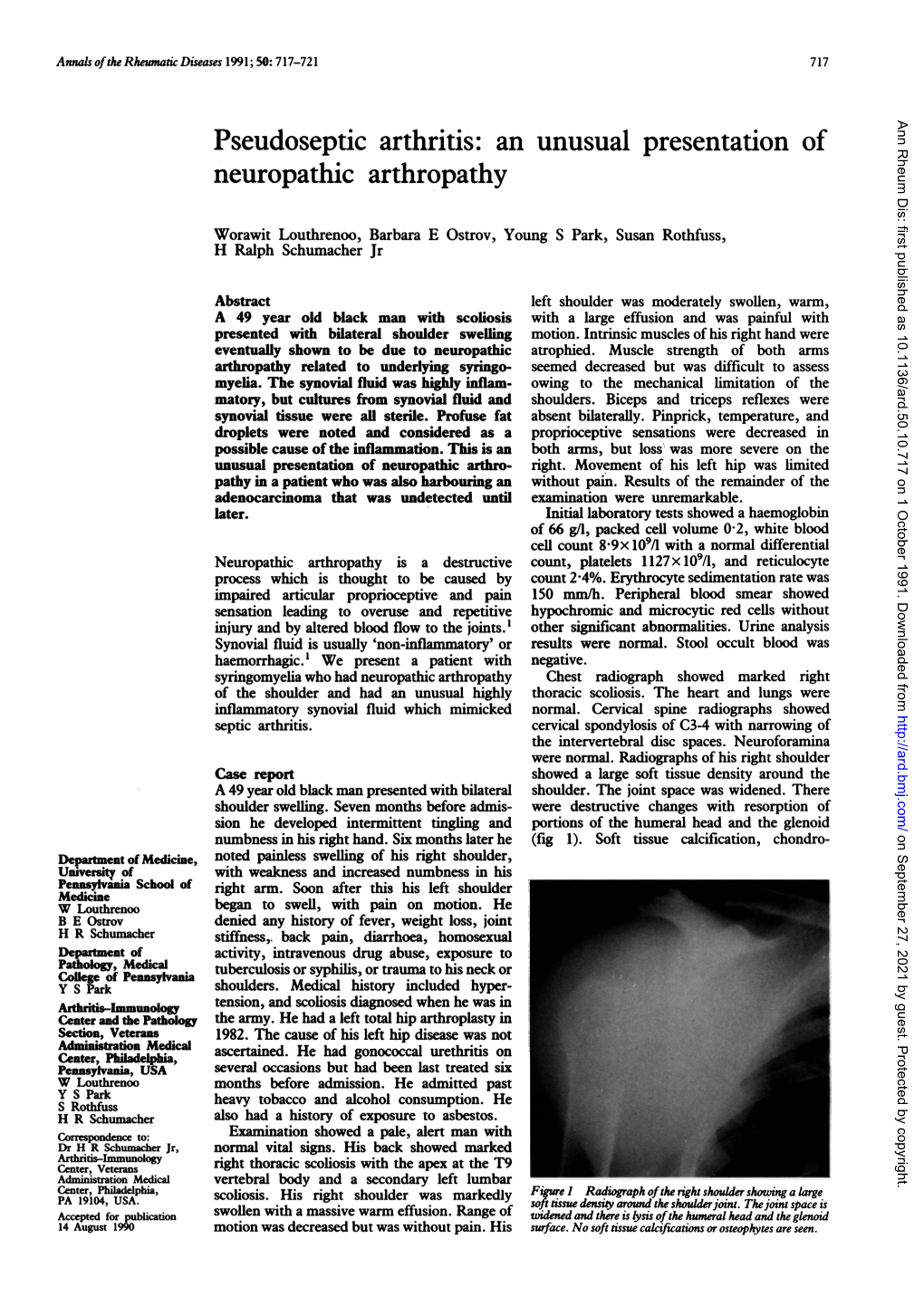
An Unusual Presentation of Neuropathic Arthropathy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Acute < 6 Weeks Subacute ~ 6 Weeks Chronic >
Pain Articular Non-articular Localized Generalized . Regional Pain Disorders . Myalgias without Weakness Soft Tissue Rheumatism (ex., fibromyalgia, polymyalgia (ex., soft tissue rheumatism rheumatica) tendonitis, tenosynovitis, bursitis, fasciitis) . Myalgia with Weakness (ex., Inflammatory muscle disease) Clinical Features of Arthritis Monoarthritis Oligoarthritis Polyarthritis (one joint) (two to five joints) (> five joints) Acute < 6 weeks Subacute ~ 6 weeks Chronic > 6 weeks Inflammatory Noninflammatory Differential Diagnosis of Arthritis Differential Diagnosis of Arthritis Acute Monarthritis Acute Polyarthritis Inflammatory Inflammatory . Infection . Viral - gonococcal (GC) - hepatitis - nonGC - parvovirus . Crystal deposition - HIV - gout . Rheumatic fever - calcium . GC - pyrophosphate dihydrate (CPPD) . CTD (connective tissue diseases) - hydroxylapatite (HA) - RA . Spondyloarthropathies - systemic lupus erythematosus (SLE) - reactive . Sarcoidosis - psoriatic . - inflammatory bowel disease (IBD) Spondyloarthropathies - reactive - Reiters . - psoriatic Early RA - IBD - Reiters Non-inflammatory . Subacute bacterial endocarditis (SBE) . Trauma . Hemophilia Non-inflammatory . Avascular Necrosis . Hypertrophic osteoarthropathy . Internal derangement Chronic Monarthritis Chronic Polyarthritis Inflammatory Inflammatory . Chronic Infection . Bony erosions - fungal, - RA/Juvenile rheumatoid arthritis (JRA ) - tuberculosis (TB) - Crystal deposition . Rheumatoid arthritis (RA) - Infection (15%) - Erosive OA (rare) Non-inflammatory - Spondyloarthropathies -

Variation in the Initial Treatment of Knee Monoarthritis in Juvenile Idiopathic Arthritis: a Survey of Pediatric Rheumatologists in the United States and Canada
Variation in the Initial Treatment of Knee Monoarthritis in Juvenile Idiopathic Arthritis: A Survey of Pediatric Rheumatologists in the United States and Canada TIMOTHY BEUKELMAN, JAMES P. GUEVARA, DANIEL A. ALBERT, DAVID D. SHERRY, and JON M. BURNHAM ABSTRACT. Objective. To characterize variations in initial treatment for knee monoarthritis in the oligoarthritis sub- type of juvenile idiopathic arthritis (OJIA) by pediatric rheumatologists and to identify patient, physi- cian, and practice-specific characteristics that are associated with treatment decisions. Methods. We mailed a 32-item questionnaire to pediatric rheumatologists in the United States and Canada (n = 201). This questionnaire contained clinical vignettes describing recent-onset chronic monoarthritis of the knee and assessed physicians’ treatment preferences, perceptions of the effective- ness and disadvantages of nonsteroidal antiinflammatory drugs (NSAID) and intraarticular corticos- teroid injections (IACI), proficiency with IACI, and demographic and office characteristics. Results. One hundred twenty-nine (64%) questionnaires were completed and returned. Eighty-three per- cent of respondents were board certified pediatric rheumatologists. Respondents’ treatment strategies for uncomplicated knee monoarthritis were broadly categorized: initial IACI at presentation (27%), initial NSAID with contingent IACI (63%), and initial NSAID with contingent methotrexate or sulfasalazine (without IACI) (10%). Significant independent predictors for initial IACI were believing that IACI is more effective than NSAID, having performed > 10 IACI in a single patient at one time, and initiating methotrexate via the subcutaneous route for OJIA. Predictors for not recommending initial or contin- gent IACI were believing that the infection risk of IACI is significant and lacking comfort with per- forming IACI. Conclusion. There is considerable variation in pediatric rheumatologists’ initial treatment strategies for knee monoarthritis in OJIA. -

