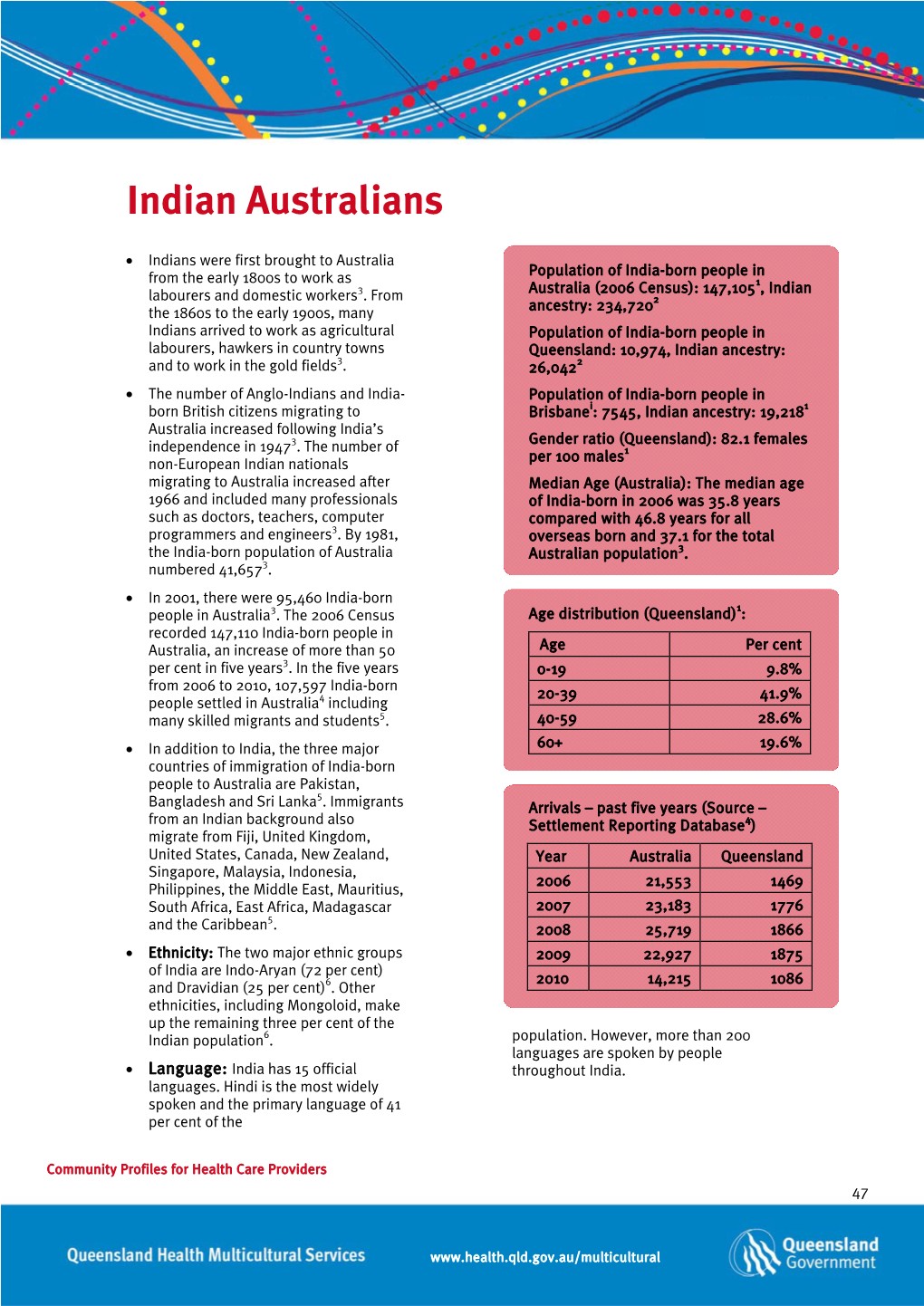
Community Profiles for Health Care Providers 47
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Disporia of Borders: Hindu-Sikh Transnationals in the Diaspora Purushottama Bilimoria1,2
Bilimoria International Journal of Dharma Studies (2017) 5:17 International Journal of DOI 10.1186/s40613-017-0048-x Dharma Studies RESEARCH Open Access The disporia of borders: Hindu-Sikh transnationals in the diaspora Purushottama Bilimoria1,2 Correspondence: Abstract [email protected] 1Center for Dharma Studies, Graduate Theological Union, This paper offers a set of nuanced narratives and a theoretically-informed report on Berkeley, CA, USA what is the driving force and motivation behind the movement of Hindus and Sikhs 2School of Historical and from one continent to another (apart from their earlier movement out of the Philosophical Studies, The University of Melbourne, Melbourne, Australia subcontinent to distant shores). What leads them to leave one diasporic location for another location? In this sense they are also ‘twice-migrants’. Here I investigate the extent and nature of the transnational movement of diasporic Hindus and Sikhs crossing borders into the U.S. and Australia – the new dharmic sites – and how they have tackled the question of the transmission of their respective dharmas within their own communities, particularly to the younger generation. Two case studies will be presented: one from Hindus and Sikhs in Australia; the other from California (temples and gurdwaras in Silicon Valley and Bay Area). Keywords: Indian diaspora, Hindus, Sikhs, Australia, India, Transnationalism, Diaspoetics, Adaptation, Globalization, Hybridity, Deterritorialization, Appadurai, Bhabha, Mishra Part I In keeping with the theme of Experimental Dharmas this article maps the contours of dharma as it crosses borders and distant seas: what happens to dharma and the dharmic experience in the new 'experiments of life' a migrant community might choose to or be forced to undertake? One wishes to ask and develop a hermeneutic for how the dharma traditions are reconfigured, hybridized and developed to cope and deal with the changed context, circumstances and ambience. -

