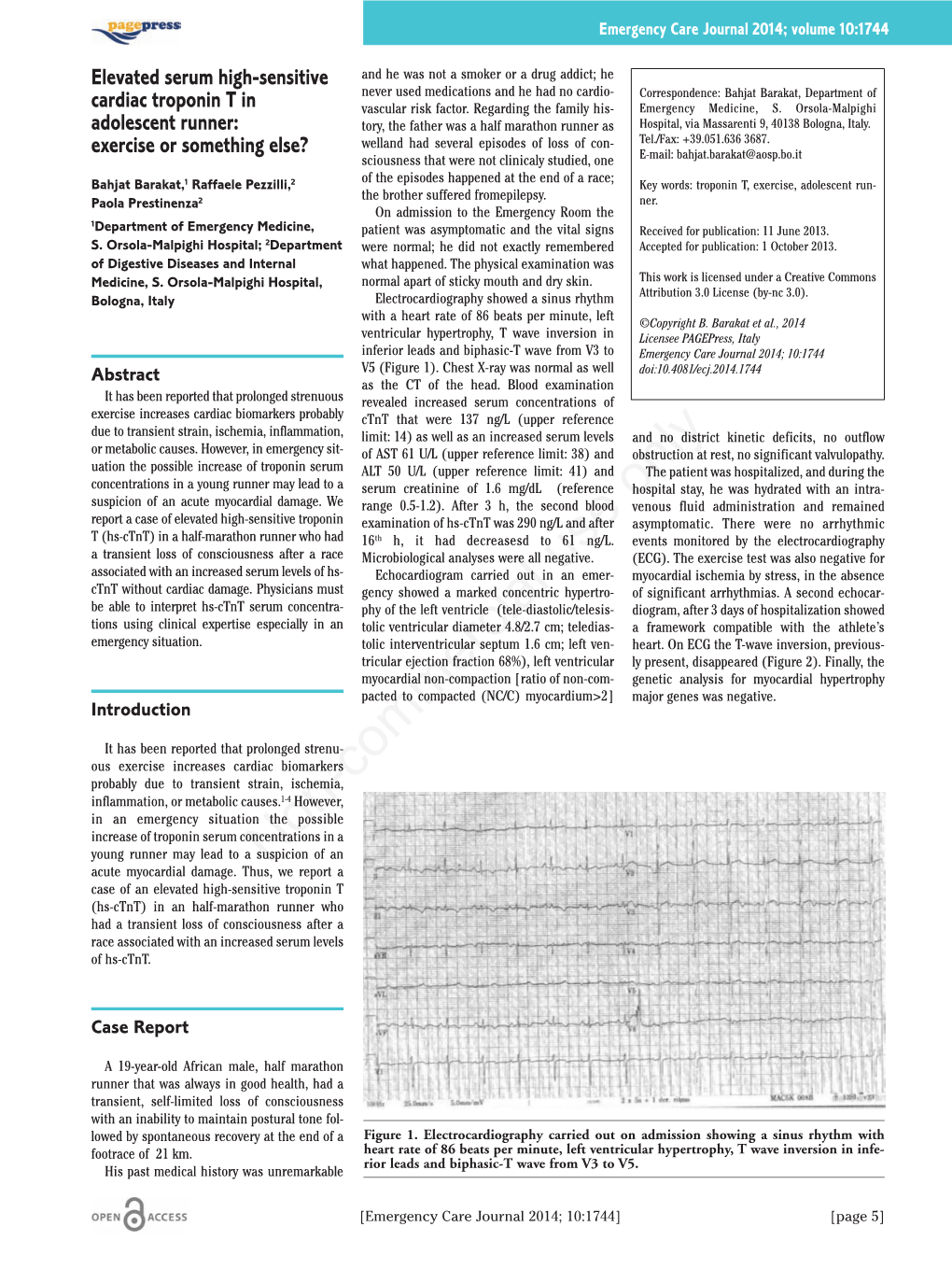
Elevated Serum High-Sensitive Cardiac Troponin T in Adolescent Runner
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Oollyymmppiiaannss
Olympians The University of Colorado has produced 60+ Olympians (through the 2008 Summer Games). The majority of the Olympians to come from the Boulder campus are former members of the Buffs’ esteemed ski teams, with alumni also competing in figure skating (2), bobsledding (1), equestrian (1), luge (3), basketball (3), cycling (1) while the following list of athletes have competed in track and field during the 20th Century. Ambassador David Bolen, Colorado’s first Olympian, finished fourth in the 400-m dash during the 1948 Summer Games in London, England. In his name, Colorado established the David Bolen Olympic Award in 1949, awarded to any current CU student-athlete who competes under the United States flag. Alan Culpepper Shayne (Wille) Culpepper Casey Malone Jenny Barringer Kara (Grgas-Wheeler) Goucher Billy Nelson Dathan Ritzenhein Jorge Torres 1948, The XIVth Olympiad, London, England 2000, The XXVIIth Olympiad, Sydney, Australia David Bolen (USA) .................................................................. 4th-400-m Hannah Cooper (Liberia) .................................................. 100-m Hurdles Alan Culpepper (USA) .............................................................. 10,000-m 1960, The XVIIth Olympiad, Rome, Italy Shayne (Wille) Culpepper (USA) ................................................ 1,500-m Ted Woods (USA) ............................................................. 1,600-m Relay Adam Goucher (USA) ......................................................... 13th-5,000-m 1968, The XIXth Olympiad, -

