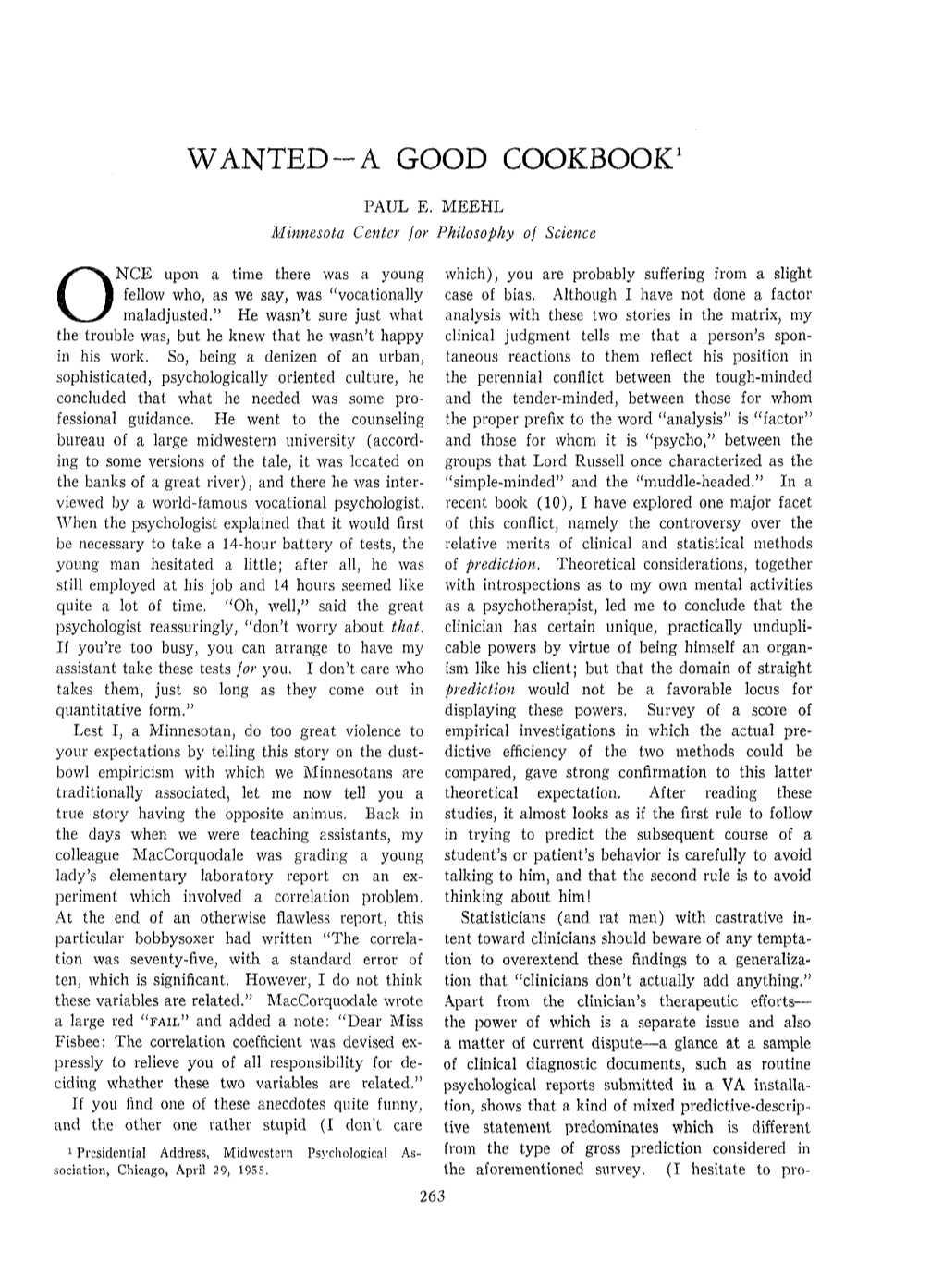
Wanted-A Good Cookbook1
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Someone's in the Kitchen Where's Dinah? Gendered Dimensions of the Professional Culinary World"
DePaul University Via Sapientiae College of Education Theses and Dissertations College of Education Spring 6-14-2013 SOMEONE’S IN THE KITCHEN, WHERE’S DINAH? GENDERED DIMENSIONS OF THE PROFESSIONAL CULINARY WORLD Stephanie Konkol DePaul University Follow this and additional works at: https://via.library.depaul.edu/soe_etd Part of the Education Commons Recommended Citation Konkol, Stephanie, "SOMEONE’S IN THE KITCHEN, WHERE’S DINAH? GENDERED DIMENSIONS OF THE PROFESSIONAL CULINARY WORLD" (2013). College of Education Theses and Dissertations. 68. https://via.library.depaul.edu/soe_etd/68 This Dissertation is brought to you for free and open access by the College of Education at Via Sapientiae. It has been accepted for inclusion in College of Education Theses and Dissertations by an authorized administrator of Via Sapientiae. For more information, please contact [email protected]. DePaul University College of Education SOMEONE’S IN THE KITCHEN, WHERE’S DINAH? GENDERED DIMENSIONS OF THE PROFESSIONAL CULINARY WORLD A Dissertation in Education With a Concentration in Curriculum Studies by Stephanie M. Konkol Copyright 2013 Stephanie M. Konkol Submitted in Partial Fulfillment Of the Requirements For the Degree of Doctor of Education June 14, 2013 iii ABSTRACT Traditionally cooking is considered to be women’s work, yet the vast majority of professional chefs, particularly in the upper echelons of restaurant work, are men. These curious gendered patterns stimulated interest in delving more deeply into the gendered nature of restaurant work. Existing research on this topic has concentrated on the front of the house (dining room) but has not addressed the gendered nature of the male-dominated back of the house (kitchen). -

Music 18145 Songs, 119.5 Days, 75.69 GB
Music 18145 songs, 119.5 days, 75.69 GB Name Time Album Artist Interlude 0:13 Second Semester (The Essentials Part ... A-Trak Back & Forth (Mr. Lee's Club Mix) 4:31 MTV Party To Go Vol. 6 Aaliyah It's Gonna Be Alright 5:34 Boomerang Aaron Hall Feat. Charlie Wilson Please Come Home For Christmas 2:52 Aaron Neville's Soulful Christmas Aaron Neville O Holy Night 4:44 Aaron Neville's Soulful Christmas Aaron Neville The Christmas Song 4:20 Aaron Neville's Soulful Christmas Aaron Neville Let It Snow! Let It Snow! Let It Snow! 2:22 Aaron Neville's Soulful Christmas Aaron Neville White Christmas 4:48 Aaron Neville's Soulful Christmas Aaron Neville Such A Night 3:24 Aaron Neville's Soulful Christmas Aaron Neville O Little Town Of Bethlehem 3:56 Aaron Neville's Soulful Christmas Aaron Neville Silent Night 4:06 Aaron Neville's Soulful Christmas Aaron Neville Louisiana Christmas Day 3:40 Aaron Neville's Soulful Christmas Aaron Neville The Star Carol 2:13 Aaron Neville's Soulful Christmas Aaron Neville The Bells Of St. Mary's 2:44 Aaron Neville's Soulful Christmas Aaron Neville Tell It Like It Is 2:42 Billboard Top R&B 1967 Aaron Neville Tell It Like It Is 2:41 Classic Soul Ballads: Lovin' You (Disc 2) Aaron Neville Don't Take Away My Heaven 4:38 The Grand Tour Aaron Neville I Owe You One 5:33 The Grand Tour Aaron Neville Don't Fall Apart On Me Tonight 4:24 The Grand Tour Aaron Neville My Brother, My Brother 4:59 The Grand Tour Aaron Neville Betcha By Golly, Wow 3:56 The Grand Tour Aaron Neville Song Of Bernadette 4:04 The Grand Tour Aaron Neville You Never Can Tell 2:54 The Grand Tour Aaron Neville The Bells 3:22 The Grand Tour Aaron Neville These Foolish Things 4:23 The Grand Tour Aaron Neville The Roadie Song 4:41 The Grand Tour Aaron Neville Ain't No Way 5:01 The Grand Tour Aaron Neville The Grand Tour 3:22 The Grand Tour Aaron Neville The Lord's Prayer 1:58 The Grand Tour Aaron Neville Tell It Like It Is 2:43 Smooth Grooves: The 60s, Volume 3 L.. -
