Science in Autism Treatment
Total Page:16
File Type:pdf, Size:1020Kb

Load more
Recommended publications
-

House Bill 1306 Industry, Business and Labor January 19, 2021, 2:45
House Bill 1306 Industry, Business and Labor January 19, 2021, 2:45 p.m. Good Morning Chairman Weisz and members of the House Human Services Committee. My name is Molly Howell and I am the Immunization Director of for the North Dakota Department of Health. I do not have testimony for HB1306 but want to let you know I am available virtually to answer questions, if needed. Additionally, attached is a list of studies that have been previously published regarding vaccines, autism and SIDS. Thank You. 1 Vaccine-Related Science: Autism and SIDS No Causal Association Found Autism Literature Reviews: Autism and Vaccines 1. Measles, Mumps, Rubella Vaccination and Autism: A Nationwide Cohort Study PDF available here Annals of Internal Medicine March 2019 The study strongly supports that MMR vaccination does not increase the risk for autism, does not trigger autism in susceptible children, and is not associated with clustering of autism cases after vaccination. It adds to previous studies through significant additional statistical power and by addressing hypotheses of susceptible subgroups and clustering of cases. 2. Autism Occurrence by MMR Vaccine Status Among US Children With Older Siblings With and Without Autism http://jama.jamanetwork.com/article.aspx?articleid=2275444 The Journal of the American Medical Association April 2015 In this large sample of privately insured children with older siblings, receipt of the MMR vaccine was not associated with increased risk of ASD, regardless of whether older siblings had ASD. These findings indicate no harmful association between MMR vaccine receipt and ASD even among children already at higher risk for ASD. -

Collaborative and Inclusive Process with the Autism Community: a Case Study in Colombia About Social Robot Design
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Ghent University Academic Bibliography International Journal of Social Robotics https://doi.org/10.1007/s12369-020-00627-y Collaborative and Inclusive Process with the Autism Community: A Case Study in Colombia About Social Robot Design Andrés A. Ramírez-Duque1,6 · Luis F. Aycardi2 · Adriana Villa3 · Marcela Munera2 · Teodiano Bastos1 · Tony Belpaeme4,5 · Anselmo Frizera-Neto1 · Carlos A. Cifuentes2 Accepted: 18 January 2020 © Springer Nature B.V. 2020 Abstract One of the most promising areas in which social assistive robotics has been introduced is therapeutic intervention for children with autism spectrum disorders (CwASD). Even though there are promising results in therapeutic contexts, there is a lack of guidelines on how to select the appropriate robot and how to design and implement the child–robot interaction. The use of participatory design (PD) methods in the design of technology-based processes for CwASD is a recognition of the stakeholders as “experts” in their fields. This work explores the benefits brought by the use of PD methods in the design of a social robot, with a specific focus on their use in autism spectrum disorders therapies on the Colombian autism community. Based on what proved to be effective in our previous research, we implemented participatory methods for both the CwASD and the stakeholders. The process leverages the active role of participants using a focus group approach with parents and specialists, and scene cards, narrative and handmade generative methods with the children. To overcome some challenges of traditional PD processes, where not all community actors are considered, we included a Colombian community consisting of therapists, nurses, caregivers and parents. -

