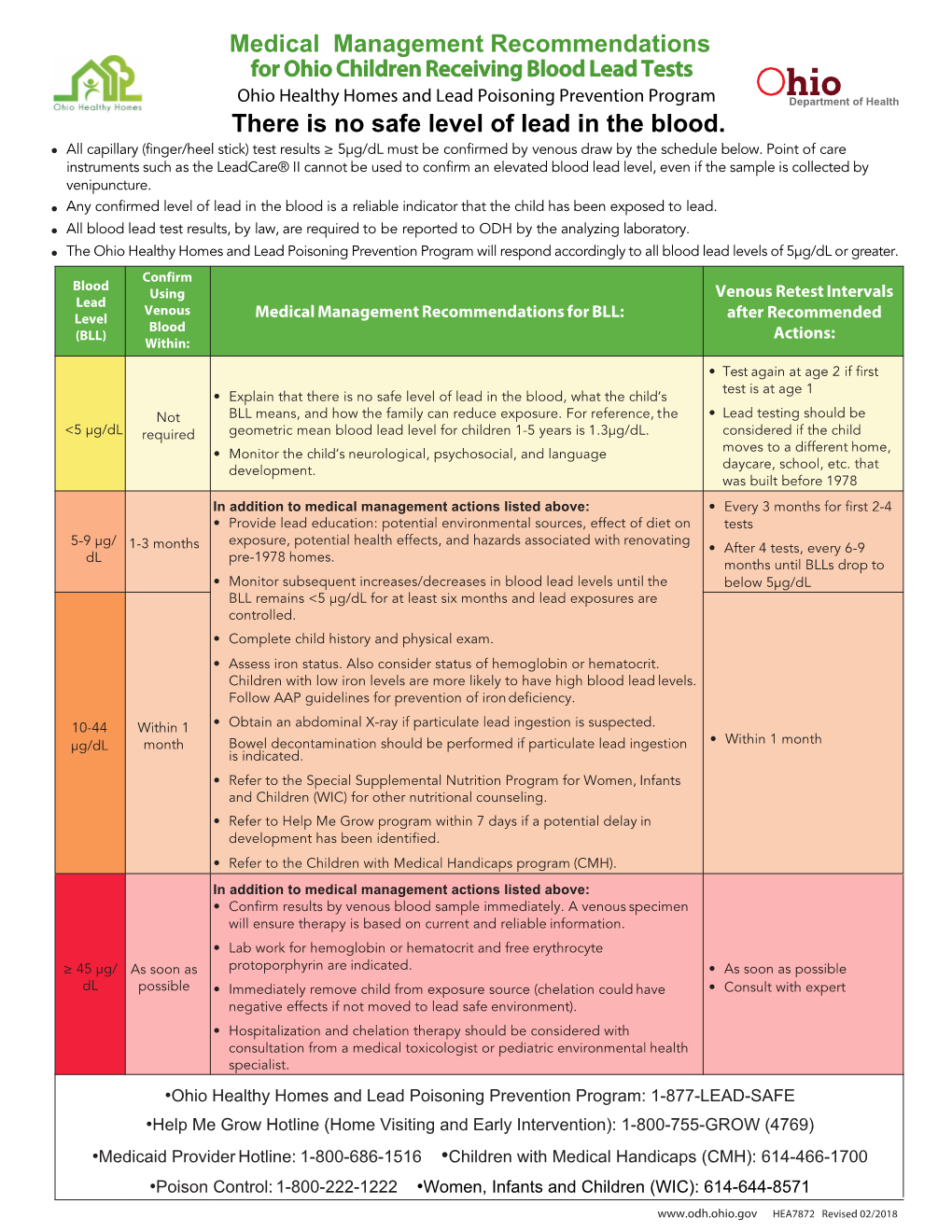
There Is No Safe Level of Lead in the Blood. • All Capillary (Finger/Heel Stick) Test Results ≥ 5Μg/Dl Must Be Confirmed by Venous Draw by the Schedule Below
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Blood Lead Test and Anticipatory Guidance
Guideline #6 BLOOD LEAD TEST AND ANTICIPATORY GUIDANCE RATIONALE No level of lead (Pb) in the body is recognized as safe. Lead toxicity is associated with impaired cognitive, motor, behavioral, and physical abilities. In 2012, the Centers for Disease Control and Prevention (CDC) recognized a risk of neurodevelopmental sequelae at blood lead levels (BLLs) below 5 micrograms of lead per deciliter of blood (mcg/dL) and replaced the former blood lead “level of concern” (10 mcg/dL) with a “reference level” of 5 mcg/dL.1 The Childhood Lead Poisoning Prevention Branch (CLPPB) of the California Department of Public Health (CDPH) is more protective in defining increased lead exposure. It interprets the reference level to include all BLLs equal to or greater than 4.5 mcg/dL.* Lead is a common environmental contaminant present in all areas of the United States, and all children are at risk for lead’s toxic effects. Within the United States approximately half a million children ages 1-5 years have blood lead levels greater than 5 mcg/dL.2 Lead exposure is one of the most common and preventable environmental diseases among California children. Many common items are associated with lead poisoning, either as the primary source or as part of the child’s cumulative exposure. Some of these have received a good deal of public attention. However, exposure to deteriorated lead-based paint and lead- contaminated dust and soil remain the major causes of childhood lead poisoning in California. Drinking water can contain lead, although it has not been found to be a major source of lead exposure in our state. -