Diagnostic Testing JACC February 21, 2006
94A ABSTRACTS - Diagnostic Testing JACC February 21, 2006 POSTER SESSION 902-3 Prognostic Value of Regional Versus Global Measures 902 of Left Ventricular Function Following Myocardial Coming of Age: Echocardiography Infarction: The VALIANT Echo Study Jens Jakob Thune, Lars Kober, Marc A. Pfeffer, Hicham Skali, Nagesh Anavekar, Eric Sunday, March 12, 2006, 9:00 a.m.-12:30 p.m. J. Velazquez, Karen S. Pieper, Jalal K. Ghali, J. Malcolm O. Arnold, John J.V. McMurray, Georgia World Congress Center, Hall B1 Scott D. Solomon, Brigham and Women’s Hospital, Boston, MA, Duke Clinical Research Institute, Duke University Medical Center, Durham, NC Presentation Hour: 9:00 a.m.-10:00 a.m. Background: Left ventricular (LV) systolic function is an important predictor of outcome 902-1 Predictors of Death in Patients With Atrial Fibrillation: following myocardial infarction (MI). It is unclear whether measures of global or regional The Role of Echocardiography systolic function are better prognostic indicators following MI. Methods: We analyzed echocardiographic studies from 507 patients with LV systolic Yoko Miyasaka, Marion E. Barnes, Stephen S. Cha, Kent R. Bailey, Walter Abhayaratna, dysfunction (SD), heart failure (HF), or both following MI, from the VALIANT trial. We Lori A. Carlson, James B. Seward, Teresa S. M. Tsang, Mayo Clinic, Rochester, MN compared the predictive value of LV ejection fraction (EF), measured by the Simpson’s-rule method, with wall motion index (WMI) based on the American Society of Echocardiography Background: Atrial fibrillation (AF) independently confers mortality risk. We sought to 16-segment model. Endpoint was all-cause death or hospitalization for HF. -