Vietnamese Identities in Modern Australia
A Quintessential Collision: critical dimensions of the Vietnamese presence in the Australia empire project Andrew Jakubowicz University of Technology Sydney Cultures in Collision Colloqium Transforming Cultures UTS May 9 2003 Abstract The Vietnamese arrival and integration into Australia represents a quintessential case of cultures in collision. In 1975 there was effectively no Vietnamese presence. Over the next twenty five years the community grew to over two hundred thousand members. Before 1975 Vietnam and Australia barely knew each other – except through the prism of the American War. By 2001 Generation 2 were a significant part of Australian political, economic and cultural life. The Vietnamese were used as the trigger for the end of the bi-partisanship on multiculturalism at the end of the 1970s, were implicated in the rising paranoia about unsafe cities in the 1980s, and centrally embroiled in the emergence of a politics of race in the 1990s. They also reflect two trajectories of integration – the anomie associated with marginalization, and the trans-national engagement associated with globalizing elites. This paper explores processes of cultural collision and reconstitution through an examination of three dimensions of the Vietnamese in Australia - the criminal world of the heroin trade; the rise and fall of Phuong Ngo; and the celebration of Generation 2. Note: this is a draft for discussion. Full references in final paper Introduction In July 2002 three young men of Vietnamese background died in an attack by a group of five young men of similar background outside a Melbourne nightclub. The tragedy was fully reported in The Age newspaper, which also was careful to refrain from using ethnic descriptors in presenting the facts of the case. -

Vietnamese Family Reunion in Australia 1983 – 2007 Bianca Lowe
Vietnamese Family Reunion in Australia 1983 – 2007 Bianca Lowe Submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy March 2016 Graduate School of Historical and Philosophical Studies The University of Melbourne ABSTRACT This thesis explores the reunification of Vietnamese families in Australia through the family reunion program from 1983 to 2007. Focusing upon these key years in the program, and building upon substantial existing research into the settlement of Vietnamese refugees in Australia, this dissertation adds to the knowledge of Vietnamese-Australian migration by focusing on the hitherto neglected story of family reunion. It offers an account of the process and circumstances by which Vietnamese families attempted to reunite and establish new lives in Australia, following the Vietnam War. Drawing upon analysis of political debate and interviews with Vietnamese families, this thesis provides an overview of years that challenged traditional narratives of national identity and of the composition and character of the ‘family of the nation’. During this period, the Australian Government facilitated the entry of large numbers of Asian migrants, which represented a fundamental shift in the composition of the national community. Analysis of political commentary on Vietnamese family reunion reveals tensions between the desire to retain traditional conceptions of Australian national identity and the drive to present Australia as an adaptable and modern country. The early chapters of this thesis examine political debate in the Australian Parliament about the family reunion program. They note differing emphases across the Hawke-Keating Labor Government (1983-1996) and Howard Liberal-National Coalition Government (1996-2007), but also similarities that underline the growing adherence to economic rationalism and the effect this had on the broad design of the program. -