A S I a K Y R
a s i a k y r e e MARCH 2020 ISSUE 3 Table Of Contents WORDS FROM THE EDITOR SONGS TO HEAR THE LEGENDARY MISSY ELLIOTT RETURNS SHE BEEN BUZZIN: JOCELYN A RIVERA CATCHING UP WITH BAD GUY AK- ASIA KYREE BUZZIN ON THE MIX PLAYLIST SHE BEEN BUZZIN: MARIE THEODORE MEET SINGER SONGWRITER JAWAN MEET SINGER JASMINE KIARA PROJECTS TO HEAR 2 WORDS FROM THE EDITOR Photo by Rodrigo L. Instagram: @peruvianrodrigo Rodrigo by L. Instagram: Photo Welcome to the third issue of She Buzzin Magazine. It's been one hell of a journey and I am so happy to finally deliver this issue to you all. As many of you know, March is Women's History month and has become She Buzzin's anniversary, since the release of the first issue in 2019. I appreciate all the love and support this platform has received thus far. I'd like to thank all the contributors who were involved in the production of this issue. Special shout out to Co-Editor Jasmine Rush and Creative Director Kashiem Brown, you all are nothing short of amazing. Since outside is cancelled for the time being and we're doing our best to practice social dis- tancing, I hope the songs and artists featured in this copy give you a reason to connect with those around you. In the age of instant releases, listeners don't have the luxury to sit and digest music like before. I challenge you to step out of the realm of mainstream plays and tap into the underground sector. -

Youth Workbook Sections 1-8 Sections
Youth Workbook Sections 1-8 Youth Workbook Sections 1-8 Helthy Trnsitions FOUNDATION for CALIFORNIA COMMUNITY COLLEGES Youth and Adult Serices Helthy Trnsitions 2 Health & Wellness Workbook Dustianne North, M.S.W., Ph.D. Jerry Sherk, M.A. Sarah E. Kremer, MA, ATR-BC Andrea Barrera Siobhan Stofka The California Mental Health Services Authority (CalMHSA) is an organization of county governments working to improve mental health outcomes for individuals, families and communities. Prevention and Early Intervention programs implemented by CalMHSA are funded through the voter-approved Mental Health Services Act (Prop 63). Prop. 63 provides the funding and framework needed to expand mental health services to previously underserved populations and all of California’s diverse communities. CALIFORNIA COMMUNITY COLLEGES CHANCELLOR’S OFFICE FOUNDATION for CALIFORNIA COMMUNITY COLLEGES Youth and Adult Serices 3 Table of Contents Session 1: Daily Wellness ................................................................................................................... 6 Why Should I Learn about Wellness and Self-Care? ..................................................................................................7 - 8 The Tree That is Me ..................................................................................................................................................................9 - 10 Wellspring Wellness ..................................................................................................................................................................11 -