Environmental Policy As Social Policy? the Impact of Childhood Lead Exposure on Crime
NBER WORKING PAPER SERIES ENVIRONMENTAL POLICY AS SOCIAL POLICY? THE IMPACT OF CHILDHOOD LEAD EXPOSURE ON CRIME Jessica Wolpaw Reyes Working Paper 13097 http://www.nber.org/papers/w13097 NATIONAL BUREAU OF ECONOMIC RESEARCH 1050 Massachusetts Avenue Cambridge, MA 02138 May 2007 I would especially like to thank Lawrence Katz for valuable advice, as well as David Cutler, Leemore Dafny, Amy Finkelstein, Claudia Goldin, Nora Gordon, Christopher Jencks, Walter Nicholson, Linda Reyes, René Reyes, Steven Rivkin, Geoffrey Woglom, Justin Wolfers, two anonymous referees, and many seminar participants. Numerous individuals at government agencies and petroleum industry companies generously provided data on lead in gasoline. Brent Mast, Bomy Hong, and John Indellicate II provided excellent research assistance. Any remaining errors are my own. This research was supported by grants from the National Science Foundation, the National Bureau of Economic Research, the National Institute on Aging, and the Harvard Multidisciplinary Program in Inequality and Social Policy. The views expressed herein are those of the author(s) and do not necessarily reflect the views of the National Bureau of Economic Research. © 2007 by Jessica Wolpaw Reyes. All rights reserved. Short sections of text, not to exceed two paragraphs, may be quoted without explicit permission provided that full credit, including © notice, is given to the source. Environmental Policy as Social Policy? The Impact of Childhood Lead Exposure on Crime Jessica Wolpaw Reyes NBER Working Paper No. 13097 May 2007 JEL No. I18,K49,Q53,Q58 ABSTRACT Childhood lead exposure can lead to psychological deficits that are strongly associated with aggressive and criminal behavior. In the late 1970s in the United States, lead was removed from gasoline under the Clean Air Act. -

