Assessing the Effectiveness of Two Intervention Methods for Stony Coral
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Coral Bleaching Early Warning Network Current Conditions Report #20090910
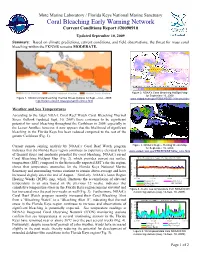
Mote Marine Laboratory / Florida Keys National Marine Sanctuary Coral Bleaching Early Warning Network Current Conditions Report #20090910 Updated September 10, 2009 Summary: Based on climate predictions, current conditions, and field observations, the threat for mass coral bleaching within the FKNMS remains MODERATE. Figure 2. NOAA’s Coral Bleaching HotSpot Map for September 10, 2009. Figure 1. NOAA’s Coral Bleaching Thermal Stress Outlook for Sept. – Dec., 2009. www.osdpd.noaa.gov/PSB/EPS/SST/climohot.html http://coralreefwatch.noaa.gov/satellite/index.html Weather and Sea Temperatures According to the latest NOAA Coral Reef Watch Coral Bleaching Thermal Stress Outlook (updated Sept. 10, 2009) there continues to be significant potential for coral bleaching throughout the Caribbean in 2009, especially in the Lesser Antilles; however, it now appears that the likelihood of significant bleaching in the Florida Keys has been reduced compared to the rest of the greater Caribbean (Fig. 1). Current remote sensing analysis by NOAA’s Coral Reef Watch program Figure 3. NOAA’s Degree Heating Weeks Map for September 10, 2009. indicates that the Florida Keys region continues to experience elevated levels www.osdpd.noaa.gov/PSB/EPS/SST/dhw_retro.html of thermal stress and moderate potential for coral bleaching. NOAA’s recent Water Temperatures (August 27 - September 10, 2009) Coral Bleaching HotSpot Map (Fig. 2), which provides current sea surface 35 temperature (SST) compared to the historically expected SST’s for the region, shows that temperature anomalies for the Florida Keys National Marine 30 Sanctuary and surrounding waters continue to remain above-average and have increased slightly since the end of August. -

A Research Review of Interventions to Increase the Persistence and Resilience of Coral Reefs (2019)
THE NATIONAL ACADEMIES PRESS This PDF is available at http://nap.edu/25279 SHARE A Research Review of Interventions to Increase the Persistence and Resilience of Coral Reefs (2019) DETAILS 258 pages | 6 x 9 | PAPERBACK ISBN 978-0-309-48535-7 | DOI 10.17226/25279 CONTRIBUTORS GET THIS BOOK Committee on Interventions to Increase the Resilience of Coral Reefs; Ocean Studies Board; Board on Life Sciences; Division on Earth and Life Studies; National Academies of Sciences, Engineering, and Medicine FIND RELATED TITLES SUGGESTED CITATION National Academies of Sciences, Engineering, and Medicine 2019. A Research Review of Interventions to Increase the Persistence and Resilience of Coral Reefs. Washington, DC: The National Academies Press. https://doi.org/10.17226/25279. Visit the National Academies Press at NAP.edu and login or register to get: – Access to free PDF downloads of thousands of scientific reports – 10% off the price of print titles – Email or social media notifications of new titles related to your interests – Special offers and discounts Distribution, posting, or copying of this PDF is strictly prohibited without written permission of the National Academies Press. (Request Permission) Unless otherwise indicated, all materials in this PDF are copyrighted by the National Academy of Sciences. Copyright © National Academy of Sciences. All rights reserved. A Research Review of Interventions to Increase the Persistence and Resilience of Coral Reefs A RESEARCH REVIEW OF INTERVENTIONS TO INCREASE THE PERSISTENCE AND RESILIENCE OF CORAL REEFS Committee on Interventions to Increase the Resilience of Coral Reefs Ocean Studies Board Board on Life Sciences Division on Earth and Life Studies A Consensus Study Report of Copyright National Academy of Sciences. -