Anarchists Cookbook V2000
ANARCHY COOKBOOK VERSION 2000 Table of Contents 1.Counterfeiting Money 58.Generic Bomb 2.Credit Card Fraud 59.Green Box Plans 3.Making Plastic Explosives 60.Portable Grenade Launcher 4.Picking Master Locks 61.Basic Hacking Tutorial I 5.The Arts of Lockpicking I 62.Basic Hacking Tutorial II 6.The Arts of Lockpicking II 63.Hacking DEC's 7.Solidox Bombs 64.Harmless Bombs 8.High Tech Revenge: The Beigebox 65.Breaking into Houses 9.COý Bombs 66.Hypnotism 10.Thermite II Bombs 67.Remote Informer Issue #1 11.Touch Explosives 68.Jackpotting ATM Machines 12.Letter Bombs 69.Jug Bomb 13.Paint Bombs 70.Fun at K-Mart 14.Ways to send a car to HELL 71.Mace Substitute 15.Do you hate school? 72.How to Grow Marijuana 16.Phone related vandalism 73.Match Head Bomb 17.Highway police radar jamming 74.Terrorizing McDonalds 18.Smoke Bombs 75."Mentor's" Last Words 19.Mail Box Bombs 76.The Myth of the 2600hz Detector 20.Hot-wiring cars 77.Blue Box Plans 21.Napalm 78.Napalm II 22.Fertilizer Bomb 79.Nitroglycerin Recipe 23.Tennis Ball Bomb 80.Operation: Fuckup 24.Diskette Bombs 81.Stealing Calls from Payphones 25.Unlisted Phone Numbers 82.Pool Fun 26.Fuses 83.Free Postage 27.How to make Potassium Nitrate 84.Unstable Explosives 28.Exploding Light bulbs 85.Weird Drugs 29.Under water igniters 86.The Art of Carding 30.Home-brew blast cannon 87.Recognizing Credit Cards 31.Chemical Equivalency List 88.How to Get a New Identity 32.Phone Taps 89.Remote Informer Issue #2 33.Landmines 90.Remote Informer Issue #3 34.A different Molitov Cocktail 91.Remote Informer Issue #4 35.Phone -

The Imaginative Nature National Council of Teachers of En
DOCUMENT RESUME ED 404 675 CS 215 781 AUTHOR Pugh, Sharon L.; And Others TITLE Metaphorical Ways of Knowing: The Imaginative Nature of Thought and Expression. INSTITUTION National Council of Teachers of English, Urbana, Ill. REPORT NO ISBN-0-8141-3151-4 PUB DATE 97 NOTE 225p. AVAILABLE FROMNational Council of Teachers of English, 1111 W. Kenyon Road, Urbana, IL 61801-1096 (NCTE Stock No. 31514-3050: $12.95 members, $16.95 nonmembers). PUB TYPE Viewpoints (Opinion/Position Papers, Essays, etc.) (120) Books (010) EDRS PRICE MF01/PC09 Plus Postage. DESCRIPTORS Class Activities; *English; *Imagination; Interdisciplinary Approach; Intermediate Grades; Language Arts; *Language Role; *Metaphors; *Multicultural Education; Rhetoric; Secondary Education IDENTIFIERS *Metaphorical Thought ABSTRACT This book explores the subject of metaphor, using the imagery of cartography to set a course. It explores the creative aspects of thinking and learning through literature, writing, and word play, drawing connections between English and other content areas. Theory and practical applications meet in the book, linking activities and resources to current classroom concerns--to multiculturalism, imagination in reading and writing, critical thinking, and expanding language experiences. The first part of the book examines the uses of metaphor in constructing meaning. The second part takes up issues related to multiple perspectives--using metaphors to experience other lives, and exploring cultures through traditions. The third part of the book is devoted to a consideration of the history and current status of the English language and focuses on using cross-cultural stories in the English classroom, offering a number of resources for teaching multicultural literature in English. The fourth part examines the sensory Ixperience of metaphors by seeing, hearing, tasting, smelling, and touching with the imagination. -