The Joy of Autism: Part 2
However, even autistic individuals who are profoundly disabled eventually gain the ability to communicate effectively, and to learn, and to reason about their behaviour and about effective ways to exercise control over their environment, their unique individual aspects of autism that go beyond the physiology of autism and the source of the profound intrinsic disabilities will come to light. These aspects of autism involve how they think, how they feel, how they express their sensory preferences and aesthetic sensibilities, and how they experience the world around them. Those aspects of individuality must be accorded the same degree of respect and the same validity of meaning as they would be in a non autistic individual rather than be written off, as they all too often are, as the meaningless products of a monolithically bad affliction." Based on these extremes -- the disabling factors and atypical individuality, Phil says, they are more so disabling because society devalues the atypical aspects and fails to accommodate the disabling ones. That my friends, is what we are working towards -- a place where the group we seek to "help," we listen to. We do not get offended when we are corrected by the group. We are the parents. We have a duty to listen because one day, our children may be the same people correcting others tomorrow. In closing, about assumptions, I post the article written by Ann MacDonald a few days ago in the Seattle Post Intelligencer: By ANNE MCDONALD GUEST COLUMNIST Three years ago, a 6-year-old Seattle girl called Ashley, who had severe disabilities, was, at her parents' request, given a medical treatment called "growth attenuation" to prevent her growing. -
Model Reveals New Links Between Autism and Fragile X
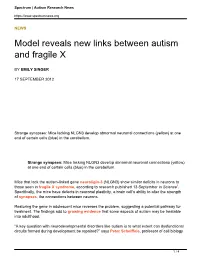
Spectrum | Autism Research News https://www.spectrumnews.org NEWS Model reveals new links between autism and fragile X BY EMILY SINGER 17 SEPTEMBER 2012 Strange synapses: Mice lacking NLGN3 develop abnormal neuronal connections (yellow) at one end of certain cells (blue) in the cerebellum. Strange synapses: Mice lacking NLGN3 develop abnormal neuronal connections (yellow) at one end of certain cells (blue) in the cerebellum. Mice that lack the autism-linked gene neuroligin-3 (NLGN3) show similar deficits in neurons to those seen in fragile X syndrome, according to research published 13 September in Science1. Specifically, the mice have defects in neuronal plasticity, a brain cell’s ability to alter the strength of synapses, the connections between neurons. Restoring the gene in adolescent mice reverses the problem, suggesting a potential pathway for treatment. The findings add to growing evidence that some aspects of autism may be treatable into adulthood. “A key question with neurodevelopmental disorders like autism is to what extent can dysfunctional circuits formed during development be repaired?” says Peter Scheiffele, professor of cell biology 1 / 4 Spectrum | Autism Research News https://www.spectrumnews.org and biological development at the University of Basel in Switzerland, and the study’s lead investigator. “We see that a substantial amount of inappropriate synapses can be rescued in the adult.” The research also supports the idea that studying so-called syndromic forms of autism, such as fragile X, which are further along in drug development than are more common forms of autism, will shed light on the molecular underpinnings of the disorder. “I was quite excited about this paper because it links what may be very different genetic causes of autism to perhaps similar mechanistic and therapeutic targets,” says Kimberly Huber, associate professor of neuroscience at the University of Texas Southwestern Medical Center in Dallas. -

100 Day Kit for Newly Diagnosed Families of School Age Children
100 Day Kit for Newly Diagnosed Families of School Age Children FAMILY SERVICES DECEMBER 2014 100 DAY KIT FOR SCHOOL AGE CHILDREN The Autism Speaks 100 Day Kit is a tool designed to help assist families of children recently diagnosed with autism during the critical period following an autism diagnosis. The 100 Day Kit for School Age Children was released in 2014 and adapted from the 2010 Asperger Syndrome/High-Functioning Autism Tool Kit after the DSM-5 was published. The kits were created by the Autism Speaks Family Services staff in conjunction with both an advisory committee and the Family Services Committee. Autism Speaks would like to extend special thanks to the Advisory Committee for the time and effort that they put into reviewing this kit: 100 Day Kit for School Age Children Mel Karmazin* Advisory Committee Grandparent Ann Brendel Brian Kelly * ** Parent Geraldine Dawson, Ph.D. Professor, Department of Psychiatry and Artie Kempner* Behavioral Sciences Parent Duke University Medical Center Gary S. Mayerson* Lauren Elder, Ph.D. Founding Attorney, Mayerson & Associates Director, Ascent Psychological Services Kevin Murray* Peter F. Gerhardt, Ed.D. Parent Former President, Organization for Autism Research (OAR) Linda Meyer, Ed.D. Kerry Magro, M.A. Executive Director, Autism New Jersey Autism Speaks Social Media Coordinator, Danny Openden, Ph.D., B.C.B.A.-D. Self-advocate President and CEO, Southwest Autism Research and Valerie Paradiz, Ph.D. Resource Center (SARRC) Director, Valerie Paradiz, LLC Valerie Paradiz, Ph.D. Director Autistic Global Initiative Director, Valerie Paradiz, LLC Parent and self-advocate Director Autistic Global Initiative Patricia R. -

