Infective Endocarditis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CASE REPORTS Supraventricular Tachycardia As the Initial
http://crim.sciedupress.com Case Reports in Internal Medicine, 2015, Vol. 2, No. 3 CASE REPORTS Supraventricular tachycardia as the initial presentation of bacterial infective endocarditis: A rare case report Wei-Tsung Wu1, Hung-Ling Huang2, Ho-Ming Su1, 3, Tsung-Hsien Lin1, 3, Kun-Tai Lee1, 3, Sheng-Hsiung Sheu1, 3, Po-Chao Hsu1, 3 1. Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan, ROC. 2. Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan, ROC. 3. Department of Internal Medicine, Faculty of Medicine, School of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan, ROC Correspondence: Po-Chao Hsu. Address: Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, 100 Tzyou 1st Road, Kaohsiung. 80708, Taiwan, ROC. Email: [email protected] Received: May 19, 2015 Accepted: June 15, 2015 Online Published: June 17, 2015 DOI: 10.5430/crim.v2n3p26 URL: http://dx.doi.org/10.5430/crim.v2n3p26 Abstract Infective endocarditis (IE) is an infection of the heart valves or the heart’s inner lining. The clinical symptoms of infectious endocarditis vary considerably, some are subtle and non-specific, which make the diagnosis difficult or the signs misleading. In some cases cardiac symptoms are associated with intra cardiac extension of the infection, including murmur, conduction blocks and congestive heart failure. However, there was no literature description of supraventricular tachycardia (SVT) as the initial presentation of IE. Herein we report a case of bacterial IE with SVT as the initial presentation of disease, which finally leaded to catastrophic outcome. -

Myocarditis, Pericarditis Cardiomyopathies
Endocarditis, myocarditis, pericarditis. Cardiomyopathies Attila Zalatnai Endocarditis: inflammation of the endocardium, especially the valves 1. Infective endocarditis: (bacteria, fungi) Predisposing factors: - septicemia - valve malformations - deformed, calcified valves - arteficial valve implantation - previous rheumatic fever - peridontal, periapical foci! Most important causative agents: Strcc. viridans Enterococcus (Str. fecalis) Staphylococcus aureus Candida species Morphology: Vegetations Valve destruction Both Complications: embolization (septic emboli, septic abscesses) sepsis „mycotic aneurysms”, subarachnoidal hemorrhage acute left sided heart failure (regurgitation, chorda tendinea rupture) healing by scarring and calcification VITIUM stenosis insufficiency combined 2. Non-infective endocarditis: verrucous endocarditis (rheumatic fever) SLE (Libman-Sacks endocarditis) – atypical „marantic” endocarditis - paraneoplastic Myocarditis: an inflammatory infiltrate (helper T-cells, macrophages) of the myocardium with necrosis and/or degeneration of adjacent myocytes Genetic and environmental disposition + causative mechanisms Direct cytotoxic Aberrant effect of infectious induction of causative agents apoptosis Cytokine expression in the myocardium Secondary autoimmune (TNF-alpha, NOS) mechanisms Etiology of the myocarditis - I. Infectious origin - VIRUSES (Coxsackie B, enterovirus, influenza, CMV, EBV, HSV… Coxsackie A9 – self limiting disease; Coxsackie B3 – severe, sometimes lethal) - bacteria (Diphtheria, tbc, clostridia, staphylococci, -

Infective Endocarditis: a Focus on Oral Microbiota
