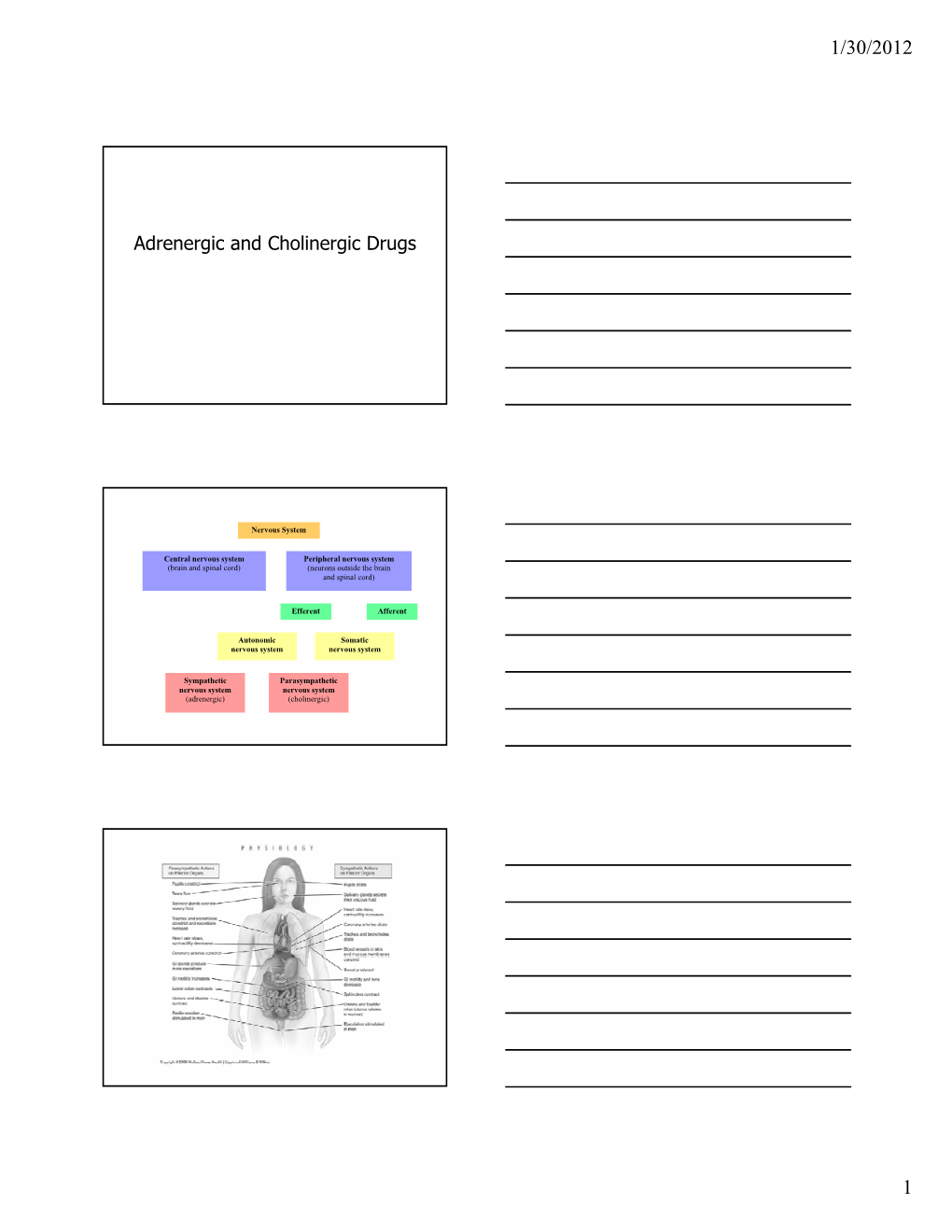
Adrenergic and Cholinergic Drugs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Table 2. 2012 AGS Beers Criteria for Potentially
Table 2. 2012 AGS Beers Criteria for Potentially Inappropriate Medication Use in Older Adults Strength of Organ System/ Recommendat Quality of Recomm Therapeutic Category/Drug(s) Rationale ion Evidence endation References Anticholinergics (excludes TCAs) First-generation antihistamines Highly anticholinergic; Avoid Hydroxyzin Strong Agostini 2001 (as single agent or as part of clearance reduced with e and Boustani 2007 combination products) advanced age, and promethazi Guaiana 2010 Brompheniramine tolerance develops ne: high; Han 2001 Carbinoxamine when used as hypnotic; All others: Rudolph 2008 Chlorpheniramine increased risk of moderate Clemastine confusion, dry mouth, Cyproheptadine constipation, and other Dexbrompheniramine anticholinergic Dexchlorpheniramine effects/toxicity. Diphenhydramine (oral) Doxylamine Use of diphenhydramine in Hydroxyzine special situations such Promethazine as acute treatment of Triprolidine severe allergic reaction may be appropriate. Antiparkinson agents Not recommended for Avoid Moderate Strong Rudolph 2008 Benztropine (oral) prevention of Trihexyphenidyl extrapyramidal symptoms with antipsychotics; more effective agents available for treatment of Parkinson disease. Antispasmodics Highly anticholinergic, Avoid Moderate Strong Lechevallier- Belladonna alkaloids uncertain except in Michel 2005 Clidinium-chlordiazepoxide effectiveness. short-term Rudolph 2008 Dicyclomine palliative Hyoscyamine care to Propantheline decrease Scopolamine oral secretions. Antithrombotics Dipyridamole, oral short-acting* May -

Severe Organophosphate Poisoning with Delayed Cholinergic Crisis, Intermediate Syndrome and Organophosphate Induced Delayed Polyneuropathy on Succession
Organophosphate Poisoning… Aklilu A 203 CASE REPORT SEVERE ORGANOPHOSPHATE POISONING WITH DELAYED CHOLINERGIC CRISIS, INTERMEDIATE SYNDROME AND ORGANOPHOSPHATE INDUCED DELAYED POLYNEUROPATHY ON SUCCESSION Aklilu Azazh ABSTRACT Organophosphate compounds are the organic derivatives of Phosphorous containing acids and their effect on neuromuscular junction and Autonomic Synapses is clinically important. After exposure these agents cause acute and sub acute manifestations depending on the type and severity of the agents like Acute Cholinergic Manifestations, Intermediate Syndrome with Nicotinic features and Delayed Central Nervous System Complications. The