Concurrent Onset of Adult Onset Still's Disease and Insulin Dependent Diabetes Mellitus
Annals ofthe Rheumatic Diseases 1990; 49: 547-548 547 Concurrent onset of adult onset Still's disease and Ann Rheum Dis: first published as 10.1136/ard.49.7.547 on 1 July 1990. Downloaded from insulin dependent diabetes mellitus J T Sibley Abstract time, partial thromboplastin time, C3, C4, Clq Within two weeks after symptoms of an upper binding, tri-iodothyronine, thyroxine, serum respiratory tract infection a 32 year old man amylase, serum protein electrophoresis, and developed Still's disease and insulin dependent gallium scan. diabetes mellitus, both ofwhich have persisted Initial and convalescent serum rubella titres for 24 months. Investigations failed to confirm (haemagglutination inhibition) were both 1/640. acute infection but did show isolated persistent Hepatic transaminases were five times normal. increase of serum antibodies to rubelia virus. Abdominal ultrasound confirmed splenomegaly The simultaneous onset of these two diseases and showed decreased echogenicity of the suggests a shared cause, possibly associated pancreas. An abdominal computed tomography with rubella infection. scan was normal except for hepatosplenomegaly. Percutaneous liver biopsy showed only minor focal portal tract inflammation. A two dimen- Adult onset Still's disease is an uncommon sional echocardiogram showed a small peri- entity characterised by a multisystem illness cardial effusion. HLA typing results were with a wide constellation of features, notably A2,-;B44,5 1 ;Cw2,-;DR1,7. fever, rash, and arthritis.' Its cause is unknown, The diagnosis of adult onset Still's disease though there are a few reports of association was based on the typical clinical features, with viral illness.2A Insulin dependent diabetes including the characteristic evanescent rash and mellitus is also thought in some cases to have a daily fever in the absence ofclinical or laboratory viral cause,5 but I am unaware of any reports of confirmation of other diagnostic possibilities.' 6 the simultaneous onset of these two diseases. -

Biological Treatment in Resistant Adult-Onset Still's Disease: a Single-Center, Retrospective Cohort Study
Arch Rheumatol 2021;36(x):i-viii doi: 10.46497/ArchRheumatol.2021.8669 ORIGINAL ARTICLE Biological treatment in resistant adult-onset Still’s disease: A single-center, retrospective cohort study Seda Çolak, Emre Tekgöz, Maghrur Mammadov, Muhammet Çınar, Sedat Yılmaz Department of Internal Medicine, Division of Rheumatology, Gülhane Training and Research Hospital, Ankara, Turkey ABSTRACT Objectives: The aim of this study was to assess the demographic and clinical characteristics of patients with adult-onset Still’s disease (AOSD) under biological treatment. Patients and methods: This retrospective cohort study included a total of 19 AOSD patients (13 males, 6 females; median age: 37 years; range, 28 to 52 years) who received biological drugs due to refractory disease between January 2008 and January 2020. The data of the patients were obtained from the patient files. The response to the treatment was evaluated based on clinical and laboratory assessments at third and sixth follow-up visits. Results: Interleukin (IL)-1 inhibitor was prescribed for 13 (68.4%) patients and IL-6 inhibitor prescribed for six (31.6%) patients. Seventeen (89.5%) patients experienced clinical remission. Conclusion: Biological drugs