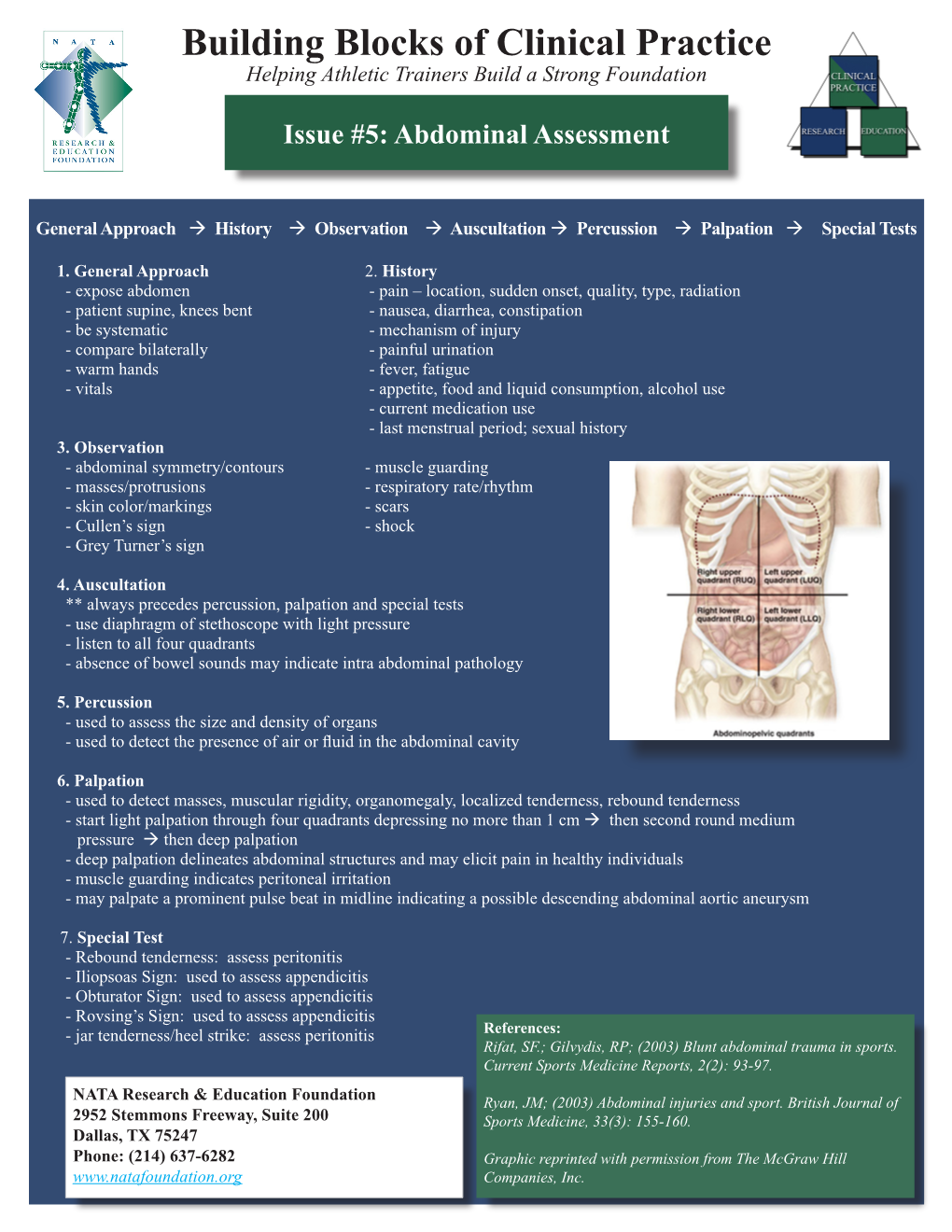
Building Blocks of Clinical Practice Helping Athletic Trainers Build a Strong Foundation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Congenital Diarrheal Disorders: an Updated Diagnostic Approach
4168 Int. J. Mol. Sci.2012, 13, 4168-4185; doi:10.3390/ijms13044168 OPEN ACCESS International Journal of Molecular Sciences ISSN 1422-0067 www.mdpi.com/journal/ijms Review Congenital Diarrheal Disorders: An Updated Diagnostic Approach Gianluca Terrin 1, Rossella Tomaiuolo 2,3,4, Annalisa Passariello 5, Ausilia Elce 2,3, Felice Amato 2,3, Margherita Di Costanzo 5, Giuseppe Castaldo 2,3 and Roberto Berni Canani 5,6,* 1 Department of Gynecology-Obstetrics and Perinatal Medicine, University of Rome “La Sapienza”, Viale del Policlinico 1, Rome 00161, Italy; E-Mail: [email protected] 2 CEINGE-Advanced Biotechnology, Via Comunale Margherita, Naples 80131, Italy; E-Mails: [email protected] (R.T.); [email protected] (A.E.); [email protected] (F.A.); [email protected] (G.C.) 3 Department of Biochemistry and Biotechnology, University of Naples “Federico II”, Via Pansini 5, Naples 80131, Italy 4 Biotechnology Science, University of Naples “Federico II”, Via De Amicis, Naples 80131, Italy 5 Department of Pediatrics, University of Naples “Federico II”, Via Pansini 5, Naples 80131, Italy; E-Mails: [email protected] (A.P.); [email protected] (M.D.C.) 6 European Laboratory for the Investigation of Food Induced Diseases, University of Naples “Federico II”, Via Pansini 5, Naples 80131, Italy * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel./Fax: +39-0817462680. Received: 18 February 2012; in revised form: 2 March 2012 / Accepted: 19 March 2012 / Published: 29 March 2012 Abstract: Congenital diarrheal disorders (CDDs) are a group of inherited enteropathies with a typical onset early in the life. -