Turbidity Criterion for the Protection of Coral Reef and Hardbottom Communities
DRAFT Implementation of the Turbidity Criterion for the Protection of Coral Reef and Hardbottom Communities Division of Environmental Assessment and Restoration Florida Department of Environmental Protection October 2020 Contents Section 1. Introduction ................................................................................................................................. 1 1.1 Purpose of Document .......................................................................................................................... 1 1.2 Background Information ..................................................................................................................... 1 1.3 Proposed Criterion and Rule Language .............................................................................................. 2 1.4 Threatened and Endangered Species Considerations .......................................................................... 5 1.5 Outstanding Florida Waters (OFW) Considerations ........................................................................... 5 1.6 Natural Factors Influencing Background Turbidity Levels ................................................................ 7 Section 2. Implementation in Permitting ..................................................................................................... 8 2.1 Permitting Information ........................................................................................................................ 8 2.2 Establishing Baseline (Pre-project) Levels ........................................................................................ -

Regional Studies in Marine Science Reef Condition and Protection Of
Regional Studies in Marine Science 32 (2019) 100893 Contents lists available at ScienceDirect Regional Studies in Marine Science journal homepage: www.elsevier.com/locate/rsma Reef condition and protection of coral diversity and evolutionary history in the marine protected areas of Southeastern Dominican Republic ∗ Camilo Cortés-Useche a,b, , Aarón Israel Muñiz-Castillo a, Johanna Calle-Triviño a,b, Roshni Yathiraj c, Jesús Ernesto Arias-González a a Centro de Investigación y de Estudios Avanzados del I.P.N., Unidad Mérida B.P. 73 CORDEMEX, C.P. 97310, Mérida, Yucatán, Mexico b Fundación Dominicana de Estudios Marinos FUNDEMAR, Bayahibe, Dominican Republic c ReefWatch Marine Conservation, Bandra West, Mumbai 400050, India article info a b s t r a c t Article history: Changes in structure and function of coral reefs are increasingly significant and few sites in the Received 18 February 2019 Caribbean can tolerate local and global stress factors. Therefore, we assessed coral reef condition Received in revised form 20 September 2019 indicators in reefs within and outside of MPAs in the southeastern Dominican Republic, considering Accepted 15 October 2019 benthic cover as well as the composition, diversity, recruitment, mortality, bleaching, the conservation Available online 18 October 2019 status and evolutionary distinctiveness of coral species. In general, we found that reef condition Keywords: indicators (coral and benthic cover, recruitment, bleaching, and mortality) within the MPAs showed Coral reefs better conditions than in the unprotected area (Boca Chica). Although the comparison between the Caribbean Boca Chica area and the MPAs may present some spatial imbalance, these zones were chosen for Biodiversity the purpose of making a comparison with a previous baseline presented. -

Microbiomes of Gall-Inducing Copepod Crustaceans from the Corals Stylophora Pistillata (Scleractinia) and Gorgonia Ventalina
www.nature.com/scientificreports OPEN Microbiomes of gall-inducing copepod crustaceans from the corals Stylophora pistillata Received: 26 February 2018 Accepted: 18 July 2018 (Scleractinia) and Gorgonia Published: xx xx xxxx ventalina (Alcyonacea) Pavel V. Shelyakin1,2, Sofya K. Garushyants1,3, Mikhail A. Nikitin4, Sofya V. Mudrova5, Michael Berumen 5, Arjen G. C. L. Speksnijder6, Bert W. Hoeksema6, Diego Fontaneto7, Mikhail S. Gelfand1,3,4,8 & Viatcheslav N. Ivanenko 6,9 Corals harbor complex and diverse microbial communities that strongly impact host ftness and resistance to diseases, but these microbes themselves can be infuenced by stresses, like those caused by the presence of macroscopic symbionts. In addition to directly infuencing the host, symbionts may transmit pathogenic microbial communities. We analyzed two coral gall-forming copepod systems by using 16S rRNA gene metagenomic sequencing: (1) the sea fan Gorgonia ventalina with copepods of the genus Sphaerippe from the Caribbean and (2) the scleractinian coral Stylophora pistillata with copepods of the genus Spaniomolgus from the Saudi Arabian part of the Red Sea. We show that bacterial communities in these two systems were substantially diferent with Actinobacteria, Alphaproteobacteria, and Betaproteobacteria more prevalent in samples from Gorgonia ventalina, and Gammaproteobacteria in Stylophora pistillata. In Stylophora pistillata, normal coral microbiomes were enriched with the common coral symbiont Endozoicomonas and some unclassifed bacteria, while copepod and gall-tissue microbiomes were highly enriched with the family ME2 (Oceanospirillales) or Rhodobacteraceae. In Gorgonia ventalina, no bacterial group had signifcantly diferent prevalence in the normal coral tissues, copepods, and injured tissues. The total microbiome composition of polyps injured by copepods was diferent. -