Autism Spectrum Conditions Affect Preferences in Valued Personal Possessions
This is a repository copy of Autism spectrum conditions affect preferences in valued personal possessions. White Rose Research Online URL for this paper: https://eprints.whiterose.ac.uk/130206/ Version: Accepted Version Article: Spikins, Penny orcid.org/0000-0002-9174-5168, Wright, Barry John Debenham orcid.org/0000-0002-8692-6001 and Scott, Callum (2018) Autism spectrum conditions affect preferences in valued personal possessions. Evolutionary Behavioral Sciences. pp. 99-112. ISSN 2330-2925 https://doi.org/10.1037/ebs0000105 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ Running head: AUTISM AND VALUED PERSONAL POSSESSIONS Autism spectrum conditions affect preferences in valued personal possessions Penny Spikins, Barry Wright and Callum Scott University of York Author Note Penny Spikins, Department of Archaeology, University of York, UK, Barry Wright, Department of Health Sciences, University of York, UK Callum Scott, Department of Archaeology, University of York, UK This research was supported in part by grants from the Creativity Priming Fund, University of York and the Sir John Templeton Foundation, and the survey was carried out with assistance from the National Autistic Society, UK. -

Campbell-Smith Mead Autism Decision.Pdf
In the United States Court of Federal Claims OFFICE OF SPECIAL MASTERS (E-Filed: March 12, 2010) No. 03-215V TO BE PUBLISHED ____________________________________ GEORGE and VICTORIA ) MEAD, Parents of ) Omnibus Autism Proceeding; WILLIAM P. MEAD, ) Test Case; Petitioners’ Second ) Theory of General Causation; Petitioners, ) Failure to Prove that ) Thimerosal-Containing v. ) Vaccines Cause Autism ) SECRETARY OF HEALTH AND ) HUMAN SERVICES, ) ) Respondent. ) ____________________________________) Thomas Powers, Portland, OR, for petitioners. Lynn Ricciardella, United States Department of Justice, Washington, DC, for respondent. DECISION1 1 Vaccine Rule 18(b) provides that all of the decisions of the special masters will be made available to the public unless an issued decision contains trade secrets or commercial or financial information that is privileged or confidential, or the decision contains medical or similar information the disclosure of which clearly would constitute an unwarranted invasion of privacy. When a special master issues a decision or substantive order, the parties have 14 days within which to move for the redaction of privileged or confidential information before the document’s public disclosure. In this case, petitioners have elected to waive the 14-day period afforded for redaction requests prior to the public disclosure of an issued decision. In Petitioners’ Notice to Waive the 14-Day Waiting Period as Defined in Vaccine Rule 18(b) (Petitioners’ Waiver Notice), petitioners state that “none of the information they have furnished in their case is ‘private’ information.” Petitioners’ Waiver Notice at 1, filed on 1/26/10. Petitioners add that the “disclosure of any or all information they have furnished (continued...) CAMPBELL-SMITH, Special Master On January 29, 2003, George and Victoria Mead (petitioners or the Meads), as parents of William P. -
Behavioral Profiles of Clinically Referred Children with Intellectual Giftedness
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 540153, 7 pages http://dx.doi.org/10.1155/2013/540153 Research Article Behavioral Profiles of Clinically Referred Children with Intellectual Giftedness Fabian Guénolé,1 Jacqueline Louis,2 Christian Creveuil,3,4 Jean-Marc Baleyte,1,4 Claire Montlahuc,2 Pierre Fourneret,2,5 and Olivier Revol2 1 CHUdeCaen,ServicedePsychiatriedel’Enfantetdel’Adolescent,avenueClemenceau,14033CaenCedex9,France 2 Hospices Civils de Lyon, Service Hospitalo-Universitaire de Psychiatrie de l’Enfant et de l’Adolescent, Hopitalˆ Femme-Mere-Enfant,` 59boulevardPinel,69500Bron,France 3 CHU de Caen, Unite´ de Biostatistiques et de Recherche Clinique, avenue Clemenceau, 14033 Caen Cedex 9, France 4 UniversitedeNormandie,Facult´ edeM´ edecine,´ avenue de la Coteˆ de Nacre, 14032 Caen Cedex 5, France 5 Universite´ Claude Bernard Lyon-1, FacultedeM´ edecine´ Lyon Est, 8 avenue Rockefeller, 69373 Lyon Cedex 8, France Correspondence should be addressed to Fabian Guenol´ e;´ guenole [email protected] Received 21 April 2013; Revised 15 June 2013; Accepted 15 June 2013 Academic Editor: Harold K. Simon Copyright © 2013 Fabian Guenol´ e´ et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. It is common that intellectually gifted children—that is, children with an IQ ≥ 130—are referred to paediatric or child neuropsychiatry clinics for socio-emotional problems and/or school underachievement or maladjustment. These clinically-referred children with intellectual giftedness are thought to typically display internalizing problems (i.e., self-focused problems reflecting overcontrol of emotion and behavior), and to be more behaviorally impaired when “highly” gifted (IQ ≥ 145) or displaying developmental asynchrony (i.e., a heterogeneous developmental pattern, reflected in a significant verbal-performance discrepancy on IQ tests). -