Childhood Lead Exposures: Medical Management Recommendations For
Childhood Lead Exposure and Poisoning Medical Management Recommendations . There is no safe level of lead in the blood. The CDC reference for an elevated blood lead level (BLL) is 5 µg/dL. Exposure to lead can have a wide range of effects on a child’s development and behavior. Any BLL of 5 µg/dL or higher requires intervention to prevent further lead exposure and increase in blood lead levels. Any capillary blood lead level ≥5 µg/dL should be confirmed with a venous blood lead test. Recommended Schedule for Obtaining Confirmatory Venous Test After Capillary Test Capillary BLL Confirm Capillary Test with Venous Blood Test: 0 – <5 µg/dL No confirmation needed. Repeat test according to DHHS Blood Lead Screening Plan. 5 – 9 µg/dL Within 3 months* 10 – 44 µg/dL Within 1 month* 45 – 69 µg/dL Within 24 - 48 hours* ≥ 70 µg/dL Immediately as an emergency test* *The higher the BLL on a screening test, the more urgent the need for confirmatory testing. Medical Management Recommendations for Confirmed Blood Lead Levels Confirmed Follow-up Venous Recommended Actions Based on Confirmed Venous BLL BLL Test Schedule Review lab results with family. For reference, the geometric mean blood lead level for No follow-up needed. children 1-5 years old is less than 2 µg/dL. Continue to test Repeat blood lead level in 6-12 months if the child is at high risk or risk changes during < 5 µg/dL according to DHHS the timeframe. Blood Lead Screening Plan Provide anticipatory guidance and discuss common lead exposure sources. -

Lead in Drinking Water and Human Blood Lead Levels In the United States
Morbidity and Mortality Weekly Report Supplement / Vol. 61 August 10, 2012 Lead in Drinking Water and Human Blood Lead Levels in the United States U.S. Department of Health and Human Services Centers for Disease Control and Prevention Supplement CONTENTS Introduction ...........................................................................................................1 Background ............................................................................................................1 Historical Trends in Blood Lead Levels ..........................................................3 Lead in the Environments of Children ..........................................................4 Lead in Drinking Water .......................................................................................4 Conclusion ..............................................................................................................7 References ...............................................................................................................7 The MMWR series of publications is published by the Office of Surveillance, Epidemiology, and Laboratory Services, Centers for Disease Control and Prevention (CDC), U.S. Department of Health and Human Services, Atlanta, GA 30333. Suggested Citation: Centers for Disease Control and Prevention. [Title]. MMWR 2012;61(Suppl; August 10, 2012):[inclusive page numbers]. Centers for Disease Control and Prevention Thomas R. Frieden, MD, MPH, Director Harold W. Jaffe, MD, MA, Associate Director for Science James -

Recommended Chelation Protocol for Children with Blls ≥45 Μg/Dl
The New York City Department of Health and Mental Hygiene Guidelines for Health Care Providers Recommended Chelation Protocol for Children With BLLs ≥45 μg/dL Before Providing Chelation Therapy: • Confirm the blood lead level (BLL) ≥45 μg/dL with a venous specimen processed as an emergency test unless symptoms of encephalopathy are present. • Obtain an abdominal x-ray to look for lead solid ingestion; if radio-opaque particles are found or recent ingestion is witnessed, use a cathartic. • Arrange hospitalization and chelation therapy at a facility with expertise in treating lead-poisoned children. • Provide chelation therapy in, and discharge child to, a lead-safe environment. Do not discharge until the NYC Health Department inspects the home. • Inform the NYC Health Department of the hospital admission by calling 646-632-6002. The Health Department can provide referrals to providers with expertise in treating lead intoxication and referrals to temporary lead-safe housing. Chelation Therapy For Children with Venous BLLs ≥45 μg/dL1 BLL (μg/dL) Agent, Dosage,* and Administration Special Considerations Follow-up <45 Chelation therapy not routinely recommended See Reverse for Recommended Follow-up Blood Lead Test Schedule for Children 45 to <70 • DMSA (succimer, 2,3-meso-dimercaptosuccinic acid) • Monitor for anemia, • Schedule weekly health care visits • 1050 mg DMSA / m2 / 24 hours* ÷ q8 hours PO x neutropenia, and to monitor compliance and signs of toxicity. 5 days; round dose to nearest 100 mg/day, and then hepatic toxicity. • Monitor BLLs weekly until level stabilizes, ÷ 100-mg capsules as evenly as possible for q8-hour then follow Recommended Follow-up dosing schedule. -