seem to be effective for AOSD patients who are resistant to conventional therapies. Due to the administration methods and the high costs of these drugs, however, tapering the treatment should be considered, after remission is achieved. Keywords: Adult-onset Still’s disease, anakinra, tocilizumab, treatment. Adult-onset Still’s disease (AOSD) is a rare diseases that may lead to similar clinical and systemic inflammatory disease with an unknown laboratory findings. etiology. The main clinical manifestations of It is well known that proinflammatory the disease are fever, maculopapular salmon- pink rash, arthralgia, and arthritis. -

Gout and Monoarthritis
Gout and Monoarthritis Acute monoarthritis has numerous causes, but most commonly is related to crystals (gout and pseudogout), trauma and infection. Early diagnosis is critical in order to identify and treat septic arthritis, which can lead to rapid joint destruction. Joint aspiration is the gold standard method of diagnosis. For many reasons, managing gout, both acutely and as a chronic disease, is challenging. Registrars need to develop a systematic approach to assessing monoarthritis, and be familiar with the management of gout and other crystal arthropathies. TEACHING AND • Aetiology of acute monoarthritis LEARNING AREAS • Risk factors for gout and septic arthritis • Clinical features and stages of gout • Investigation of monoarthritis (bloods, imaging, synovial fluid analysis) • Joint aspiration techniques • Interpretation of synovial fluid analysis • Management of hyperuricaemia and gout (acute and chronic), including indications and targets for urate-lowering therapy • Adverse effects of medications for gout, including Steven-Johnson syndrome • Indications and pathway for referral PRE- SESSION • Read the AAFP article - Diagnosing Acute Monoarthritis in Adults: A Practical Approach for the Family ACTIVITIES Physician TEACHING TIPS • Monoarthritis may be the first symptom of an inflammatory polyarthritis AND TRAPS • Consider gonococcal infection in younger patients with monoarthritis • Fever may be absent in patients with septic arthritis, and present in gout • Fleeting monoarthritis suggests gonococcal arthritis or rheumatic fever -

Differential Diagnosis of Juvenile Idiopathic Arthritis
pISSN: 2093-940X, eISSN: 2233-4718 Journal of Rheumatic Diseases Vol. 24, No. 3, June, 2017 https://doi.org/10.4078/jrd.2017.24.3.131 Review Article Differential Diagnosis of Juvenile Idiopathic Arthritis Young Dae Kim1, Alan V Job2, Woojin Cho2,3 1Department of Pediatrics, Inje University Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea, 2Department of Orthopaedic Surgery, Albert Einstein College of Medicine, 3Department of Orthopaedic Surgery, Montefiore Medical Center, New York, USA Juvenile idiopathic arthritis (JIA) is a broad spectrum of disease defined by the presence of arthritis of unknown etiology, lasting more than six weeks duration, and occurring in children less than 16 years of age. JIA encompasses several disease categories, each with distinct clinical manifestations, laboratory findings, genetic backgrounds, and pathogenesis. JIA is classified into sev- en subtypes by the International League of Associations for Rheumatology: systemic, oligoarticular, polyarticular with and with- out rheumatoid factor, enthesitis-related arthritis, psoriatic arthritis, and undifferentiated arthritis. Diagnosis of the precise sub- type is an important requirement for management and research. JIA is a common chronic rheumatic disease in children and is an important cause of acute and chronic disability. Arthritis or arthritis-like symptoms may be present in many other conditions. Therefore, it is important to consider differential diagnoses for JIA that include infections, other connective tissue diseases, and malignancies. Leukemia and septic arthritis are the most important diseases that can be mistaken for JIA. The aim of this review is to provide a summary of the subtypes and differential diagnoses of JIA. (J Rheum Dis 2017;24:131-137) Key Words. -