St. Kitts Final Report
ReefFix: An Integrated Coastal Zone Management (ICZM) Ecosystem Services Valuation and Capacity Building Project for the Caribbean ST. KITTS AND NEVIS FIRST DRAFT REPORT JUNE 2013 PREPARED BY PATRICK I. WILLIAMS CONSULTANT CLEVERLY HILL SANDY POINT ST. KITTS PHONE: 1 (869) 765-3988 E-MAIL: [email protected] 1 2 TABLE OF CONTENTS Page No. Table of Contents 3 List of Figures 6 List of Tables 6 Glossary of Terms 7 Acronyms 10 Executive Summary 12 Part 1: Situational analysis 15 1.1 Introduction 15 1.2 Physical attributes 16 1.2.1 Location 16 1.2.2 Area 16 1.2.3 Physical landscape 16 1.2.4 Coastal zone management 17 1.2.5 Vulnerability of coastal transportation system 19 1.2.6 Climate 19 1.3 Socio-economic context 20 1.3.1 Population 20 1.3.2 General economy 20 1.3.3 Poverty 22 1.4 Policy frameworks of relevance to marine resource protection and management in St. Kitts and Nevis 23 1.4.1 National Environmental Action Plan (NEAP) 23 1.4.2 National Physical Development Plan (2006) 23 1.4.3 National Environmental Management Strategy (NEMS) 23 1.4.4 National Biodiversity Strategy and Action Plan (NABSAP) 26 1.4.5 Medium Term Economic Strategy Paper (MTESP) 26 1.5 Legislative instruments of relevance to marine protection and management in St. Kitts and Nevis 27 1.5.1 Development Control and Planning Act (DCPA), 2000 27 1.5.2 National Conservation and Environmental Protection Act (NCEPA), 1987 27 1.5.3 Public Health Act (1969) 28 1.5.4 Solid Waste Management Corporation Act (1996) 29 1.5.5 Water Courses and Water Works Ordinance (Cap. -
Checklist of Fish and Invertebrates Listed in the CITES Appendices
JOINTS NATURE \=^ CONSERVATION COMMITTEE Checklist of fish and mvertebrates Usted in the CITES appendices JNCC REPORT (SSN0963-«OStl JOINT NATURE CONSERVATION COMMITTEE Report distribution Report Number: No. 238 Contract Number/JNCC project number: F7 1-12-332 Date received: 9 June 1995 Report tide: Checklist of fish and invertebrates listed in the CITES appendices Contract tide: Revised Checklists of CITES species database Contractor: World Conservation Monitoring Centre 219 Huntingdon Road, Cambridge, CB3 ODL Comments: A further fish and invertebrate edition in the Checklist series begun by NCC in 1979, revised and brought up to date with current CITES listings Restrictions: Distribution: JNCC report collection 2 copies Nature Conservancy Council for England, HQ, Library 1 copy Scottish Natural Heritage, HQ, Library 1 copy Countryside Council for Wales, HQ, Library 1 copy A T Smail, Copyright Libraries Agent, 100 Euston Road, London, NWl 2HQ 5 copies British Library, Legal Deposit Office, Boston Spa, Wetherby, West Yorkshire, LS23 7BQ 1 copy Chadwick-Healey Ltd, Cambridge Place, Cambridge, CB2 INR 1 copy BIOSIS UK, Garforth House, 54 Michlegate, York, YOl ILF 1 copy CITES Management and Scientific Authorities of EC Member States total 30 copies CITES Authorities, UK Dependencies total 13 copies CITES Secretariat 5 copies CITES Animals Committee chairman 1 copy European Commission DG Xl/D/2 1 copy World Conservation Monitoring Centre 20 copies TRAFFIC International 5 copies Animal Quarantine Station, Heathrow 1 copy Department of the Environment (GWD) 5 copies Foreign & Commonwealth Office (ESED) 1 copy HM Customs & Excise 3 copies M Bradley Taylor (ACPO) 1 copy ^\(\\ Joint Nature Conservation Committee Report No. -