The Safety of Vaccines for African American Children Immunization Is
The Safety of Vaccines for African American Children Immunization is one of the greatest health achievements in recent history. As public health advocates, we have witnessed firsthand the value of vaccination in protecting our children from dangerous, and potentially deadly, diseases. As outbreaks of these diseases begin to spread again across the country, we feel it is necessary to remind parents of the importance of ensuring the timely immunization of children of all races, ethnicities and genders in order to protect them from deadly infectious diseases. Recently, members of the African American community have become concerned that certain vaccines may not be safe for their children or that they may cause autism. This is simply not true. The worldwide scientific community has conducted multiple studies and reviews demonstrating that neither vaccines, nor components of vaccines, are linked to autism. Many of these published scientific studies are listed below. Vaccines are only licensed for use if safety and effectiveness are established through extensive clinical trials. Following licensure by the Food and Drug Administration (FDA), vaccines are recommended by the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices after additional, intense scrutiny of the safety, effectiveness and optimal timing of vaccinations. Further, once a vaccine is in use, several comprehensive systems are in place to continue to monitor the safety and effectiveness of each vaccine. These include the Vaccine Adverse Event Reporting System (VAERS), which accepts reports from any provider, patient, parent, or other person who is aware of any problem after vaccination. There are no indications that African American children are at a higher risk of rare side effects from vaccines than any other ethnic group. -