microorganisms Review Infective Endocarditis: A Focus on Oral Microbiota Carmela Del Giudice 1 , Emanuele Vaia 1 , Daniela Liccardo 2, Federica Marzano 3, Alessandra Valletta 1, Gianrico Spagnuolo 1,4 , Nicola Ferrara 2,5, Carlo Rengo 6 , Alessandro Cannavo 2,* and Giuseppe Rengo 2,5 1 Department of Neurosciences, Reproductive and Odontostomatological Sciences, Federico II University of Naples, 80131 Naples, Italy; [email protected] (C.D.G.); [email protected] (E.V.); [email protected] (A.V.); [email protected] (G.S.) 2 Department of Translational Medical Sciences, Medicine Federico II University of Naples, 80131 Naples, Italy; [email protected] (D.L.); [email protected] (N.F.); [email protected] (G.R.) 3 Department of Advanced Biomedical Sciences, University of Naples Federico II, 80131 Naples, Italy; [email protected] 4 Institute of Dentistry, I. M. Sechenov First Moscow State Medical University, 119435 Moscow, Russia 5 Istituti Clinici Scientifici ICS-Maugeri, 82037 Telese Terme, Italy 6 Department of Prosthodontics and Dental Materials, School of Dental Medicine, University of Siena, 53100 Siena, Italy; [email protected] * Correspondence: [email protected]; Tel.: +39-0817463677 Abstract: Infective endocarditis (IE) is an inflammatory disease usually caused by bacteria entering the bloodstream and settling in the heart lining valves or blood vessels. Despite modern antimicrobial and surgical treatments, IE continues to cause substantial morbidity and mortality. Thus, primary Citation: Del Giudice, C.; Vaia, E.; prevention and enhanced diagnosis remain the most important strategies to fight this disease. In Liccardo, D.; Marzano, F.; Valletta, A.; this regard, it is worth noting that for over 50 years, oral microbiota has been considered one of the Spagnuolo, G.; Ferrara, N.; Rengo, C.; significant risk factors for IE. -

Infective Endocarditis
. Infective endocarditis Information for patients You may have recently been diagnosed or treated for a heart condition called infective endocarditis. Or you may wonder if you are at risk of this condition. This leaflet explains the causes and symptoms of infective endocarditis, and what to do if you have any. It describes treatments that you might have and how you should recover after treatment. This leaflet also has information on preventing an episode of infective endocarditis in the future. There is also a list of hospital contacts and sources of further information and support. What is infective endocarditis? Infective endocarditis is an infection of the inner lining or valves of the heart. It is caused by bacteria entering the bloodstream and sticking to heart structures. It is very rare, affecting 30 people in every one million each year. It can be serious, especially if complications develop. Early diagnosis, early antibiotic treatment and early surgery (if needed) are vital. Treatment requires hospital admission and a course of antibiotics through a drip. Up to 50% of patients may need surgery to repair or replace a damaged heart valve. In the most severe cases, the risk of death can be 1 in 5. What causes infective endocarditis? Your heart is usually well protected against infection and most bacteria pass by harmlessly. If your heart valves are damaged or you have an artificial valve, it is easier for bacteria to “sneak past” your normal immune defence and take root. This can mean that: • Bacteria – or occasionally fungi – settle on the inner lining of your heart (the endocardium). -
Infective Endocarditis