Review on Hard Coral Recruitment (Cnidaria: Scleractinia) in Colombia
Universitas Scientiarum, 2011, Vol. 16 N° 3: 200-218 Disponible en línea en: www.javeriana.edu.co/universitas_scientiarum 2011, Vol. 16 N° 3: 200-218 SICI: 2027-1352(201109/12)16:3<200:RHCRCSIC>2.0.TS;2-W Invited review Review on hard coral recruitment (Cnidaria: Scleractinia) in Colombia Alberto Acosta1, Luisa F. Dueñas2, Valeria Pizarro3 1 Unidad de Ecología y Sistemática, Departamento de Biología, Facultad de Ciencias, Pontificia Universidad Javeriana, Bogotá, D.C., Colombia. 2 Laboratorio de Biología Molecular Marina - BIOMMAR, Departamento de Ciencias Biológicas, Facultad de Ciencias, Universidad de los Andes, Bogotá, D.C., Colombia. 3 Programa de Biología Marina, Facultad de Ciencias Naturales, Universidad Jorge Tadeo Lozano. Santa Marta. Colombia. * [email protected] Recibido: 28-02-2011; Aceptado: 11-05-2011 Abstract Recruitment, defined and measured as the incorporation of new individuals (i.e. coral juveniles) into a population, is a fundamental process for ecologists, evolutionists and conservationists due to its direct effect on population structure and function. Because most coral populations are self-feeding, a breakdown in recruitment would lead to local extinction. Recruitment indirectly affects both renewal and maintenance of existing and future coral communities, coral reef biodiversity (bottom-up effect) and therefore coral reef resilience. This process has been used as an indirect measure of individual reproductive success (fitness) and is the final stage of larval dispersal leading to population connectivity. As a result, recruitment has been proposed as an indicator of coral-reef health in marine protected areas, as well as a central aspect of the decision-making process concerning management and conservation. -

White-Band Disease in <I>Acropora Palmata</I>
NOTES 639 BULLETIN OF MARINE SCIENCE. 32(2): 639-643. 1982 WHITE-BAND DISEASE IN ACROPORA PALMATA: IMPLICATIONS FOR THE STRUCTURE AND GROWTH OF SHALLOW REEFS W. B. Gladfelter In the last two decades a wide variety of organisms has been implicated in the destruction of reef-building corals (Glynn, 1973; Endean, 1976; Antonius, 1977). These fall generally into three categories: predators (Endean, 1973; Bak and van Eys, 1975; Reese, 1977), competitors for substrate (Glynn, 1973; Lang, 1973; Gladfelter et al., 1978) and disease-causing organisms (Garrett and DuckIow, 1975; Mitchell and Chet, 1975). In most instances the known impact of such organisms is restricted to portions of, or at most, single coral colonies. The impact of such organisms on whole reefs or systems has been documented only for the predatory starfish Acanthaster planci (Endean, 1973). In the present study we document the impact of another agent on a reef-wide scale. In much of the Caribbean Sea shallow windward reefs are dominated at depths of 1 to 5 m or more by the large branched coral Acropora palmata (Adey and Burke, 1976; Adey, 1978). In some such reefs >99% of living coral surface be- longs to this species (pers. obs.). In addition to quantitative dominance on such reefs this coral has one of the greatest rates of deposition of CaC03 per unit tissue surface (Gladfelter et al., 1978; Gladfelter and Gladfelter, unpublished) as well as high linear growth rates (5-10 cm/yr, Gladfelter et al., 1978) and consequently healthy A. palmata reefs exhibit some of the greatest measured reef growth rates (Adey and Burke, 1976 and unpublished calculations by Gladfelter and Gladfelter 2 of 10.3 kg CaC03/m /yr). -