Peach State Caravanner Volume 52 / Issue 6 / November 2013
Peach State Caravanner Volume 52 / Issue 6 / November 2013 visit, please come to the Top and get involved. You'll be glad you did! To all our volunteers, thank you for your participation and help that is so vital for our success. Vonceil and Howard NeSmith did a great service leading the Airstream Tips session on Saturday. There was good information shared to keep our members aware of procedures to maintain their Airstreams. We always learn something helpful in these sessions! There were more than 30 members attending. I'm already getting excited about next season and our April work days on April 14-15! This is a neat time when our members come and Hello Airstream friends! work together to ready our park for our first rally of the season, the spring rally! Thanks to ow, Airstreamers, did we have a great all the Volunteers who help to get the Top in W Fall Rally or what! The weather was shape. just what the doctor ordered, cool nights and mostly very nice days. Everyone had an Our 2014 season will bring some new ideas to attitude of "Live, laugh and love," and believe us such as theme names for Rallys, and your me, your Board worked "better together" and First Lady Sharon will share a new craft each got a lot of things accomplished. Of course, rally with the ladies. One additional Buddy the major project is the replacement of the Rally is set to introduce more of our buddies entrance retainer wall to the park. The to the Airstream lifestyle. -

JIMMY DOUGLASS – Producer/Mixer/Engineer
JIMMY DOUGLASS – Producer/Mixer/Engineer Jimmy Douglass is the most rare of creative people. With unmatched experience across the genres, Jimmy has been making records sound exciting for years. There aren’t many that can boast the diversity of Jimmy’s discography and he feels equally at home with organic musician driven music as he does in the world of hip-hop that he now dominates. As long time engineer and mixer for Timbaland, Jimmy has been instrumental in pushing forward hip-hop music and he continues breaking boundaries. Form is temporary, class is permanent. Discography Mixed Justin Timberlake “The 20/20 Experience” Album RCA The Cataracs “Mouthful” EP Track Universal Republic Aaliyah “Aaliyah” Album Virgin “I Care 4 You” Album Virgin “Try Again” Single Virgin “Are U That Somebody” Single “One in A Million” Single John Legend & The Roots “Wake-Up” Album Columbia Justin Timberlake “Future Sex Love Songs” Singles & Album Jive “Sexy Back” “What Goes Around Comes Around” “My Love” “Justified” Album Jive “Cry Me A River” Single Al Green “Lay It Down” Album Blue Note Ginuwine “The Bachelor” Album Epic “So Anxious Album” Album Epic “Life” Album Epic Jay-Z “Dirt Off Your Shoulder” Single Roc-A-Fella “The Black Album” Album Tracks “Vol 2: Hard Knock Life” Album Roc-A-Fella “Vol 3: Life & Times…” Album Roc-A-Fella “Big Pimpin” Single Roc-A-Fella “In My Lifetime Vol. 3” Album Missy Elliott “Da Real World” Album Elektra “Miss E… So Addictive” Album Elektra “Under Construction” Album Elektra “The Cookbook” Album Atlantic “Work It”/Get ur Freak -
The Fourth of March Brian Doyle