Infective Endocarditis Infective Endocarditis • Definitions and Historical Perspective • Epidemiology • Pathogenesis • Clinical Presentation and Diagnosis • Therapy • Prevention MID 9 Infective Endocarditis: Definitions • A microbial infection of a cardiac valve or the endocardium caused by bacteria, fungi, or chlamydia • Often categorized as acute or subacute based on the rapidity of the clinical course – Alternatively described by type of risk factor e.g., nosocomial, prosthetic valve, intravenous drug use - associated • Pathological findings include the presence of friable valvular vegetations containing bacteria, fibrin and inflammatory cells. There is often valvular destruction with extension to adjacent structures. – Embolic lesions may demonstrate similar findings MID 9 Historical Perspective • “.. A concretion larger than a pigeon’s egg; contained in the left auricle.” Burns, 1809 • Osler’s Gulstonian lectures provided the 1st comprehensive overview of the disease • Lewis and Grant (1923) were the first to link a transient bacteremia with deformed valves esastet as the two opedo predomin an t risk factors for infection • The introduction of penicillin marked the first successful therapy for this otherwise fatal infection Sir William Osler Epidemiology of Endocarditis • Incidence the same or slightly increased – 1.7-6.2/100,000 deppgending on the p ppopulation • The age of subjects with endocarditis has increased over the past 60 years (30-40 to 47-69) • There has been a major shift in nature of underlying valvular disorders • -
Recommendations for the Practice of Echocardiography in Infective Endocarditis
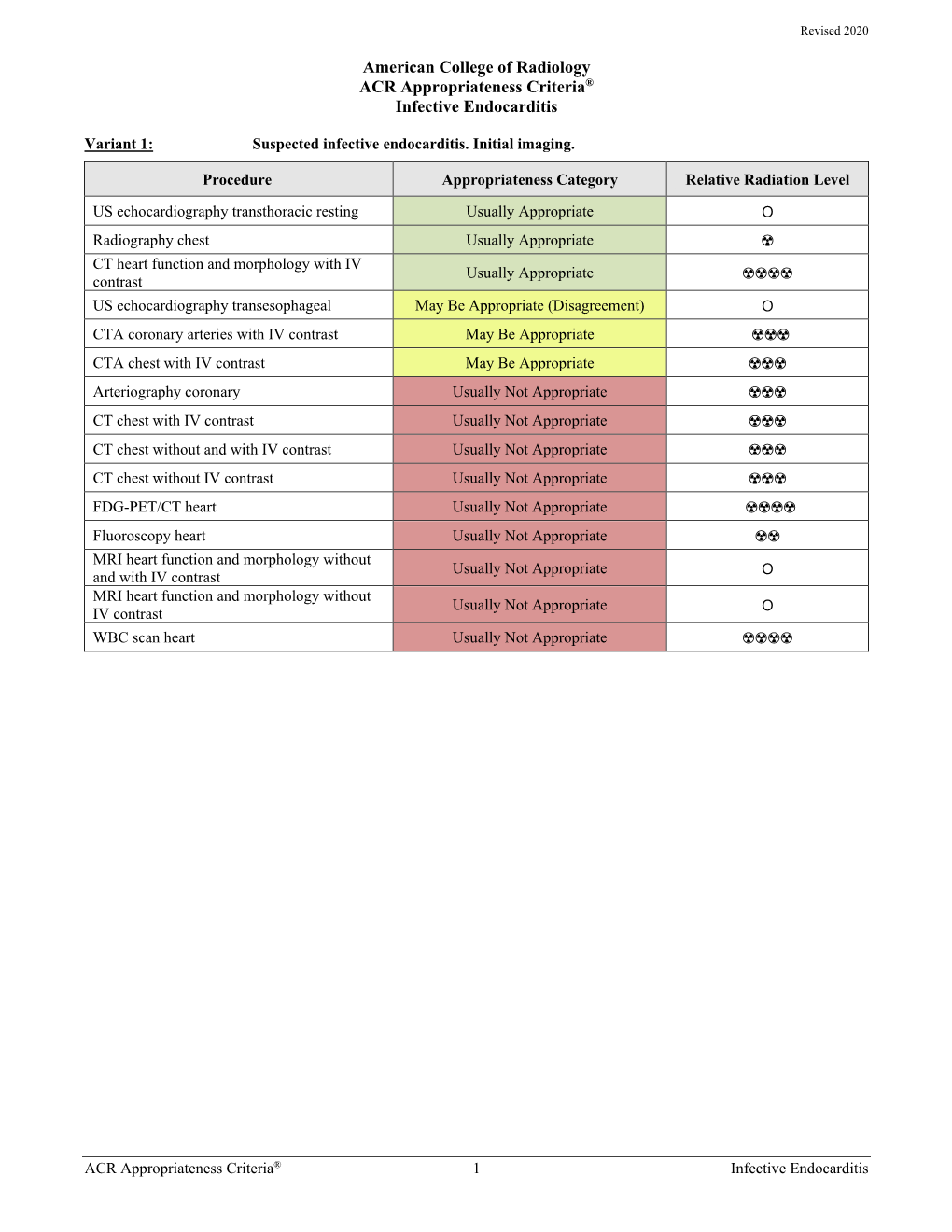
European Journal of Echocardiography (2010) 11, 202–219 RECOMMENDATIONS doi:10.1093/ejechocard/jeq004 Recommendations for the practice of echocardiography in infective endocarditis Gilbert Habib (France)*, Luigi Badano (Italy), Christophe Tribouilloy (France), Isidre Vilacosta (Spain), and Jose Luis Zamorano (Spain) Scientific Committee: Maurizio Galderisi (Italy), Jens-Uwe Voigt (Belgium), Rosa Sicari (Italy) Document Reviewers: Bernard Cosyns (Belgium), Kevin Fox (UK), Svend Aakhus (Norway) On behalf of the European Association of Echocardiography Service de Cardiologie, CHU La Timone, Bd Jean Moulin, 13005 Marseille, France Received 20 December 2009; accepted after revision 30 December 2009 Echocardiography plays a key role in the assessment of infective endocarditis (IE). It is useful for the diagnosis of endocarditis, the assessment of the severity of the disease, the prediction of short- and long-term prognosis, the prediction of embolic events, and the follow-up of patients under specific antibiotic therapy. Echocardiography is also useful for the diagnosis and management of the complications of IE, helping the physician in decision-making, particularly when a surgical therapy is considered. Finally, intraoperative echocardiography must be performed in IE to help the surgeon in the assessment and management of patients with IE during surgery. The current ‘recommendations for the practice of echocardiography in infective endocarditis’ aims to provide both an updated summary concerning the value and limitations of echocardiography in IE, and clear and simple recommendations for the optimal use of both transthoracic and transoesophageal echocardiography in IE. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Echocardiography † Endocarditis † Valve disease Table of Contents Introduction . 202 2. Echocardiographic follow-up under therapy . 212 Chapter 1: Echocardiography for the diagnosis of infective 3. -

Hickam's Dictum Vs. Occam's Razor in Diagnosing Subacute Bacterial Infective Endocarditis