Effects of Age and Gender on Physical Performance
Effects of age and gender on physical performance Vanina Bongard & Ann Y. McDermott & Gerard E. Dallal & Ernst J. Schaefer Lipid Metabolism, Tufts University Human Nutrition Research Center, 711 Washington Street, Boston, MA 02111, USA Abstract Our purpose was to examine the effects of in men and women at all ages, and the 1-year age- age and gender on physical performance. We assessed a related declines in performance were about twice as one-hour swimming performance and participation of great at 40 y and more than four-times as great at 80 y 4,271 presumably healthy men and women, aged 19– than at 20 y of age, with even greater age-related 91 years, from the 2001–2003 United States Masters declines in participation being noted for both men and Swimming long-distance (1 h) national competition. women. The decline in performance with increasing age was found to be quadratic rather than linear. The equation Keywords Aging . Physical performance . which best fit variation in 1 h swimming distance in Physical activity . Exercise . Swimming meters (m) according to variations in age in years (y) in men was: distance (m)=4058+2.18 age−0.29 age (http://www.acsmmsse.org/pt/re/msse/positionstan dards.htm;jsessionid=DiRVACC7YS3mq27s5kV3vw Introduction pEVSokmmD1ZJLC7pdnol3KcfoSu0t!1096311956! 949856145!9001!-1), with the same equation for Habitual exercise is able significantly and positively women except that 380 m needed to be subtracted to impact on health, and the Centers for Disease from the calculated value at all ages (about a 10% Control and Prevention and the American College of difference). -

Post Collegiate Success
POST COLLEGIATE SUCCESS Here at CU we are no more proud of the successes of present Buffs than we are of those who went on to the next level. Frankly, we don’t believe there is another college program in the country that can boast as many national level professionals. During the tenure of Coach Wetmore, numerous graduates of the Buff distance program have gone on to professional contracts. Seven are currently active. Ten have been Olympians and two have won Olympic Bronze Medals. Twenty-eight have made World Championship Track or Cross Country teams. Eighteen made World teams while still running for CU. It’s a tradition of excellence. RENEE METIVIER (‘05) ....................Distance EMMA COBURN (‘13) ....Mid Distance/Steeple Club ............................................... Mizuno Club .......................................New Balance • 2005 USATF Outdoor Championships (5th, 10k) • *2011 USA Steeplechase Champion • 2006 USA XC Championships (3rd, 4k), IAAF • *2011 IAAF World Championship Steeplechase World XC Championships (49th) Finalist (13th) • 2008 USA XC Championships (2nd), IAAF World • *2011 USA No. 1 Ranked Steeplechase XC Championships (49th) • *2012 USA Olympic Trials Steeplechase • 2008 USA Olympic Trials Qualifier (5k) Champion • 2010 USA XC Championships (5th), IAAF World • *2012 Olympic Games Steeplechase Finalist XC Championships (38th) (8th-highest American) • 2010 USA Indoor 3k Champion • *2012 USA No. 1 Ranked Steeplechaser • 2010 USA Outdoor Championships (8th, 5k) • 2014 USA No. 1 Ranked Steeplechaser • 2011 Bolder Boulder Team USA Member (6th) • 2014 Shanghai Golden Grand Prix (1st) • 2012 Chicago Marathon, 1st American, 7th • 2014 USA Steeplechase Champion overall (2:27.17) • 2014 Glasgow British Athletics Diamond • 2015 Bolder Boulder Elite Race participant League (2nd), broke the American record • 2016 U.S. -

Homeland Security Secretary Chertoff Visits Sandia, Speaks Highly of Labs
Homeland Security Secretary Chertoff visits Sandia, speaks highly of Labs’ antiterrorism technologies ‘We don’t need to reinvent the wheel,’ he says about national labs’ R&D resources By Bill Murphy Taking up Sen. Pete Domenici’s suggestion that he tour Sandia, Homeland Security Secretary Michael Chertoff said during a visit to the Labs last Friday that “it turned out to be good advice.” Chertoff spent a half day at the Labs to learn about Sandia’s capabilities, and received brief- ings on several specific Sandia-developed home- land security technologies and programs. The briefings came from new Labs President and Director Tom Hunter, other members of senior management, and several subject matter experts. Following the briefings, Chertoff, joined by Domenici, Rep. Heather Wilson, and Tom, con- ducted a half-hour news conference in the Bldg. 810 lobby to talk about the relationship between Sandia and the Department of Homeland Secu- rity. Representatives from most of the Albu- querque news media attended. Chertoff said he was impressed with what he had learned at Sandia and expressed a hope to spend more time at the Labs in the future. “There is a tremendous contribution [to homeland security] to be made here,” he said. He said the energy, the dedication, and the cre- ativity at Sandia “truly are remarkable.” The 21st century challenges in national WELCOME MR. SECRETARY— US Sen. Pete Domenici, left, praises new Homeland Security Secretary Michael security, Chertoff said, more and more will be Chertoff, right, during last Friday’s news conference at Sandia. With them is new Labs President and Director Tom Hunter, who hosted Chertoff. -