Colonoscopic Review and Surgical Approach in the Management of Colorectal Carcinoma–A Retrospective Study of 50 Cases
Original Paper Colonoscopic Review and Surgical Approach in the Management of Colorectal Carcinoma–A Retrospective Study of 50 cases 1 2 3 Ershad-ul-Quadir M , Rahman MMM , Rahman MM Abstract Introduction: There is no exact statistics about the with abdominal pain 12 out of 22 cases (56%) and incidence of colorectal cancer in Bangladesh. weight loss 15 cases (68%). For left colon cancer According to National Cancer Institute, London, it is commonest symptom was weight loss and weakness the 2nd most common cancer affecting more than and altered bowel habit. Almost all cases with rectal 30,000 people in each year. As many patients with carcinoma presented with bleeding per rectum. colon cancer do not develop symptoms until it is advanced and detection in early stage can only be Conclusion: About 50% of lesions were found in achieved by screening of asymptomatic person. recto-sigmoid junction and male: female ratio was Maximum patients present lately with distance 1.9:1. All efforts and modern technology should be metastases when there is nothing to treat except applied for early detection and treatment. The palliative therapy. survival rate is usually very poor in rectal carcinoma. In this study most of the cases were subjected to Objectives: To identify the risk factors, early post operative Chemo and Radiotherapy, but more symptoms, signs, treatment modalities, operative were treated with neoadjuvant chemoradiation for outcome, morbidity and mortality rate. down staging. The need for early detection of Colorectal Carcinoma (CRC) should be stressed in Materials and Methods: This retrospective study the form of screening patient awareness and was carried out at CMH Dhaka during August 2002 understanding about symptomatology. -