Environmental Health Perspectives
ENVIRONMENTAL HEALTH ehp PERSPECTIVES ehponline.org A Geospatial Analysis of the Effects of Aviation Gasoline on Childhood Blood Lead Levels Marie Lynn Miranda, Rebecca Anthopolos, Douglas Hastings http://dx.doi.org/10.1289/ehp.1003231 Online 13 July 2011 National Institutes of Health U.S. Department of Health and Human Services Page 1 of 21 1 A Geospatial Analysis of the Effects of Aviation Gasoline on Childhood Blood Lead Levels Marie Lynn Miranda *, Rebecca Anthopolos, and Douglas Hastings Children’s Environmental Health Initiative, Nicholas School of the Environment, Duke University, Durham, NC 27708 *Corresponding author: Marie Lynn Miranda, Ph.D. Nicholas School of the Environment Duke University Box 90328 Levine Science Research Center Room A134 Durham, NC 27708-0328 919-613-8023 (o) 919-684-3227 (fax) [email protected] Page 2 of 21 2 Running Title: Aviation Gasoline and Childhood Blood Lead Levels Keywords: Aviation gasoline; Avgas; Blood lead; Childhood; Geospatial; Lead poisoning Acknowledgments: The authors gratefully acknowledge aviation gas data provided by Marion Hoyer from the EPA’s Office of Transportation and Air Quality and childhood lead exposure data provided by Ed Norman and Tena Ward from the NC Department of Environment and Natural Resources. We also acknowledge the geocoding work undertaken by the GIS staff of the Children’s Environmental Health Initiative. This work was funded in part by a grant from the USEPA (RD- 83329301) and the North Carolina Department of Environment and Natural Resources (1 H64 EH000151). Competing Financial Interest Declaration: The authors have no competing financial interests with regard to this manuscript. Abbreviations (as defined in the text): Avgas Aviation gasoline CDC Centers for Disease Control and Prevention CI Confidence interval EPA Environmental Protection Agency GIS Geographic Information Systems LL Low-lead NHANES National Health and Nutrition Examination Survey Page 3 of 21 3 Abstract Background: Aviation gasoline, commonly referred to as avgas, is a leaded fuel used in small aircraft. -

Ending Child Lead Exposure in Kent County
Kent County Land Bank Authority Review Subcommittee ENDING CHILD LEAD EXPOSURE IN KENT COUNTY Kent County Lead Task Force January 2018 May 11, 2017 The mission of Kent County government is to be an effective and efficient steward in delivering quality services for our diverse community. Our priority is to provide mandated services, which may be enhanced and supplemented by additional services to improve the quality of life for all our citizens within the constraints of sound fiscal policy. TABLE OF CONTENTS EXECUTIVE SUMMARY ..............................................................................3 KENT COUNTY LEAD TASK FORCE: PURPOSE AND PEOPLE .............7 GLOSSARY..................................................................................................9 Chapter 1: LEAD: SO USEFUL, SO DANGEROUS .................................10 Why people use lead and how lead can harm them More Kent County children are being poisoned by lead Chapter 2: SOURCES OF LEAD IN KENT COUNTY ...............................18 It’s not our municipal water system Lead dust in homes and soils Other lead contamination sources Young children are most at risk Chapter 3: CURRENT MODEL: TEST ONLY SOME CHILDREN ............27 Who gets tested and how Treatment and follow up for lead-poisoned children Secondary treatment vs. primary prevention Chapter 4: CURRENT MODEL: GET LEAD OUT OF POISONED CHILDREN’S HOMES ...............................................................................34 Levels of lead hazard control Who finances lead hazard control -