2018 Colorado Cross Country
2018 COLORADO CROSS COUNTRY DO NOT APPROACH THE BUFFALOES! These animals may appear tame, but are wild, unpredictable and dangerous. Buffaloes can weigh 2,000 pounds and can sprint at 30 mph, three times faster than you can run. INDEX COLORADO AT A GLANCE SPORTS INFORMATION Academics and Athletics ................... 93-97 Location .........................Boulder, Colo. (102,500) Cross Country Contact ...............Linda Sprouse All-Americans ................................... 64-65 Founded .......................................................1876 Office ...................................303/492-5980 Athlete Biographies ............................ 9-47 Enrollment .................................................32,220 Fax .......................................303/492-3811 Boulder/Denver Facts and Trivia ........ 98-99 Colors ................................. Silver, Gold and Black E-Mail [email protected] Coaching Staff ...........................................3 Nickname ...................................Buffaloes (Buffs) Internet .........................www.CUBuffs.com Conference History ..................................52 Home Course ............Buffalo Ranch at So Campus Twitter/Instagram ................ @cubuffstrack Head Coach Mark Wetmore .......................2 Distances ..................5,800-m (women), 8k (men) Facebook ..........facebook.com/cubuffstrack Honor Roll ......................................... 66-69 Elevation ..................... 5,435 feet above sea level Letterwinners, All-Time -

Emma Coburn — Have Combined for 19 NCAA Individual Cross Country, Indoor and Outdoor Championships
2011 COLORADO CROSS COUNTRY DO NOT APPROACH THE BUFFALOES! These animals may appear tame, but are wild, unpredictable and dangerous. Buff aloes can weigh 2,000 pounds and can sprint at 30 mph, three times faster than you can run. INDEX COLORADO AT A GLANCE SPORTS INFORMATION Academics and Athletics ................... 84-86 Location ...........................Boulder, Colo. (97,385) Cross Country Contact ....Linda Poncin Sprouse Coaching Staff ...........................................3 Founded .......................................................1876 Offi ce ...................................303/492-5980 All-Americans .........................................64 Enrollment .................................................29,952 Fax .......................................303/492-3811 Athlete Biographies ............................7-50 Colors ................................. Silver, Gold and Black E-Mail [email protected] Big 12 10th Anniversary Team .................82 Nickname ...................................Buff aloes (Buff s) Internet .........................www.CUBuff s.com Boulder/Denver Facts and Trivia ........ 87-88 Home Course ............Buff alo Ranch at So Campus Buff s vs. The Nation .................................56 Distances ..................5,800-m (women), 8k (men) PRACTICE SCHEDULE Conference History ..................................54 Elevation ..................... 5,435 feet above sea level Mondays ...................... 2 p.m. (Fieldhouse) Head Coach Mark Wetmore .......................2 -