Acute Monoarthritis (Adult) on AMU
Acute Monoarthritis (Adult) on AMU Document Examinations Findings Consider Potential Causes Articular Features (pain, tenderness Septic Arthritis Swelling, redness, warmth) Gout Other joint involvement Pyrophosphate Crystal Deposition Extra-articular features (pseudogout) Tophi Reactive Arthritis SEW Score Monoarticular Onset Polyarthritis Precipitating factors (e.g trauma) Traumatic Synovitis& Mechanical Evidence of other disease (incl. post fracture) Haemarthrosis Inflammatory OA Investigations Aspiration from an area of clear skin must be performed as part of initial investigations (must be done by/under supervision of experienced clinician) DO NOT ASPIRATE PROSTHETIC JOINTS WITHOUT ORTHOPAEDIC SUPPORT: • microbiology sample in a universal container (cell count & crystals) • blood culture bottles • If gonococcus suspectd request PCR • Phone the microbiology MLSO to inform of sample for crystals Peripheral Blood Cultures (x 2 if clinical sepsis and/or pyrexia) Full blood count & biochemistry PV & CRP X-ray joint INR if on warfarin Any other investigations suggested by history/examination to determine cause D/W Rheumatology on call when possible Suspicion of Septic Reactive Arthritis Gout Pyrophosphate or Arthritis pseudogout Uncomplicated Full dose NSAID 1. Full dose NSAID with As per gout (likely gram + ve) with gastric gastric protection or * Flucloxacillin IV 2g protection Bed-rest & local QID 2. Colchicine steroid injection * Clindamycin 600mg Treat precipitating 500micrgrams 2-3 QID if penicillin-allergic factor (e.g. times daily -

Rheumatology Emergencies
EMERGENCIES IN RHEUMATOLOGY RICHARD LAI, MD, FACP, FACR BENEFIS HOSPITAL SECTION OF RHEUMATOLOGY Difficulty Breathing DIFFICULTY BREATHING – CASE 1 A 45-year-old woman presents to the emergency room with glottic and subglottic inflammation and edema, requiring an urgent tracheostomy. She’s treated with antibiotics, but cultures of the pharynx and larynx are thus far negative. Three days earlier, she developed pain and swelling of her nose. During the past year, she has had episodes of ear swelling and recurrent pain and swelling in the knees. On physical examination, a tracheostomy is in place, and she is afebrile. The joints show no swelling or limitation. There is swelling, redness, and warmth over the distal half of the nose. The remainder of the examination is normal. Laboratory studies Leukocyte count - 11,000/µL Serum creatinine - 0.6 mg/dL P-ANCA - 1:160 (positive) C-ANCA – Normal Urinalysis – Normal Chest radiograph – Normal WHAT IS THE MOST LIKELY DIAGNOSIS? A. Granulomatosis with polyangiitis B. Systemic lupus erythematosus C. Rheumatoid arthritis D. Relapsing polychondritis E. Polyarteritis nodosa WHAT IS THE MOST LIKELY DIAGNOSIS? A. Granulomatosis with polyangiitis B. Systemic lupus erythematosus C. Rheumatoid arthritis D. Relapsing polychondritis E. Polyarteritis nodosa RELAPSING POLYCHONDRITIS EPISODIC INFLAMMATION OF HYALINE CARTILAGE Ears and/or nose common Larynx and tracheal cartilage - life-threatening Non-erosive arthritis Eyes (scleritis) Aortic regurgitation Panniculitis of skin Which of the conditions below is LEAST likely to cause stridor? A. Rheumatoid arthritis B. Complement mediated angioedema C. Granulomatosis with polyangiitis D. Inflammatory myopathy E. Ankylosing spondylitis Which of the conditions below is LEAST likely to cause stridor? A. -