Hickam’s Dictum Vs. Occam’s Razor in Diagnosing Subacute Bacterial Infective Endocarditis Bella Kalayilparampil, MS4; Stacy Philip, MS4; Sara Alhaj, MS4; Ahmad Hallak, MD; Tarek Naguib, MD Department of Internal Medicine Texas Tech University Health Sciences Center, Amarillo Introduction Discussion Infective endocarditis (IE) is a fatal time-dependent diagnosis that clinicians should suspect in patients with ● Each organ pathology was considered to be the primary cause of our patient’s symptoms, without considering prosthetic heart valves, implanted intracardiac devices, and those with a history of intravenous (IV) drug use, infective endocarditis as a unifying cause immunosuppression, or recent dental or surgical procedures. Subtleties in the presentation of IE pose a ○ Using Hickam’s dictum reasoning to separately explain this patient’s presentation of CVA, pancytopenia, AKI, challenge to clinicians in the diagnostic process. IE can present as an acute, rapidly progressive infection or in dysphagia, and B12 deficiency, rather than utilizing an Occam’s razor approach to identify one encompassing an insidious, subacute, and chronic nature with non-specific symptoms. Common signs and symptoms include diagnosis to link these findings, led to a delay in proper management. fever and cardiac murmur in the vast majority of cases. However, splenomegaly, splinter hemorrhages, and Figure 1: Valve vegetation as seen ● Patient’s first hospitalization consisted of: on TEE ○ Gait disturbances and dysphagia → suggestive of CVA petechial hemorrhages are found less frequently. Immediate workup of symptoms in a high-risk patient plays a ■ CVA was appropriately investigated with a TTE and vascular imaging significant role in the morbidity and mortality of patients with IE. -

Endocarditis, Myocarditis and Pericarditis
ENDOCARDITIS, MYOCARDITIS AND PERICARDITIS ENDOCARDITIS Infective endocarditis is inflammatory disease of the endocardium, ussually affecting valves, if not treated is leading to death. -most frequent is bacterial, less frequent fungal ( viral ??? ) -mainly in older people, more men like women. Non-infective is not so frequent. Classification: 1. acute form 2. subacute form Acute IE – etiologically Staphyllococcus aureus, Streptococcus pyogenes, Neisseria etc. -affecting ussually healthy valves, causing metastatic lesions, proceed like sepsis. Subacute IE – much more frequent, ussually caused by streptococcal infection ( Str. viridans or epidermidis ) – affecting mainly valves damaged before infection. No metastatic deposits. Etiological classification: 1. IE of native valves 2. IE of drugs abusers 3. IE of prostethic valves Risk classification: 1. high risk – prosthetic valves, aortic stenosis and insuficiency, opened ductus arteriosus Bottali, A-V anastomoses, aortic coarctation, Marfan´s syndrome, previous IE 2. medium risk – mitral stenosis, tricuspidal stenosis and insuficiency, hypertrophic cardiomyopathy, calcified aortic stenosis, Fallot tetralogy, mitral prolapse, mitral insuficiency 3. low risk - degenerative heart diseases, atrial defect – type septum secundum, luetic aortitis, pacemakers, aorto-coronary bypasses Etiology and pathogenesis oropharyngeal infections, genitourinary, gastrointestinal or repiratory infections, history of instrumental procedures ( endoscopy of respiratory or gastrointestinal tract ), urological procedures, -

Infective Endocarditis Associated with Acute Myocardial Infarction Caused by Septic Emboli