``Citizenship from Below'' Among ``Non-White'' Minorities in Australia
“Citizenship from below” among “non-white” minorities in Australia: Intergroup relations in a northern suburb of Adelaide Ritsuko Kurita To cite this version: Ritsuko Kurita. “Citizenship from below” among “non-white” minorities in Australia: Intergroup relations in a northern suburb of Adelaide. Anthropological Notebooks , Slovenian Anthropological Society, 2020. halshs-03115973 HAL Id: halshs-03115973 https://halshs.archives-ouvertes.fr/halshs-03115973 Submitted on 20 Jan 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. ‘Citizenship from Below’ Among ‘Non-White’ Minorities in Australia: Intergroup Relations in a Northern Suburb of Adelaide Ritsuko Kurita Associate professor, Faculty of Foreign Languages, Department of English, Kanagawa University [email protected] Abstract The recent scholarship on citizenship has highlighted the significance of horizontal citizenship, which states how an individual’s eligibility for membership is determined by a social system formed by equal peers and the development of a community who share a citizen’s sense of belonging. However, researchers have paid scant attention to the sense of citizenship evinced by marginalised ethnic minorities. The present investigation examines citizenship in Australia by exploring intergroup relations. It attempts to determine the feeling of belonging that connects the Indigenous people of Australia to other ‘non-white’ groups considered ’un-Australian’ by the mainstream society. -

Out of Africa: Sudanese Refugees and the Construction of Difference in Political and Lay Talk
Out of Africa: Sudanese refugees and the construction of difference in political and lay talk Scott Hanson-Easey School of Psychology Faculty of Health Sciences The University of Adelaide Submitted in fulfilment of the requirements for the degree of Doctor of Philosophy December 2011 Abstract ................................................................................................................................... iii Declaration ............................................................................................................................ vii Publications .......................................................................................................................... viii Acknowledgments ................................................................................................................. ix Exegesis .................................................................................................................................... 1 The structure of this thesis .................................................................................................... 5 Aims of this thesis .................................................................................................................. 6 Chapter 1: Previous discursive research on refugees and asylum seekers .......... 9 Australia‟s humanitarian refugee history ............................................................................. 9 Discursive research on refugees and asylum seekers in Australia, the United Kingdom and Spain. ............................................................................................................ -

A Peaceful Mind: Vietnamese-Australians with Liver Cancer
A peaceful mind: Vietnamese-Australians with liver cancer Interview report Max Hopwood & Carla Treloar Centre for Social Research in Health The University of New South Wales December 2013 1 Summary: Participants indicated little desire for detailed information about liver cancer. Family doctors and liver specialists were the primary sources of information about liver cancer. The internet was another source of liver cancer-related information. DVDs, print resources and Australian/Vietnamese media were not considered to be good sources of liver cancer-related information. Participants relied upon interpreters for understanding the information and advice given by doctors and specialists. Culture and family had a large influence over dietary decisions. Unemployment and under-employment as a result of illness created financial stress for participants. Participants borrowed money from friends and family when necessary. Coping with liver cancer was facilitated by a focus on keeping a peaceful mind. Strategies to consider: On the basis of interview findings derived from this small sample of Vietnamese- Australian liver cancer patients, the following strategies might be considered: Liaising with Vietnamese community medical practitioners to discuss ways of supporting family doctors and liver specialists to ensure patients receive adequate levels of information about living with liver cancer and treatment options. A review of Vietnamese language websites for people with liver cancer, and a compilation of URL addresses of the best site(s) for dissemination via Vietnamese media, community family doctors and liver cancer specialists. A review of interpretation services for Vietnamese people with an aim to publish an online directory and printed directory in the Vietnamese media. -