Atypical Monoarthritis Presentation in Children with Oligoarticular Juvenile
Lepore et al. Pediatric Rheumatology (2017) 15:2 DOI 10.1186/s12969-016-0129-x SHORTREPORT Open Access Atypical monoarthritis presentation in children with oligoarticular juvenile idiopathic arthritis: a case series Natasha Lepore1,2,3,4, Megan Cashin2,5, Debra Bartley2,5 and Daniela Simona Ardelean1,2,4,6* Abstract Background: Oligoarticular juvenile idiopathic arthritis (oligoJIA), the most common chronic inflammatory arthritis of childhood, usually involves the knees and ankles. Severe oligoJIA monoarthritis presenting in a joint other than knees and ankles, is rare. Findings: We report four children who presented with severe isolated arthritis of the hip, wrist or elbow and were diagnosed with oligoJIA. All four were girls with a median age of 11.5 years. Those with hip arthritis also met the classification criteria for juvenile-onset spondylarthopathy. Median duration of symptoms prior to diagnosis was 9.5 months. Three children had already cartilage loss or erosive disease at diagnosis. Conclusions: Children diagnosed with oligoJIA that present with monoarthritis of the hip, wrist and elbow can have aggressive disease. Girls with positive HLA-B27 presenting with isolated hip arthritis could meet the classification criteria for both oligoJIA and juvenile-onset SpA. Early referral to specialized care may improve their diagnosis, treatment and outcome. Keywords: Children,Atypicalmonoarthritis,oligoJIA,Presentation,Hip,Elbow,Wrist Introduction Hence, early recognition is paramount in avoiding irre- Juvenile idiopathic arthritis (JIA) is a heterogeneous versible joint and bone damage. In this study, we describe group of seven immune-mediated chronic inflammatory four children with oligoJIA who presented at our center diseases that target the joints in children younger than with severe, erosive monoarthritis. -

Non-Inflammatory Arthritis Non-Inflammatory Arthritis
The webinar will start promptly at the scheduled time All attendees are muted throughout the webinar The moderator will review your questions and present them to the Welcome to lecturer at the end of the presentation At the bottom of your screen are three options for the ViP Adult comments/questions: Chat is to used to make general comments that everyone can see Webinar Raise Your Hand is to be used to notify the Host that you need attention. The Host will send you a private chat in response. Q&A is used to post questions relevant to the lecture. These questions can only be seen by the lecturer and moderator. Approach to the Patient with “Arthritis” Jason Kolfenbach, MD University of Colorado Disclosures I have no disclosures related to the content of this talk. FOCUS ON: Non-inflammatory arthritis Non-inflammatory Arthritis • History • no “believable” red/hot joints • slow steady progression • mechanical pain: use, rest/night • no profound/prolonged morning stiffness • no systemic findings • Physical exam • swelling: • effusion/osteophytes/ligaments • crepitus/grating • local joint line tenderness Acute Non-inflammatory Monoarthritis Trauma Internal derangement (meniscal tear) Osteoarthritis Hemophilia Avascular necrosis Sickle cell disease Transient osteoporosis of the hip Chronic Non-inflammatory Monoarthritis Osteoarthritis Internal derangement Tumors: PVNS (chocolate SF), synovial sarcoma Charcot: Diabetes, syphilis, syringomyelia Others: Avascular necrosis, hemarthrosis (bleeding disorder; coumadin use), synovial chondromatosis -

Acute Monoarthritis in Young Children: Comparing the Characteristics of Patients with Juvenile Idiopathic Arthritis Versus Septi
