -

Caribbean Compass Yachting Magazine
C A R I B B E A N On-line C MPASS NOVEMBER 2017 NO. 266 The Caribbean’s Monthly Look at Sea & Shore PLANNING FOR A SEASON OF FUN! Story on page 27 TIM WRIGHT / WWW.PHOTOACTION.COM NOVEMBER 2017 CARIBBEAN COMPASS PAGE 2 ART ROSS The Caribbean’s Monthly Look at Sea & Shore www.caribbeancompass.com NOVEMBER 2017 • NUMBER 266 CHRIS DOYLE FLYING BUZZARD FRIENDS WWW.CARNAVALDEBARRANQUILLA.ORG DEPARTMENTS Info & Updates ......................4 Look Out For… ......................38 Business Briefs .......................8 Readers’ Forum .....................39 Eco-News .............................. 12 What’s On My Mind ..............41 Regatta News........................ 14 Caribbean Market Place .....42 Y2A ......................................... 20 Calendar of Events ...............45 Regatta Updates Island Poets ...........................34 Meridian Passage .................45 Storms don’t stop the show .. 14 Book Reviews ........................35 Classified Ads ....................... 46 The Caribbean Sky ...............36 Advertisers Index ..................46 NOVEMBER 2017 CARIBBEAN COMPASS PAGE 3 Youth Sailing Caribbean Compass is published monthly by Compass Publishing Ltd., The Valley, P.O. Box 727, Anguilla, British West Indies. Taking on new meaning ........20 Plan for a Tel: (784) 457-3409, Fax: (784) 457-3410, [email protected], www.caribbeancompass.com Publisher..................................Tom Hopman Art, Design & Production.........Wilfred Dederer Fun Season [email protected] [email protected] -

I Feel the Need…
44 AUSTRALIAN SAILING AUGUST-SEPTEMBER 2017 MYSAILING.COM.AU 45 SPORTSBOATS BETH MORLEY SPORTSAILINGPHOTOGRAPHY.COM SPORTS BOATS I FEEL THE NEED… ANDREW YORK LOOKS AT THE DEVELOPMENT OF SPORTSBOATS AND HOW THEY NEED TO BE SAILED IT was in the early years of this century that sports boats broke away from their trailer-sailer forebears. A more competitive group of owners started adding sail area and stripping out accommodation from their boats. Most people’s perception of a sports boat is a trailerable sailing boat with masses of sail area. While this was the genesis of sports boats there has been a gradual change. It became evident that sports boats needed to form their own separate group. ASBA was founded in 2007 by Cameron Rae, Mark Roberts and Richard Parkes. They wanted a more scientific handicapping system than had been employed in the past. In 2008 the Sportsboat Measurement System (SMS) was put in place by a body independent to ASBA. It was created by the same people who formulated the Australian Measurement System (AMS) in 1997. Sports boat racing has flourished across Australia under the ASBA banner, with the SMS rule encouraging high performance designs without the penalties that existed under other systems. Large asymmetrical spinnakers, in particular, are not penalised as harshly in the rating as the working sail area is, so that is why you see the sports boats with clouds of sails downwind. In Australia sports boats are defined as being between 5.8m and 8.5m in length and no more than 3.5m wide including hiking racks. -

Sailing Instructions
Verve Inshore Regatta Chicago Yacht Club Belmont Harbor, Chicago, IL August 24-26, 2018 SAILING INSTRUCTIONS Abbreviations [SP] Rules for which a standard penalty may be applied by the race committee without a hearing or a discretionary penalty applied by the protest committee with a hearing. [DP] Rules for which the penalties are at the discretion of the protest committee. [NP] Rules that are not grounds for a protest or request for redress by a boat. This changes RRS 60.1(a) 1 RULES 1.1 The regatta will be governed by the rules as defined in The Racing Rules of Sailing. 1.2 Appendices T and V1 shall apply. 1.3 Class rules prohibiting the use of marine band radios and cellular telephones will not apply. All keelboats are required to carry an operating VHF marine-band radio while sailing in these events. This changes International Etchells class rule C.5.2(b)(8). 1.4 Class rules prohibiting GPS navigation devices will not apply. The following conditions will apply to the use of GPS navigation devices: When class rules prohibit the use of a GPS while racing, such a device may be used provided that it will be installed in a position or covered in such a way that no data may be taken from it while sailing. Data produced by such device may be viewed only at the dock or on shore. This changes International Etchells class rule C.5.1(b) and Shields class rule 10.9. 1.5 For the J/70 class only, J/70 Class Rules Part III I.3 (Support Boats) will apply. -

Setting up Your FD to Go Sailing
FD Trim Setting up your FD to go sailing The FD is a complex and powerful dinghy and getting the boat set up correctly for the prevailing conditions makes all the difference between the boat flying along and its being a pig to sail, especially to windward. It is important, therefore, that the significant controls are readily adjustable by the helmsman whilst sailing, so that he can fine tune the rig without loosing way or control. Of course, all the usual boat turning and preparation rules apply to the FD as to any other performance dinghy. Get the centreboard and rudder vertical and in line; get the mast central and upright in the boat; make the mast a tight fit in the step and partners etc. However some aspects of the FD are a bit special so try this way of sorting boat out and getting set for the race. Set up the genoa: The most important control of an FD is the genoa halyard, controlling the mast rake. This needs the purchase of at least 24:1 led to either side of the boat for the helmsman to adjust while hiking. A courser adjustment, say 6:1, is also ideal for changing between the different clew attachment positions available in modern genoas. We use a 6:1 purchase on the back face of the mast which hooks up to the genoa halyard. One end of this goes directly to a clam-cleat for the course adjustment and this marked with a position for each clew. The other end goes to 4:1 purchase running along the boats centreline and led to each side.