Journal of Cardiology Cases (2010) 1, e28—e32 View metadata, citation and similar papers at core.ac.uk brought to you by CORE available at www.sciencedirect.com provided by Elsevier - Publisher Connector journal homepage: www.elsevier.com/locate/jccase Case Report Infective endocarditis associated with acute myocardial infarction caused by septic emboli Iwao Okai (MD) a, Kenji Inoue (MD, PhD) a,∗, Naotaka Yamaguchi (MD) b, Haruka Makinae (MD) c, Sonomi Maruyama (MD) a, Kaoru Komatsu (MD) d, Yasunobu Kawano (MD) e, Shinya Okazaki (MD) a, Yasumasa Fujiwara (MD) a, Masataka Sumiyoshi (MD) a, Atsushi Amano (MD, FJCC) c, Hiroyuki Daida (MD, FJCC) d a Department of Cardiology, Juntendo University Nerima Hospital, 3-1-10 Takanodai, Nerima-ku, Tokyo 177-8521, Japan b Department of Emergency and Intensive Care, Juntendo University Nerima Hospital, Tokyo, Japan c Department of Cardiovascular Surgery, Juntendo University School of Medicine, Tokyo, Japan d Department of Cardiology, Juntendo University School of Medicine, Tokyo, Japan e Department of Cardiology, Juntendo University Urayasu Hospital, Chiba, Japan Received 15 December 2008; received in revised form 30 May 2009; accepted 10 June 2009 KEYWORDS Abstract A 53-year-old Japanese man presented with severe chest pain. He had suffered Infective from persistent fever, muscle pain, arthralgia, and dyspnea on exertion (New York Heart endocarditis; Association class I) for two and half months prior to admission. He had been treated with Myocardial infarction; several antibiotics for two months and prednisolone for almost one month prior to admission. Septic emboli On the day of admission, he had suffered from chest pain at rest, and had come to our hospital. -

CARDIAC INFECTIONS Rheumatic Heart Disease and Infective Endocarditis
CARDIAC INFECTIONS Rheumatic Heart Disease and Infective Endocarditis Jonas D. Del Rosario, MD, FPPS, FPCC Clinical Associate Professor UP College of Medicine RHEUMATIC FEVER RHEUMATIC HEART DISEASE RF to RHD “Rheumatic Fever is a disease the LICKS the joints but BITES heart.” RHD IS THE MOST SERIOUS COMPLICATION OF RF Rheumatic Fever • Most common cause of acquired heart disease in children & young adults worldwide • Diffuse inflammation of connective tissues of heart, joints, brain, blood vessels & subcutaneous tissues • Rheumatic process causes fibrosis of heart valves leading to RHD Epidemiology • Incidence of RF and RHD has not decreased in developing countries • Rheumatic Fever is principally a disease of childhood, with a median age of 10 years, although is also occurs in adults • Remains a major cause of morbidity and mortality in country Acute Rheumatic Fever Age and Sex Distribution ( N = 117 ) Frequency 30 25 20 Male 15 Female 10 5 0 Age <2 2-3 4-5 6-7 8-9 10-11 12-13 14-15 >16 Years PGH – Pedia 1986-90 Rheumatic Fever & Rheumatic Heart Disease Prevalence in school children: Developing countries 18.6 / 1000 Philippines 1971-1980 0.9 / 1000 1981-1990 0.6 / 1000 Developed countries USA 1971-1980 0.7 / 1000 Australia 1981-1990 12.3 / 1000 Group A β-Hemolytic Streptococcus (GAS) • Capsule – Non-antigenic • Cell wall – M-protein – Induces antibodies – Serotypes 5, 6, & 19 cross react with myosin Streptococcal Tonsillopharyngitis Pathophysiology • Rheumatic fever develops in some children and adolescents following PHARYNGITIS with -

Infective Endocarditis: Determinants of Long Term Outcome R O M Netzer, S C Altwegg, E Zollinger, M Täuber, T Carrel, C Seiler