Continuing Relationship Between Kinan Area in Japan and Northern Australia
The Otemon Journal of Australian Studies, vol. 35, pp. 147−155, 2009 147 Migration and Beyond: Continuing relationship between Kinan area in Japan and northern Australia Yuriko Yamanouchi School of Global Studies, Tama University Abstract In most of the migration studies, the focus is on migrants and their descendants. When temporary migrants return to their original country, the effect of their migration to connect their original and receiving countries has not been approached academically. In this research note, I would like to examine the various relationships and ties developed after migration was consid- ered ‘finished’. From the 1870s to 1960s, Japanese migratory workers worked in northern Aus- tralia, namely Thursday Island and Broome, in industries such as pearl shelling. With the out- break of World War II, most of them were interned and eventually deported. However, the ties and relationships they developed through migration have continued and led to another ties and relationships in various ways. By looking at this, I suggest rethinking the framework of ‘migra- tion’ itself. 1. Introduction In most of the migration studies, the focus is on the migrants and their descendants. In cases of temporary migrants such as return migrants, temporary labour migrants and sojourners, the phe- nomenon of migration is often considered to ‘finish’ when the migrants return to their countries of origin on permanent basis, although there has been the research on the ex-migrants after they return to their countries of origin focusing on the issues such as their re-integration into their original so- ciety, usage of remittances, and memory and nostalgia (e.g. -

Cultural Profiles for Health Care Providers
Queensland Health CCoommmmuunniittyy PPrrooffiilleess for Health Care Providers Acknowledgments Community Profiles for Health Care Providers was produced for Queensland Health by Dr Samantha Abbato in 2011. Queensland Health would like to thank the following people who provided valuable feedback during development of the cultural profiles: x Dr Taher Forotan x Pastor John Ngatai x Dr Hay Thing x Ianeta Tuia x Vasanthy Sivanathan x Paul Khieu x Fazil Rostam x Lingling Holloway x Magdalena Kuyang x Somphan Vang x Abel SIbonyio x Phuong Nguyen x Azeb Mussie x Lemalu Felise x Nao Hirano x Faimalotoa John Pale x Surendra Prasad x Vaáaoao Alofipo x Mary Wellington x Charito Hassell x Rosina Randall © State of Queensland (Queensland Health) 2011. This document is licensed under a Creative Commons Attribution Non-Commercial 2.5 Australia licence. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/2.5/au. You are free to copy, communicate and adapt the work for non-commercial purposes, as long as you attribute Queensland Health. For permissions beyond the scope of this licence contact: Intellectual Property Officer Queensland Health GPO Box 48 Brisbane Queensland 4001 email [email protected] phone 07 3234 1479 Suggested citation: Abbato, S. Community Profiles for Health Care Providers. Division of the Chief Health Officer, Queensland Health. Brisbane 2011. i www.health.qld.gov.au/multicultural Table of contents Acknowledgments............................................................................................................ -

Table of Contents Vidya Ramachandran
Table of Contents Privileged Hybrids: Examining ‘our own’ in the Indian-Australian diaspora ................ 2 Introduction .................................................................................................................... 2 Data collection and methodology ..................................................................................... 3 The Indian diaspora in Australia: navigating ‘Indianness’ and ‘Australianness’ ........... 4 Towards ‘Indianness’: the gradual dissolution of regional/linguistic identity ................. 7 ‘Hinduness’ and ‘Indianness’ .......................................................................................... 8 A model minority ............................................................................................................ 9 Unpacking caste: privilege and denial ........................................................................... 10 Conclusion ..................................................................................................................... 13 Vidya Ramachandran 1 Privileged Hybrids: Examining ‘our own’ in the Indian-Australian diaspora Introduction In April, the ‘Indian Wedding Race’ hit television screens across Australia (Cousins 2015). The first segment in a three-part series on multicultural Australia distributed by the SBS, the documentary follows two young Indian-Australians in their quest to get married before the age of thirty. Twenty-nine year-old Dalvinder Gill-Minhas was born and raised in Melbourne. Dalvinder’s family members are -