General Signs and Symptoms of Abdominal Diseases
General signs and symptoms of abdominal diseases Dr. Förhécz Zsolt Semmelweis University 3rd Department of Internal Medicine Faculty of Medicine, 3rd Year 2018/2019 1st Semester • For descriptive purposes, the abdomen is divided by imaginary lines crossing at the umbilicus, forming the right upper, right lower, left upper, and left lower quadrants. • Another system divides the abdomen into nine sections. Terms for three of them are commonly used: epigastric, umbilical, and hypogastric, or suprapubic Common or Concerning Symptoms • Indigestion or anorexia • Nausea, vomiting, or hematemesis • Abdominal pain • Dysphagia and/or odynophagia • Change in bowel function • Constipation or diarrhea • Jaundice “How is your appetite?” • Anorexia, nausea, vomiting in many gastrointestinal disorders; and – also in pregnancy, – diabetic ketoacidosis, – adrenal insufficiency, – hypercalcemia, – uremia, – liver disease, – emotional states, – adverse drug reactions – Induced but without nausea in anorexia/ bulimia. • Anorexia is a loss or lack of appetite. • Some patients may not actually vomit but raise esophageal or gastric contents in the absence of nausea or retching, called regurgitation. – in esophageal narrowing from stricture or cancer; also with incompetent gastroesophageal sphincter • Ask about any vomitus or regurgitated material and inspect it yourself if possible!!!! – What color is it? – What does the vomitus smell like? – How much has there been? – Ask specifically if it contains any blood and try to determine how much? • Fecal odor – in small bowel obstruction – or gastrocolic fistula • Gastric juice is clear or mucoid. Small amounts of yellowish or greenish bile are common and have no special significance. • Brownish or blackish vomitus with a “coffee- grounds” appearance suggests blood altered by gastric acid. -

Colorectal Cancer Symptoms
Colorectal Symptoms - Suspected Colorectal Cancer Disclaimer This pathway is for symptomatic patients. see also National Bowel Cancer Screening Program (NBCSP). Contents Disclaimer ............................................................................................................................................................................................ 1 Background .................................................................................................................................................. 2 About colorectal symptoms ......................................................................................................................................................... 2 Assessment ................................................................................................................................................... 2 Rectal bleeding .................................................................................................................................................................................. 2 Gastrointestinal history .................................................................................................................................................................. 2 Previous procedures ........................................................................................................................................................................ 2 Family history of bowel cancer ................................................................................................................................................... -

Acute Abdomen
Acute abdomen: Shaking down the Acute abdominal pain can be difficult to diagnose, requiring astute assessment skills and knowledge of abdominal anatomy 2.3 ANCC to discover its cause. We show you how to quickly and accurately CONTACT HOURS uncover the clues so your patient can get the help he needs. By Amy Wisniewski, BSN, RN, CCM Lehigh Valley Home Care • Allentown, Pa. The author has disclosed that she has no significant relationships with or financial interest in any commercial companies that pertain to this educational activity. NIE0110_124_CEAbdomen.qxd:Deepak 26/11/09 9:38 AM Page 43 suspects Determining the cause of acute abdominal rapidly, indicating a life-threatening process, pain is often complex due to the many or- so fast and accurate assessment is essential. gans in the abdomen and the fact that pain In this article, I’ll describe how to assess a may be nonspecific. Acute abdomen is a patient with acute abdominal pain and inter- general diagnosis, typically referring to se- vene appropriately. vere abdominal pain that occurs suddenly over a short period (usually no longer than What a pain! 7 days) and often requires surgical interven- Acute abdominal pain is one of the top tion. Symptoms may be severe and progress three symptoms of patients presenting in www.NursingMadeIncrediblyEasy.com January/February 2010 Nursing made Incredibly Easy! 43 NIE0110_124_CEAbdomen.qxd:Deepak 26/11/09 9:38 AM Page 44 the ED. Reasons for acute abdominal pain Visceral pain can be divided into three Your patient’s fall into six broad categories: subtypes: age may give • inflammatory—may be a bacterial cause, • tension pain. -