number forty-eight HARVARD REVIEW published by HOUGHTON LIBRARY harvard university HARVARD REVIEW publisher: Tom Hyry, Florence Fearrington Librarian of Houghton Library publisher emeritus: Michael Shinagel founding editor: Stratis Haviaras editor: Christina Thompson poetry editor: Major Jackson fiction editor: Suzanne Berne visual arts editor: Judith Larsen digital editor: Laura Healy managing editor: Chloe Garcia Roberts design: Alex Camlin contributing editors: André Aciman • John Ashbery • Robert Atwan • Mary Jo Bang • Karen Bender • Michael Collier • Robert Coover • Lydia Davis • Denise Duhamel • David Ferry • Stephen Greenblatt • Alice Hoffman • Miranda July • Ilya Kaminsky • Yusef Komunyakaa • Campbell McGrath • Heather McHugh • Rose Moss • Geoffrey Movius • Paul Muldoon • Les Murray • Dennis O’Driscoll • Peter Orner • Carl Phillips • Stanley Plumly • Theresa Rebeck • Donald Revell • Peter Sacks • Robert Antony Siegel • Robert Scanlan • Charles Simic • Cole Swensen • Chase Twichell • Dubravka Ugresic • Katherine Vaz • Kevin Young senior readers: M. R. Branwen, Deborah Pursch interns: Christopher Alessandrini • Silvia Golumbeanu • Virginia Marshall • Victoria Zhuang readers: Nathan Bernhard • Laila Carter • Ophelia John • Tess Cushing • Allie Freiwald • Annie Harvieux • Joan Li • Joanna Liu • Jennifer Nickerson • Kelsey O’Connor • Rachel Poser • Rachel Silverstein • Sebastian Sarti • Annie Wei • Natalia Wojcik harvard review (issn 1077-2901) is published twice a year by Houghton Library domestic subscriptions: individuals: $20 (one year); $50 (three years), $80 (five years) institutions: $30 (one year) overseas subscriptions: individuals: $32 (one year) institutions: $40 (one year) enquiries to: Harvard Review, Lamont Library, Harvard University, Cambridge, MA 02138 phone: (617) 495-9775 fax: (617) 496-3692 email: [email protected] online at harvardreview.org paper submissions should be accompanied by sase. online submissions should be submitted at harvardreview.submittable.com. -
The Kazaa Ruling Oz Court Forces Music Biz Into Action >P.12 the Music Upfront Labels Tighten Links with Consumer Brands >P.32
KANYE'S BUSH BASHING IGNITES HIP -HOP PASSIONS >os #BXNCTCC SCH 3-DIGIT 90', IIIIIIII111I11I1II1III111I11III1I11III I II111II #BL2408043# FPRO6 A04 B009: MONTY GR.ETIL1 3740 ELM A\.E # A TONG BEACH CA 90807 -340 SEPT FOR MORE THAN 110 YEARS 17 2005 DOUBLE WHAMMY OIL PRICES, KATRINA ADD TO INDUSTRY WOES >P.5 THE KAZAA RULING OZ COURT FORCES MUSIC BIZ INTO ACTION >P.12 THE MUSIC UPFRONT LABELS TIGHTEN LINKS WITH CONSUMER BRANDS >P.32 U NT'S 55.99US E8.99CAP 74470 6.99, CAN $8.39, UK 8.95, JAPAN Y2,500 www.billboard.com www.billboard.biz www.americanradiohistory.com music.yahoo.com LET EHERE BE INO , 1 !r -on 11 r Over a million songs. 5 bucks a month. THIS IS HUGE. M MUSICrMUNLIMITED O N YIAHOO ! www.americanradiohistory.com SAVE THE BATE: ems Billb.aral SEPTEMBER 17, 2005 DAncE music summIT VOLUME 117, NO. 38 Union Sq.Jare Ballroom, NYC bil boardeverts.com ON THE CHARTS KOMI ALBUMS PAGE ARTIST / TITLE UPFRONT KANYE WEST / 5 News THE BILLBOARD 200 46 LATE REGISTRATION NICKEL CREEK / 15 Legal Matters TOP BLUEGRASS 56 WHV SHOULD THE HRE DIE? 16 Global YO -YO MA/THE SILK ROAD ENSEMBLE / 70P CLASSICAL '= 61 `r '" SILK ROAD JOURNEYS.: BEYOND THE HORIZON 18 The Indies TOP CLASSICAL CROSSOVER r 61 0 / 19 Retail Track BROOKS & DUNN / 20 Making The Brand TOP COUNTRY 56 HILLBILLY DELUXE GORILIAZ / 22 On The Road, Boxscore TOP ELECTRONIC F 59 DAYS DEMON 24 Touring KANYE WEST / TOP INTERNET 62 LATE REGISTRATION 25 Digital Entertainment TOP MICHAEL NUBLE / JAZZ 61 IT'S TIME 26 Q&A: Joe DiMuro HERBIE K / TOP CONTEMPORARY JAZZ 61 POSS IOILITIES COVER STORY SHAKIRA / TOP LATIN 58 FUACION ORAL VOL. -