Effect of Chelation Therapy on the Neuropsychological and Behavioral Development of Lead-Exposed Children After School Entry
Effect of Chelation Therapy on the Neuropsychological and Behavioral Development of Lead-Exposed Children After School Entry Kim N. Dietrich, PhD*; James H. Ware, PhD‡; Mikhail Salganik, PhD‡; Jerilynn Radcliffe, PhD§; Walter J. Rogan, MD; George G. Rhoads, MD¶; Martha E. Fay, MPH‡; Cecilia T. Davoli, MD#; Martha B. Denckla, MD#; Robert L. Bornschein, PhD*; Donald Schwarz, MD**; Douglas W. Dockery, PhD‡; Susan Adubato, PhD‡‡; and Robert L. Jones, PhD§§, for the Treatment of Lead-Exposed Children Clinical Trial Group ABSTRACT. Objective. Some children in the United Results. Chelation therapy with succimer lowered av- States continue to be exposed to levels of lead that in- erage blood lead levels for ϳ6 months but resulted in no crease their risk for lowered intellectual functioning and benefit in cognitive, behavioral, and neuromotor end- behavior problems. It is unclear whether chelation ther- points. apy can prevent or reverse the neurodevelopmental se- Conclusion. These new follow-up data confirm our quelae of lead toxicity. The objective of this study was to previous finding that the TLC regimen of chelation ther- determine whether chelation therapy with succimer apy is not associated with neurodevelopmental benefits (dimercaptosuccinic acid) in children with referral blood in children with blood lead levels between 20 and 44 lead levels between 20 and 44 g/dL (0.96-2.12 mol/L) at g/dL (0.96–2.17 mol/L). These results emphasize the 12 to 33 months of age has neurodevelopmental benefits importance of taking environmental measures to prevent at age 7 years. exposure to lead. Chelation therapy with succimer cannot Methods. -

Lead Poisoning Prevention and Treatment Recommendations for Refugee Children
CDC Lead Poisoning Prevention and Treatment Recommendations for Refugee Children 1. Background: • Children who mouth or eat non-food items, especially soil, are at risk for lead poisoning, • Lead poisoning remains one of the most common regardless of the age of their housing. This and preventable pediatric environmental occurrence is common among certain refugee conditions in the United States. populations. • Lead is a poison that affects virtually every system in the human body. 3. Signs and Symptoms: • Lead poisoning, for the most part, is • Lead is particularly harmful to the developing brain asymptomatic. The vast majority of cases, and nervous system of fetuses and young children. therefore, go undiagnosed and untreated. • The prevalence of elevated blood lead levels • Very high lead levels in children can cause severe is much higher among newly resettled refugee neurologic problems such as coma, convulsion, children in the United States than the 1.6% and even death, although such levels are now rare prevalence for U.S. borne children. in the United States. 2. Exposure Routes: • Lower levels cause adverse effects on the central nervous system, kidney, and hematopoietic system. • The most common source of lead exposure for • Blood lead levels as low as 10µg/dL, which do children is deteriorated lead paint from older not cause distinctive symptoms, are associated housing. with decreased intelligence and impaired neurobehavioral development. • The primary route of exposure for children is by ingesting house dust or soil contaminated by • Many other effects begin at these low blood lead leaded paint. levels, including decreased stature or growth, decreased hearing acuity, and decreased ability • Young children have a higher risk for exposure to maintain a steady posture or growth. -

Flint Water Crisis
Case Examples FLINT WATER CRISIS Flint Water Crisis The Challenge The safety of our nation’s drinking water systems has recently been called into question. The water crisis that began in Flint, Michigan, in April 2014 sheds light on the interplay between weak governmental policy, the physical environmental health infrastructure, and the lack of oversight and accountability in a post-industrial region suffering from years of under-employment and industry divestment. Over the course of many months, a population of nearly 100,000 was stripped of one of the most basic human needs: clean drinking water. Flint’s aged water system—similar to that in many US urban areas—contains a large percentage of lead pipe sand plumbing.1 In April 2014, the city switched its water source from treated Lake Huron/Detroit River water to improperly treated Flint River water, which corroded pipes and caused lead to leach into the water. Lead can enter the body through drinking water, through foods cooked with contaminated water, or through infant formulas mixed with lead-tainted water. While lead occurs in the environment naturally, both EPA and CDC maintain no safe blood lead level in children.2, 3 In fact, lead exposure is linked to developmental and neurological damage in children,4 whose bodies absorb ingested lead at the alarming rate of 40 to 50 percent, compared with 3 to 10 percent in adults.1 Groups suffering disproportionate lead exposure include children, pregnant women, and low-income individuals.1 Most water system damage, as in Flint, is preventable with enforcement of proper regulatory safeguards. -