POEMS Syndrome: an Atypical Presentation with Chronic Diarrhoea and Asthenia
European Journal of Case Reports in Internal Medicine POEMS Syndrome: an Atypical Presentation with Chronic Diarrhoea and Asthenia Joana Alves Vaz1, Lilia Frada2, Maria Manuela Soares1, Alberto Mello e Silva1 1 Department of Internal Medicine, Egas Moniz Hospital, Lisbon, Portugal 2 Department of Gynecology and Obstetrics, Espirito Santo Hospital, Evora, Portugal Doi: 10.12890/2019_001241 - European Journal of Case Reports in Internal Medicine - © EFIM 2019 Received: 28/07/2019 Accepted: 13/11/2019 Published: 16/12/2019 How to cite this article: Alves Vaz J, Frada L, Soares MM, Mello e Silva A. POEMS syndrome: an atypical presentation with chronic diarrhoea and astenia. EJCRIM 2019;7: doi:10.12890/2019_001241. Conflicts of Interests: The Authors declare that there are no competing interest This article is licensed under a Commons Attribution Non-Commercial 4.0 License ABSTRACT POEMS syndrome is a rare paraneoplastic condition associated with polyneuropathy, organomegaly, monoclonal gammopathy, endocrine and skin changes. We report a case of a man with Castleman disease and monoclonal gammopathy, with a history of chronic diarrhoea and asthenia. Gastrointestinal involvement in POEMS syndrome is not frequently referred to in the literature and its physiopathology is not fully understood. Diagnostic criteria were met during hospitalization but considering the patient’s overall health condition, therapeutic options were limited. Current treatment for POEMS syndrome depends on the management of the underlying plasma cell disorder. This report outlines the importance of a thorough review of systems and a physical examination to allow an attempted diagnosis and appropriate treatment. LEARNING POINTS • POEMS syndrome should be suspected in the presence of peripheral polyneuropathy associated with monoclonal gammopathy; diagnostic workup is challenging and delay in treatment is very common. -

Missed Appendicitis Diagnosis: a Case Report Jocelyn Cox, Bphed, DC1 Guy Sovak, Phd2
ISSN 0008-3194 (p)/ISSN 1715-6181 (e)/2015/294–299/$2.00/©JCCA 2015 Missed appendicitis diagnosis: A case report Jocelyn Cox, BPhEd, DC1 Guy Sovak, PhD2 Objective: The purpose of this case report is to highlight Objectif : Cette étude de cas vise à souligner la nécessité and emphasize the need for an appropriate and thorough d’une liste appropriée et détaillée de diagnostics list of differential diagnoses when managing patients, as différentiels lors de la gestion des patients, car il n’est it is insufficient to assume cases are mechanical, until pas suffisant de supposer que les cas sont d’ordre proven non-mechanical. There are over 250,000 cases mécanique, jusqu’à la preuve du contraire. Il y a plus de of appendicitis annually in the United States. Of these 250 000 cas d’appendicite par an aux États-Unis. Parmi cases, <50% present with classic signs and symptoms of ces cas, < 50 % présentent des signes et des symptômes pain in the right lower quadrant, mild fever and nausea. classiques de douleur dans le quadrant inférieur droit, It is standard for patients who present with appendicitis de fièvre légère et de nausées. Il est normal qu’un to be managed operatively with a laparoscopic patient qui se présente avec une appendicite soit géré appendectomy within 24 hours, otherwise the risk of par une intervention chirurgicale (appendicectomie complications such as rupture, infection, and even death par laparoscopie) dans les 24 heures, sinon le risque increases dramatically. de complications, telles que rupture, infection et décès, Clinical Features: This is a retrospective case report augmente considérablement. -

A RISK MANAGEMENT APPROACH to ABDOMINAL PAIN in PRIMARY CARE Symptoms Most Predictive of Appendicitis Are Right Lower Torsion
EMERGENCY MEDICINE – WHAT THE FAMILY PHYSICIAN CAN TREAT UNIT NO. 6 A RISK MANAGEMENT APPROACH TO ABDOMINAL PAIN IN PRIMARY CARE Symptoms most predictive of appendicitis are right lower torsion. inammatory disease (PID) and appendicitis can be virtually for a patient with abdominal pain yields little information, aneurysm or a dissection in elderly patients presenting with quadrant pain (RLQ), and migration of pain from the indistinguishable via the anterior abdominal examination, and unless one is specically looking for air-uid levels indicative of ank pain. Up to one-third of patients with abdominal aortic SUMMARY Dr Lim Jia Hao periumbilical region to RLQ. Anorexia, which has been Palpation should begin with light palpation to localise the it will be the pelvic examination that can reveal the true intestinal obstruction in a patient exhibiting obstructive aneurysms may have haematuria, which can further confound classically taught to be useful in diagnosing appendicitis has region of tenderness and to elicit guarding. Deep palpation aetiology. While both conditions can result in painful cervical symptoms. Abnormal calcications associated with gallstone the physician. Detection of vascular emergencies can be dicult e assessment of abdominal pain in the primary healthcare been found to have little predictive value.6, 7 A gynaecological follows for the detection of organomegaly and masses. However, motion and adnexal tenderness, it is the presence of disease, kidney stones, appendicoliths, as well as aortic if the diagnosis is not entertained from the outset. setting will require the family physician to employ the ABSTRACT just as important to recognise the patients that require a referral and sexual history should be obtained when evaluating women, this can be deeply distressing to the patient with severe mucopurulent discharge from the cervix that will allow the calcications can sometimes be seen on the plain lm as well. -