61 CARDIOVASCULAR MEDICINE Heart: first published as 10.1136/heart.88.1.61 on 1 July 2002. Downloaded from Infective endocarditis: determinants of long term outcome R O M Netzer, S C Altwegg, E Zollinger, M Täuber, T Carrel, C Seiler ............................................................................................................................. Heart 2002;88:61–66 Objective: To evaluate predictors of long term prognosis in infective endocarditis. Design: Retrospective cohort study. Setting: Tertiary care centre. Patients: 212 consecutive patients with infective endocarditis between 1980 and 1995 See end of article for Main outcome measures: Overall and cardiac mortality; event-free survival; and the following authors’ affiliations events: recurrence, need for late valve surgery, bleeding and embolic complications, cerebral dysfunc- ....................... tion, congestive heart failure. Correspondence to: Results: During a mean follow up period of 89 months (range 1–244 months), 56% of patients died. Professor Christian Seiler, In 180 hospital survivors, overall and cardiac mortality amounted to 45% and 24%, respectively. By Swiss Cardiovascular multivariate analysis, early surgical treatment, infection by streptococci, age < 55 years, absence of Centre Bern, University congestive heart failure, and > 6 symptoms or signs of endocarditis during active infection were pre- Hospital, Inselspital, Freiburgstrasse, CH-3010 dictive of improved overall long term survival. Independent determinants of event-free survival were Bern, Switzerland; infection by streptococci and age < 55 years. Event-free survival was 17% at the end of follow up both christian.seiler@ in medically–surgically treated patients and in medically treated patients. [email protected] Conclusions: Long term survival following infective endocarditis is 50% after 10 years and is Accepted 6 March 2002 predicted by early surgical treatment, age < 55 years, lack of congestive heart failure, and the initial ...................... -

Ischemic Stroke and ST-Elevation Myocardial Infarction Revealing Infective Endocarditis
European Review for Medical and Pharmacological Sciences 2017; 21: 4640-4641 Ischemic stroke and ST-elevation myocardial infarction revealing infective endocarditis G.-R. JOLIAT1,2, N. HALKIC1, O. PANTET2, N. BEN-HAMOUDA2 1Division of Visceral Surgery, Lausanne University Hospital (CHUV), Lausanne, Switzerland 2Adult Intensive Care Unit and Burn Center, Lausanne University Hospital (CHUV), Lausanne, Switzerland Abstract. – In this clinical scenario, we re- sedation stop. Cerebral CT showed an import- port the case of a patient who presented multi- ant ischemic stroke (Figure 1b). In reviewing ple embolic complications due to mitral infective the previous abdominal CT, splenic (Figure 2a) endocarditis (IE). A 68-year-old woman had ex- and renal infarcts (Figure 2b) were found. As tended right hepatectomy for hilar cholangiocar- cinoma. Unfortunately, she had multiple postop- endocarditis was suspected, a transesophageal erative complications and had to be transferred echocardiography was performed and revealed to the Intensive Care Unit. During this stay, we a 15-mm vegetation on the mitral valve. The pa- have diagnosed an Enterococcus faecium IE af- tient was given antibiotherapy but intensive care ter the occurrence of multiple embolic compli- was stopped considering poor neurological state cations (myocardial infarction, ischemic stroke, and bad oncologic prognosis. The patient died digital emboli, splenic emboli, and renal emboli). 10 days later. The autopsy examination identi- The case is presented hereunder with illustra- tive imagings. While embolism is a known com- fied Enterococcus faecium on the mitral valve, plication of IE, the presence of multiple emboli but surprisingly only calcifications were found in various organs is rare. macroscopically on the valve suggesting that the vegetation had completely dislodged.