Missy Elliot Get Your Freak on Clean Mp3 Download
Missy elliot get your freak on clean mp3 download Buy Get Ur Freak On [Clean]: Read 2 Digital Music Reviews - Buy Get Ur Freak On [Explicit]: Read 21 Digital Music Reviews - "Get Ur Freak On" is a hip hop song written by American rapper/singer Missy Elliott and her producer Tim "Timbaland" Mosley for Elliott's third studio album Miss. Get Ur Freak On. Missy Elliott - Miss Addictive • MB • K plays. Get Ur Freak On (stanislav Shik & Denis Rook Remix). Missy Elliott • MB • K. I DO NOT own this song. All credit goes to Missy Elliot and WMG. Please Subscribe to my channel and. Similar to the MTV and Vevo versions. I created this by combining the acapella with the instrumental. If you. "Get Ur Freak On [Clean]" by Missy Elliott Listen ad-free with YouTube Red; Download Free missy elliott get ur freak on mp3 music download, easily listen and. Lose Control (Clean Extended Break) - Missy Elliott by Dj Promote, released 30 Missy Elliot Get Ur Freak On ACDC Remix (Plus mp3 download link) Missy. "Get Ur Freak On" is a song by American recording artist Missy "Misdemeanor" Elliott. In , Scottish acoustic rocker KT Tunstall released her version of "Get Ur Freak On" performed for BBC Radio Live Lounge on certain versions of the. Get Ur Freak On Lyrics: Kore kara minna de mechakucha odotte / Sawago Missy Elliott Missy be puttin' it down, I'm the hottest 'round We got the radio shook like we got a gun Eight years after it hit the top ten of Billboard's Hot , “Get Ur Freak On” still sounds like an audaciously leftfield stroke of genius, a song. -
The-Cookbook-V-1.4.Pdf Efficiency Is Everything 2
1 The Efficiency Is Everything Cookbook Recipes that have you eating for $24 a week. Eight recipes that take two active minutes and make enough food for a week. Food that is so phenomenal that anyone will believe you are a professional. Michael Kirk https://efficiencyiseverything.com/The-Cookbook-v-1.4.pdf Efficiency Is Everything 2 Preface These recipes are not authentic to a country, a culture, or cuisine; they are time effective, affordable, often healthy, and tasty. I am not a chef, but I spent hours reading cooking message boards daily, reading Good Housekeeping at the gym, and excessive time cooking/trying/studying food, including our own Efficiency Is Everything Calorie and Protein Per Dollar List. These are the meals we eat daily, the groceries we buy every week, and serve our friends. I give detailed work instructions style directions, but most corners can be cut. I suggest reading through the entire recipe you plan to make, before starting. I wrote this recipe book like I am talking to someone who has experience with ramen while trying to shove as many of the cooking tips I’ve learned - all combined with the Factory Efficiency. Efficiency Is Everything - In Life is concise, each recipe has very fine details, using Work Instructions. The goal being, that everyone regardless of skill, can pick up the recipe and complete it without questions and without difficulty. This was written like a book, where the first chapters give the finer details on characters – in this case the first recipes give the specifics on the cooking processes.