Coral Disease Fact Sheet
Florida Department of Environmental Protection Coral Reef Conservation Program SEAFAN BleachWatch Program Coral Disease Fact Sheet About Coral Disease Like all other animals, corals can be affected by disease. Coral disease was first recognized in the Florida Keys and the Caribbean in the 1970s, and since that time disease reports have emerged from reefs worldwide. Naturally, there are background levels of coral disease but reports of elevated disease levels – often called disease outbreaks – have been increasing in both frequency and severity over the past few decades. Today, coral disease is recognized as a major driver of coral mortality and reef degradation. Coral disease can result from infection by microscopic organisms (such as bacteria or fungi) or can be caused by abnormal growth (akin to tumors). The origins or causes of most coral diseases are not known and difficult to determine. There is increasing evidence that environmental stressors, including increasing water temperatures, elevated nutrient levels, sewage input, sedimentation, overfishing, plastic pollution, and even recreational diving, are increasing the prevalence and Disease affecting Great Star Coral (Montastraea severity of coral diseases. There is also strong evidence cavernosa). Photo credit: Nikole Ordway-Heath (Broward County; 2016). that a combination of coral bleaching and disease can be particularly devastating to coral populations. This is likely due to corals losing a major source of energy during a bleaching event, reducing their ability to fight off or control disease agents. Coral disease is often identifiable by a change in tissue color or skeletal structure as well as progressive tissue loss. Tissue loss may originate from a single discrete spot, multiple discrete areas, or appear scattered throughout the colony. -

Growth and Survivorship of Scleractinian Coral Transplants And
Nova Southeastern University NSUWorks Oceanography Faculty Proceedings, Presentations, Department of Marine and Environmental Sciences Speeches, Lectures 2006 Growth and Survivorship of Scleractinian Coral Transplants and the Effectiveness of Plugging Core Holes in Transplant Donor Colonies Elizabeth Glynn Fahy Nova Southeastern University Richard E. Dodge Nova Southeastern University, [email protected] Daniel P. Fahy Nova Southeastern University, [email protected] T. Patrick Quinn Nova Southeastern University David S. Gilliam Nova Southeastern University, [email protected] See next page for additional authors Follow this and additional works at: http://nsuworks.nova.edu/occ_facpresentations Part of the Marine Biology Commons, and the Oceanography and Atmospheric Sciences and Meteorology Commons NSUWorks Citation Fahy, Elizabeth Glynn; Dodge, Richard E.; Fahy, Daniel P.; Quinn, T. Patrick; Gilliam, David S.; and Spieler, Richard E., "Growth and Survivorship of Scleractinian Coral Transplants and the Effectiveness of Plugging Core Holes in Transplant Donor Colonies" (2006). Oceanography Faculty Proceedings, Presentations, Speeches, Lectures. Paper 44. http://nsuworks.nova.edu/occ_facpresentations/44 This Conference Proceeding is brought to you for free and open access by the Department of Marine and Environmental Sciences at NSUWorks. It has been accepted for inclusion in Oceanography Faculty Proceedings, Presentations, Speeches, Lectures by an authorized administrator of NSUWorks. For more information, please contact [email protected]. Authors Elizabeth Glynn Fahy, Richard E. Dodge, Daniel P. Fahy, T. Patrick Quinn, David S. Gilliam, and Richard E. Spieler This conference proceeding is available at NSUWorks: http://nsuworks.nova.edu/occ_facpresentations/44 Growth and survivorship of scleractinian coral transplants and the effectiveness of plugging core holes in transplant donor colonies Elizabeth Glynn FAHY*, Richard E. -

High Density of Diploria Strigosa Increases
HIGH DENSITY OF DIPLORIA STRIGOSA INCREASES PREVALENCE OF BLACK BAND DISEASE IN CORAL REEFS OF NORTHERN BERMUDA Sarah Carpenter Department of Biology, Clark University, Worcester, MA 01610 ([email protected]) Abstract Black Band Disease (BBD) is one of the most widespread and destructive coral infectious diseases. The disease moves down the infected coral leaving complete coral tissue degradation in its wake. This coral disease is caused by a group of coexisting bacteria; however, the main causative agent is Phormidium corallyticum. The objective of this study was to determine how BBD prominence is affected by the density of D. strigosa, a common reef building coral found along Bermuda coasts. Quadrats were randomly placed on the reefs at Whalebone Bay and Tobacco Bay and then density and percent infection were recorded and calculated. The results from the observations showed a significant, positive correlation between coral density and percent infection by BBD. This provides evidence that BBD is a water borne infection and that transmission can occur at distances up to 1m. Information about BBD is still scant, but in order to prevent future damage, details pertaining to transmission methods and patterns will be necessary. Key Words: Black Band Disease, Diploria strigosa, density Introduction Coral pathogens are a relatively new area of study, with the first reports and descriptions made in the 1970’s. Today, more than thirty coral diseases have been reported, each threatening the resilience of coral communities (Green and Bruckner 2000). The earliest identified infection was characterized by a dark band, which separated the healthy coral from the dead coral.