N-Terminal Prob-Type Natriuretic Peptide (NT-Probnp)
Article in press - uncorrected proof Clin Chem Lab Med 2008;46(2):247–249 ᮊ 2008 by Walter de Gruyter • Berlin • New York. DOI 10.1515/CCLM.2008.024 2007/323 N-Terminal proB-type natriuretic peptide (NT-proBNP) concentrations in elite rugby players at rest and after active and passive recovery following strenuous training sessions Giuseppe Banfi1,2,*, Gianlodovico Melzi Keywords: athletes; N-terminal proB-type natriuretic D’Eril2,3, Alessandra Barassi2,3 and Giuseppe peptide (NT-proBNP); rugby. Lippi4 1 IRCCS Galeazzi, Milan, Italy Introduction 2 School of Medicine, University of Milan, Milan, Italy The serum biomarker N-terminal proB-type natriuretic 3 Ospedale S. Paolo, Milan, Italy peptide (NT-proBNP), the cleaved fragment of the pre- 4 School of Medicine, University of Verona, Verona, cursor of brain natriuretic peptide (amino acids 1–76), Italy is accepted as a parameter useful for evaluating and monitoring cardiac injury characterized by myocardial Abstract wall stress in association with additional instrumental and biochemical parameters. Strenuous exercise may Background: The serum biomarker N-terminal proB- generate transitory ischemia, myocardial stress and type natriuretic peptide (NT-proBNP), a cleaved frag- diastolic left ventricular dysfunction, often inducing ment of the brain natriuretic peptide (BNP) precursor an increase in biomarker concentrations commonly (amino acids 1–76), is accepted as a standard marker measured to determine heart anomalies (1). for evaluating and monitoring cardiac injury charac- Cardiac damage during marathon running has been terized by myocardial wall stress. Strenuous exercise described in 60 recreational athletes who participated may generate transitory ischemia, myocardial stress in the 2004 and 2005 Boston Marathon: 60% of rec- and diastolic left ventricular dysfunction, possibly reational runners showed increased troponin T after inducing increased concentrations of NT-proBNP. -

Kalamazoo Shufflers Marathon & Half
“Man Imposes his own limitations; don’t set any” -Anthony Bailey March 14, 2010 www.kalamazooarearunners.com The Kalamazoo Area Runners Rundownwsletter Contents Introduction Page 1 Hot Club News and Events Page 4 Easter Hash/Children’s East Treat Hunt March 20 Kal-Haven Trail Run Registration is now OPEN Boston Tea Party 4 Mile Fun Run and Dick Beardsley Presentation KAR Annual Banquet and Election Scheduled March 23 Join the Kalamazoo Area Runners Leadership Team Notification of Changes to By-Laws Sponsorship Opportunities Join KAR Team Pink for the Susan G. Komen Foundation Race for the Cure Club Series Races & Discounts - Page 11 The Boston Marathon is no doubt the most prestigious marathon in the The Shamrock 5k Kicks off Club Series March 20 world. I recall a story shared by fellow runners several years ago Borgess Run for the Health of IT April 23 & 24 regarding Anne Flynn, a past member of Kalamazoo Area Runners Rock n’ Roll Half Marathon Discount and the Battle Creek Road Runners. Anne had qualified for the Olympic Trials, and in discussing her phenomenal accomplishment, Community Events & Programs Page 13 14th Annual Wheel Run Together 10k, 5k the individual she was talking with was more interested in knowing whether she had run Boston. Well recognized by both runners and Group Runs & Training Programs Page 13 non-runners alike, Boston is the pinnacle of running achievement and Beyond Marathon Training Program aspiration. Perhaps it is a goal that for many recreational runners is SHufflers Marathon Training within reach, whereas the Olympics serves as an endeavor only the Borgess Run Camp elite few can aspire to. -

2013 Cross Country Media Guide.Indd
2013 COLORADO CROSS COUNTRY DO NOT APPROACH THE BUFFALOES! These animals may appear tame, but are wild, unpredictable and dangerous. Buff aloes can weigh 2,000 pounds and can sprint at 30 mph, three times faster than you can run. INDEX COLORADO AT A GLANCE SPORTS INFORMATION Academics and Athletics ................... 79-81 Location .........................Boulder, Colo. (102,500) Cross Country Contact ...............Linda Sprouse Coaching Staff ...........................................3 Founded .......................................................1876 Offi ce ...................................303/492-5626 All-Americans .........................................55 Enrollment .................................................29,884 Fax .......................................303/492-3811 Athlete Biographies ............................7-39 Colors ................................. Silver, Gold and Black E-Mail [email protected] Big 12 10th Anniversary Team .................77 Nickname ...................................Buff aloes (Buff s) Internet .........................www.CUBuff s.com Boulder/Denver Facts and Trivia ........ 82-84 Home Course ............Buff alo Ranch at So Campus Twitter ................................. @cubuff strack Buff s vs. The Nation ...........................46-47 Distances ..................5,800-m (women), 8k (men) Facebook ..........facebook.com/cubuff strack Conference History ..................................44 Elevation ..................... 5,435 feet above sea level Head Coach -