www.nature.com/scientificreports OPEN Acute monoarthritis in young children: comparing the characteristics of patients with juvenile idiopathic arthritis versus septic and undiferentiated arthritis Marion Thomas1,2,3,4, Stephane Bonacorsi5,6, Anne‑Laure Simon5,7, Cindy Mallet5,7, Mathie Lorrot8, Albert Faye1,5, Glory Dingulu1, Marion Caseris1, Ivo Gomperts Boneca2,3,4, Camille Aupiais9,10,12 & Ulrich Meinzer1,2,3,4,5,11,12* Acute arthritis is a common cause of consultation in pediatric emergency wards. Arthritis can be caused by juvenile idiopathic arthritis (JIA), septic (SA) or remain undetermined (UA). In young children, SA is mainly caused by Kingella kingae (KK), a hard to grow bacteria leading generally to a mild clinical and biological form of SA. An early accurate diagnosis between KK‑SA and early‑onset JIA is essential to provide appropriate treatment and follow‑up. The aim of this work was to compare clinical and biological characteristics, length of hospital stays, duration of intravenous (IV) antibiotics exposure and use of invasive surgical management of patients under 6 years of age hospitalized for acute monoarthritis with a fnal diagnosis of JIA, SA or UA. We retrospectively analyzed data from < 6‑year‑old children, hospitalized at a French tertiary center for acute mono‑arthritis, who underwent a joint aspiration. Non‑parametric tests were performed to compare children with JIA, SA or UA. Bonferroni correction for multiple comparisons was applied with threshold for signifcance at 0.025. Among the 196 included patients, 110 (56.1%) had SA, 20 (10.2%) had JIA and 66 (33.7%) had UA. Patients with JIA were older when compared to SA (2.7 years [1.8–3.6] versus 1.4 [1.1–2.1], p < 0.001). -

Alteration of Descending Modulation of Nociception During the Course of Monoarthritis in the Rat
The Journal of Neuroscience, March 15, 1999, 19(6):2394–2400 Alteration of Descending Modulation of Nociception during the Course of Monoarthritis in the Rat Nicolas Danziger, Jeanne Weil-Fugazza, Daniel Le Bars, and Didier Bouhassira Institut National de la Sante´ et de la Recherche Me´ dicale U-161, 75014 Paris, France Diffuse noxious inhibitory controls (DNIC), which involve su- However, they showed different electrophysiological profiles. In praspinal structures and modulate the transmission of nocicep- the animals with acute monoarthritis, the DNIC-induced inhibi- tive signals, were investigated at different stages during the tions produced by mechanical or thermal stimulation of the development of adjuvant-induced monoarthritis in the rat. After arthritic joint were significantly increased at all intensities com- behavioral evaluation, recordings of trigeminal convergent neu- pared with the normal joint. In contrast, in the chronic stage of rons were performed in anesthetized animals with acute (24–48 monoarthritis, the DNIC-induced inhibitions triggered by ther- hr) or chronic (3–4 weeks) monoarthritis of the ankle. Inhibitions mal or pressure stimuli were similar for both ankles, except with of C-fiber-evoked neuronal responses during and after the the most intense mechanical stimuli. This discrepancy between application of noxious conditioning stimuli to the ankle were the behavioral and electrophysiological findings suggests that measured to evaluate DNIC. The conditioning stimuli consisted inputs activated during chronic monoarthritis may fail to recruit of mechanical (maximal flexion and graded pressures) and DNIC and may thus be functionally different from those acti- graded thermal stimuli and were applied alternately to normal vated in the acute stage of inflammation.