Coexistence of Pneumothorax and Chilaiditi Sign: a Case Report
Asian Pac J Trop Biomed 2014; 4(1): 75-77 75 Contents lists available at ScienceDirect Asian Pacific Journal of Tropical Biomedicine journal homepage: www.elsevier.com/locate/apjtb Document heading doi:10.1016/S2221-1691(14)60212-4 2014 by the Asian Pacific Journal of Tropical Biomedicine. All rights reserved. 襃 Coexistence of pneumothorax and chilaiditi sign: A case report 1 1 2 1 1 1 1 Tangri Nitin *, Singhal Sameer , Sharma Priyanka , Mehta Dinesh , Bansal Sachin , Bhushan Neeraj , Singla Sulbha , Singh 1 Puneet 1Department of Respiratory Medicine, M.M Institute of Medical Sciences & Research, Mullana, Ambala, Haryana, India 2Department of Biochemistry, M.M Institute of Medical Sciences & Research, Mullana, Ambala, Haryana, India PEER REVIEW ABSTRACT Peer reviewer We present a case of 50 year old male patient withfi coexistence of Pneumothorax and Chilaiditi Dr Sumit Mehra, MD (Pulmonary sign. Chilaiditi sign is an incidental radiographic nding of a usually asymptomatic condition Medicine) Fellowship Sleep Medicine “in which a part of in”testine is located between the liver and diaphragm; however, the term (AASM, USA), Department of medicine, Chilaiditi syndrome is used for symptomatic hepatodiaphragmatic interposition. The patient H H H ervey bay ospital, ervey bay, had no symptoms of abdominal pain, constipation, diarrhea, ofir emesis. Incidentally, Chilaiditi Queensland Australia. sign was diagnosed on chest radiography. Pneumothorax is de ned as air in the pleural space. Tel: +6107 4325 6666, +6104 7741 2243 Pneumothoraces are classified as spontaneous or traumatic. Spontaneous pneumothorax is E-mail: Sumitmeh2000@yahoo labelled as primary when no underlying lung disease is present, or secondary, when it is [email protected] associated with pre-existing lung disease. -

Acute Abdomen in the Emergency Department
IAJPS 2018, 05 (11), 11847-11852 Muhanad Khalid Kondarji et al ISSN 2349-7750 CODEN [USA]: IAJPBB ISSN: 2349-7750 INDO AMERICAN JOURNAL OF PHARMACEUTICAL SCIENCES Available online at: http://www.iajps.com Review Article ACUTE ABDOMEN IN THE EMERGENCY DEPARTMENT Muhanad Khalid Kondarji1, Mohammed Khalid Kondarji2, Abdullah Mohammed Alzahrani1, Hussa Ali Alrashid2, Turki Ghaleb Al Ahmadi1, Faisal Mohammed Hinkish3, Fisal Amjed Abdulaziz4, Hamoud Marzuq Alrougi1, Rayan Tareq Alrefai1, Hassan Ibrahim Alasmari1 1 King Fahd Hospital, Jeddah 2 King Abdulaziz University 3 Althaghr Hospital 4 Taibah University Abstract: Introduction: 7% of the patients come to the emergency department with the chief complain of acute abdominal pain. They can have minor causes, but also be due to very serious causes, which requires urgency in care and serious diagnosis and management. Acute abdominal emergencies are a big contributor to morbidity and mortality. Aim of the work: In this study, we aim to understand the standard way to approach a case of acute abdominal pain in the emergency department. Methodology: we conducted this review using a comprehensive search of MEDLINE, PubMed and EMBASE from January 1970 to March 2017. The following search terms were used: acute abdomen, abdominal pain management, clinical evaluation of abdominal pain, management acute abdomen Conclusion: Acute abdomen is an extremely common presentation in the emergency department. However, it is not easy to assess, diagnose, and manage. Rate of misdiagnoses and fatalities are high; therefore, physicians should always consider all possible and start with more serious etiologies. Proper assessment and management of acute abdomen can lead to significant improvement of morbidity and mortality. -