Summer, 2005 the SUN
Summer, 2005 THE SUN Your Board in “Actio n” Hot Running Fun in the Page 2 Summertime! By Ben Bensen Big Sur Marathon ! The last week in June was amazing, and Page 3 not just for its temperatures. The Lake Wyola Race celebrated its 25th Anniversary with a beautiful event, two new records and Following a small but de- an impressive turnout - 137 runners and The Power Gel from - termined group of walkers four walkers finished the event. Marjorie (Yes, it does rhyme!) (Above), runners line up, Page 4 Shearer of Greenfield won for the second then take off at the start time in 31:10, and Kent Lemme of Williams- of the 25th. Annual Lake town won the men’s race in 25:28. Susan Wyola Race (below). Wootton? Walker (41:23; Female Veteran, 50-59) and Yes, Wootton! Harry Masterton, Jr. (35:01; Senior Male, Page 5 60+), both of Shutesbury established new course records for their respective divisions. And the Coffee Club took the team title Boston Marathon again with a total of 140:31 for its top five & 1st. Cave Hill Classic runners (see http://www.wyolaroadrace.com) P ages 6 -7 ! Meanwhile, up on Northfield Mountain, international-class trail runners assembled Cross-Country with the hope of nabbing a spot on the U.S. Lives in NoHo! National Team by racing in the La Spportiva P ages 8-9 USATF NE Mountain Running Championship. The event was featured in an article by John Stifler in The Gazette (wwell worth reading - 30th. Holyoke it appeared on the 28th.), but several local St. -

KEEPING RACES SAFE: POLICE, EMS & RACE DIRECTORS Your Playlist Powers You Through Every Training Run
THE RUNNER’S SOURCE FOR THE DC AREA RUNWASHINGTON.COM WASHINGTONJUNE/JULY 2013 RUNNING FASTER AFTER A BREAKUP DC’S RUNNING BLOGGERS WILL RUN FOR CHICKEN KEEPING RACES SAFE: POLICE, EMS & RACE DIRECTORS Your playlist powers you through every training run. But on a Rock ‘n’ Roll race day, it’s time to channel some high-volume star power. It’s time for you to be cheered on by live bands and throngs of fans lining the streets. It’s time to lace up, glam up, and rock out. So pass the glitter. It’s showtime. Sign Up Today! VB_12_RunWashington_May_ad.indd 1 5/3/13 2:36 PM ©2013 New Balance Athletic Shoe,Balance Inc. New Athletic ©2013 The New Balance 1080v3. Featuring nitrogen-infused N2 foam for superior cushioning and a new lightweight Fantom Fit upper that cradles the midfoot, the 1080v3 takes smart to the next level. New Balance athletes Team Gen LaCaze and Beverly Ramos. NBLRUNP3068_C_v1a.indd 1 4/2/13 11:17 AM NBLRUNP3068 Date: 4/1/13 Version: 1 Page: 1 NBLRUNP3068_C_v1a 8.75x11.125” Ken NBX Women’s 1080 Performance 8.375x10.875” Anthony Amanda 8x10.5” Diane 7.5x10” 4c 100% Cover: Arlington County Police lead the runners at the 2011 Clarendon Day 10k. THE RUNNER’S SOURCE FOR THE DC AREA Photo: Brian Knight/ Swim Bike Run Photography WASHINGTON Editor’s PUBLISHER K. Dalby NOTE RunWashington LLC EDITOR IN CHIEF Charlie Ban CONTENTSJUNE/JULY 2013 Photo: Brian Knight/Swim Bike Run Photography [email protected] SENIOR EDITOR LETTERS TO THE EDITOR ................................... 4 Dickson Mercer [email protected] OFF THE BEATEN PATH ....................................