Association of Childhood Blood Lead Levels with Firearm Violence Perpetration and Victimization Lindsay Rae Emer University of Wisconsin-Milwaukee
University of Wisconsin Milwaukee UWM Digital Commons Theses and Dissertations December 2017 Association of Childhood Blood Lead Levels with Firearm Violence Perpetration and Victimization Lindsay Rae Emer University of Wisconsin-Milwaukee Follow this and additional works at: https://dc.uwm.edu/etd Part of the Environmental Health Commons, and the Public Health Commons Recommended Citation Emer, Lindsay Rae, "Association of Childhood Blood Lead Levels with Firearm Violence Perpetration and Victimization" (2017). Theses and Dissertations. 1610. https://dc.uwm.edu/etd/1610 This Dissertation is brought to you for free and open access by UWM Digital Commons. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of UWM Digital Commons. For more information, please contact [email protected]. ASSOCIATION OF CHILDHOOD BLOOD LEAD LEVELS WITH FIREARM VIOLENCE PERPETRATION AND VICTIMIZATION by Lindsay R. Emer A Dissertation Submitted in Partial Fulfillment of the Requirements for the Degree of Doctor of Philosophy in Public Health at The University of Wisconsin-Milwaukee December 2017 ABSTRACT ASSOCIATION OF CHILDHOOD BLOOD LEAD LEVELS WITH FIREARM VIOLENCE PERPETRATION AND VICTIMIZATION by Lindsay R. Emer The University of Wisconsin-Milwaukee, 2017 Under the Supervision of Professor Dr. Lance S. Weinhardt Over 10,000 Americans are killed in firearm homicides each year, and an additional 40,000 are injured in nonfatal shootings. There is a significant public health need to identify risk factors that can be modified to prevent firearm violence. Environmental lead exposure is a demonstrated neurotoxicant which causes behavior changes that are known to be criminogenic. More recent research has demonstrated that homicides and nonfatal shootings differ by the circumstances that lead to the shootings (i.e. -

The Worldwide Problem of Lead in Petrol Philip J
Editorials The worldwide problem of lead in petrol Philip J. Landrigan1 The use of lead as a petrol additive has mean blood lead level (6). Similar effects earlier this year, called specifically for the been a catastrophe for public health. were recorded in Western Europe, removal of lead from petrol. This call Leaded petrol has caused more exposure Australia, Canada, New Zealand and resonates with the theme of World Health to lead than any other source worldwide. South Africa (7). In a number of devel- Day 2003, which is healthy environments By contaminating air, dust, soil, drinking- oping countries too, including China, for children. water and food crops, it has caused El Salvador, India, Mexico and Thailand, Precaution is the lesson to be learnt harmfully high human blood lead levels declines in blood lead levels have followed from the history of lead in petrol. The around the world, especially in children (1). the removal of lead from petrol (8). worldwide dissemination of tetraethyl- Tetraethyllead was first added to Nearly 50 nations have now renounced lead is a classic example of our excessive petrol in 1922, to improve engine perfor- the use of lead in petrol, and more are willingness to adopt a promising but mance. Soon after production began in planning such action in the next five years. unproven new technology without heed Bayway, New Jersey, USA, an outbreak of Worldwide, unleaded petrol now to its possible consequences. We made acute neuropsychiatric disease appeared accounts for 80% of total sales (1). This is the same error with chlorofluorocarbon among workers, 80% of whom developed a triumph for public health.