Japanese Lifestyle Migrants in Southeast Queensland
Japanese lifestyle migrants in Southeast Queensland: Narratives of long-term residency, mobility and personal communities Jared Denman BA Honours (Japanese); BEd A thesis submitted for the degree of Doctor of Philosophy at The University of Queensland in 2014 School of Languages and Comparative Cultural Studies Abstract Contemporary Japanese migration and overseas residency are being increasingly understood through the lens of lifestyle migration, whereby those who leave Japan prioritise lifestyle factors ahead of other considerations. Studies of Australia’s Japanese communities in particular have tended to focus on such migrants and advance this concept. This study employs biographical- narrative and case study elements to further the study of Japanese lifestyle migration to Australia in two ways. One is by examining cases from a cohort in Southeast Queensland that has yet to be a focus of investigation: those who arrived during the late 1980s and early 1990s, before the transformations of post-bubble Japan. The other is by supplementing existing understandings of Japanese phenomena with an emerging conceptualisation of lifestyle migration in Western Europe. This alternative framework observes that narratives of lifestyle migrants are shaped by themes of escape and pursuit and rhetoric of personal transformation, while also proposing that the act of migration is not a final outcome but is embedded within an ongoing lifestyle trajectory. By analysing participants’ narratives and examining their reasons for migration, their mobility histories and self-defined personal communities, this thesis argues that existing characterisations of the particular cohort and of Japanese lifestyle migrants in general are too narrow. Decisions are not straightforward individual matters framed by escape and pursuit, but can be directed by more complicated individual and household trajectories influenced by a variety of mobility experiences that are not simply geographical. -

Improving Outcomes with South Sudanese Australians a Co-Design Project to Build on Community Strengths and Initiate New Solutions
Improving Outcomes with South Sudanese Australians A co-design project to build on community strengths and initiate new solutions September 2018 Acknowledgement of traditional land owners As guests, vistors, migrants and refugees we acknowledge the traditional owners of the land. We offer our deepest respect to the ancestors and elders of these traditional lands, and through them to all Aboriginal and Torres Straight Island peoples past and present. Written by Farida Machar, Co-designer Acknowledgement of the South Sudanese Australian Community It was a great privilege for us to work with and hear the stories of all participants within the South Above: Young women who participated in co-design consultations Sudanese Australian Community. This work would not have been possible without their generosity in sharing experiences, insight and wisdom. The pathways presented on the following pages reflect what was heard from and created by members of the South Sudanese Communities of Western Metropolitan Melbourne. We pay our respects to South Sudanese Australian Community leaders and elders of the past present and future and are committed to collaboratively working toward a better future for all. Improving Outcomes with the South Sudanese Community 2 Community Co-designers The work presented here was conducted in cohealth is a not-for-profit community health collaboration with a Community Co-design organisation that provides vital local health and team: support services including medical, dental, allied Ariik Arok, Anyuop Dau, Farida Machar, Flora Chol, health, mental health, aged care and counselling, John Jok, Sebit Gurech and Ez Eldin Deng. and many specialist health services across Melbourne’s CBD, northern and western suburbs. -

Engagement with Asia: Time to Be Smarter
Securing Australia's Future By Simon Torok and Paul Holper, 208pp, CSIRO Publishing, 2017 2 Engagement with Asia: time to be smarter You can’t do Asia with a Western head, Western thinking. Australian businesses miss opportunities because of a mindset that ‘Aussies know best’. Aussies need to change the way they think about their business. Chinese executive, quoted in SAF11 Australia’s Diaspora Advantage Golden thread Australia must celebrate its relationships in the Asia-Pacific region. We need to engage better and cement Australia’s prominent place in the region. Finding these new opportunities must embrace the invaluable resources of Asian and Pacific communities by improving Australia’s language ability, increasing cultural awareness, building on current export strengths and extending networks and linkages. Key findings This objective distils the interdisciplinary research and evidence from the 11 reports published as part of ACOLA’s Securing Australia’s Future project. To meet this objective, the following six key findings for improving Australia’s smart engagement with Asia and the Pacific need to be addressed: 1. Incentives are required to improve Australia’s linguistic and intercultural competence at school, university, and in the workplace. 2. We need to increase Australia’s ‘soft power’ through cultural diplomacy that updates perceptions of Australia in the Asia-Pacific region, and brings into the 21st century the way Australians see our place in the world. 23 © Australian Council of Learned Academies Secretariat Ltd 2017 www.publish.csiro.au Securing Australia's Future By Simon Torok and Paul Holper, 208pp, CSIRO Publishing, 2017 24 Securing Australia’s Future 3.