An Observational Study of Abdominal Organ Involvement Detected By
Published online: 2019-04-05 Original Article An observational study of abdominal organ involvement detected by ultrasound and computed tomography in children suffering from lymphoreticular malignancy at a tertiary care hospital in Eastern India ABSTRACT Introduction: Abdominal organs are usually involved in lymphoreticular malignancies (LRM), and the detection is crucial for Initial staging, determination of the location and extent of disease, and is the hallmark for the choice of treatment. At present, the established radiological technique for staging Hodgkin’s disease is computed tomography (CT) and ultrasonography (USG) in our country. Objective: The objective of the study was to evaluate the pattern of abdominal organ involvement in childhood LRM by USG and CT and to analyze the findings. Methods: The study included 121 children with newly diagnosed childhood LRM who underwent real time USG and contrast enhanced CT scan. The records of the US and CT scanning were analyzed with respect to size, shape, margins, echogenicity /density pattern of various abdominal organs and lymph nodes to evaluate the extent and pattern of abdominal organ involvement by the disease process. Results: Out of 121 cases of LRM, US detected significant portal lymphadenopathy in 9 (7.44%) cases where CT detected enlarged portal nodes in only 3 and missed in 6 cases. However in the retroperitoneal lynphadenopathy CT scored over US, as CT detected 16 (13.22%) cases as against 13 (10.74%) cases detected by US. Conclusion: In our study we observed abdominal organs are commonly involved at the time of initial presentation in childhood LRM, with diffuse organomegaly being commoner than focal lesions. -

Approach to Nausea and Vomiting
Approach to Nausea and Vomiting By James F. Graumlich, MD, FACP Associate Professor of Medicine and Clinical Pharmacology University of Illinois College of Medicine Peoria, IL 61637 Approach to Nausea and Vomiting Objectives: At the end of this session, the learner will be able to List the causes of nausea and vomiting based on organ systems Describe the diagnostic approach to nausea and vomiting based on the history and physical exam and diagnostic laboratory and radiographic tests Discuss the pharmacologic interventions available for the treatment of nausea and vomiting Describe interventions to prevent complications of nausea and vomiting References: Gan TJ. Postoperative nausea and vomiting--can it be eliminated? JAMA. 287(10): 1233-6, 2002 Mar 13. Tramer MR. A rational approach to the control of postoperative nausea and vomiting: evidence from systematic reviews. Part II. Recommendations for prevention and treatment, and research agenda. Acta Anaesthesiologica Scandinavica. 45(1): 14-9, 2001 Jan. Apfel CC, Korttila K, Abdalla M, Kerger H, Turan A, Vedder I, Zernak C, Danner K, Jokela R, Pocock SJ, Trenkler S, Kredel M, Biedler A, Sessler DI, Roewer N; IMPACT Investigators. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med. 2004 Jun 10;350(24):2441-51. Scorza K, Williams A, Phillips D, Shaw J. Evaluation of Nausea and Vomiting Am Fam Physician 2007;76:76-84 Section I Directions: Begin by reading the references. Use the information from the background article (and other sources as appropriate) to answer the questions following each case. The questions are "open-ended" and therefore there are no right or wrong answers.