Materials to Help Convince Your Self-Funded Company to Provide an Insurance Benefit for Autism
Materials to Help Convince Your Self-funded Company to Provide an Insurance Benefit for Autism Lorri Unumb, Esq. Autism Speaks [email protected] Table of Contents Letter from Lorri . Presentation Slides . Sample Letters to the Company . List of Companies that offer an Autism Benefit . Examples of policy language . Letter from Lorri explaining the issue Sincerely yours, Lorri Shealy Unumb, J.D. Senior Policy Advisor & Counsel Autism Speaks Autism Coverage Benefits The Self-funded Company Lorri Unumb, Esq. Autism Speaks [email protected] What is Autism? • Autism is a medical condition, brought on through no fault of the family. • Autism affects a person’s communication abilities and social skills, and often causes repetitive patterns of behavior. • Autism is diagnosed by a medical doctor (usually a developmental pediatrician). • Treatment is prescribed by a medical doctor. “Autism” • The term “autism” is often used imprecisely: – some people use it interchangeably with “autism spectrum disorder” – others use it to mean one of the autism spectrum disorders. • In fact, there are 3 distinct diagnoses within the family of autism spectrum disorders. (See chart on next slide.) • Across the spectrum, people vary greatly in terms of type and severity of deficits. Pervasive There are 5 Pervasive Developmental Developmental Disorders (PDDs). Disorders Within the 5 PDDs, there are 3 Autism (the umbrella category Spectrum Disorders in the DSM-IV) (ASDs), shown in purple below. Autistic Asperge Pervasive r’s Disorder Developmental Syndro (classic me Disorder – Not autism) Otherwise Specified a/k/a “autism” (PDD-NOS) Less than Approx. ½ of all ASDs 1/3 of all 1/6 ASDs of all ASDs Rett’s Syndrome Curable? Treatable? • Although there is no known cure for autism, it can be treated so that the symptoms are not disabling. -

Autism Study by Dr. Eric Fombonne Is Inaccurate and Incomplete; Safeminds Aims to Correct Misinformation
For Immediate Release Contact: Alison Strock 202.628.7772 [email protected] Autism Study by Dr. Eric Fombonne is Inaccurate and Incomplete; SafeMinds Aims to Correct Misinformation Washington, DC – A Quebec study to be published in the July 2006 issue of Pediatrics, the official journal of the American Academy of Pediatrics, states that it is “very clear” that there is no relationship between mercury-based thimerosal in vaccines and the onset of autism. Dr. Eric Fombonne of the McGill University Health Center bases his opinion on a study among schoolchildren in Quebec, Canada. According to an analysis by SafeMinds, however, the study methodology is unlikely to lend itself to such declarative statements and should be treated with skepticism, for a number of reasons. The study looked at 27,749 students in grades kindergarten through 12th grade in a Montreal school district and found 187 cases of autism. The vast majority of these cases (more than 90%) were born in years in which thimerosal vaccines were widely used for infants in Quebec, as they were in the US. Only a tiny fraction of the autism students were born when thimerosal-free DTP and Hib vaccines were given, and these students may have been exposed to thimerosal from the Hepatitis B vaccine newly recommended for infants of foreign born parents, which made up over one fourth of the greater Montreal population. Dr. Fombonne wrongfully claims that large-population studies in the United States, England and Denmark also disprove a link between mercury and autism, and he states that “there is no autism epidemic.” He conveniently ignores the vast body of scientific evidence that has shown that environmental factors such as mercury may have caused the increased number of autism diagnoses in the US and other countries. -
Self-Funded Employer Tool Kit
Self-Funded Employer Tool Kit A tool kit to help families approach their self-funded “ERISA” employers about adding autism benefits to the company health plan February 2014 Dear Families: Thank you for requesting this information packet from Autism Speaks. It is our hope that these materials will help you convince your self-funded employer to offer meaningful autism benefits. The American population receives its health care coverage from a variety of sources. Some people have private health insurance arranged and paid for (perhaps partially) by their employers. Others purchase health insurance on their own in the individual market. As of January 2014, some Americans purchase insurance through “marketplaces” under the Affordable Care Act. Still others are insured through public insurance programs such as Medicaid or Medicare. Of the Americans whose insurance is provided through their employers, more than half are covered by health benefit plans that are not subject to state regulation. The largest body of non-state-regulated plans are self-insured or self-funded plans, which are plans provided by large employers who choose to pay claims from their own money rather than purchase a typical insurance policy for their employees. Many consumers do not know whether their employer-provided plan is a traditional insurance plan or a self-funded plan, largely because most insurance cards carried by consumers look essentially the same regardless of whether the coverage is traditional insurance or a self- funded plan. The cards look the same because most self-funded plans are administered by a company called a “third-party administrator,” and the third-party administrator is usually a health insurance company, such as Cigna or Aetna.