patient reported here had severe Organophosphate Poisoning with various rare complications on a succession. This is the first report of Organophosphates Poisoning complicated by Intermediate Syndrome and Organophosphate Induced Delayed Polyneuropathy in Ethiopia and it is reported to increase awareness of health care workers on these rare complications of a common problem. INTRODUCTION phosphorylated by the Phosphate end of Organophosphates; then the net result is Organophosphate compounds are the organic accumulation of excessive Acetyl Chlorine with derivatives of Phosphorous containing acids and resultant effect on Muscarinic, Nicotinic and their effect on Neuromuscular Junction and central nervous system (Figure 2). Autonomic synapses is clinically important. In the Neuromuscular Junction Acetylcholine is released Following classical OP poisoning, three well when a nerve impulse reaches -

Molecular Signatures of G-Protein-Coupled Receptors A
REVIEW doi:10.1038/nature11896 Molecular signatures of G-protein-coupled receptors A. J. Venkatakrishnan1, Xavier Deupi2, Guillaume Lebon1,3,4,5, Christopher G. Tate1, Gebhard F. Schertler2,6 & M. Madan Babu1 G-protein-coupled receptors (GPCRs) are physiologically important membrane proteins that sense signalling molecules such as hormones and neurotransmitters, and are the targets of several prescribed drugs. Recent exciting developments are providing unprecedented insights into the structure and function of several medically important GPCRs. Here, through a systematic analysis of high-resolution GPCR structures, we uncover a conserved network of non-covalent contacts that defines the GPCR fold. Furthermore, our comparative analysis reveals characteristic features of ligand binding and conformational changes during receptor activation. A holistic understanding that integrates molecular and systems biology of GPCRs holds promise for new therapeutics and personalized medicine. ignal transduction is a fundamental biological process that is comprehensively, and in the process expand the current frontiers of required to maintain cellular homeostasis and to ensure coordi- GPCR biology. S nated cellular activity in all organisms. Membrane proteins at the In this analysis, we objectively compare known structures and reveal cell surface serve as the communication interface between the cell’s key similarities and differences among diverse GPCRs. We identify a external and internal environments. One of the largest and most diverse consensus structural scaffold of GPCRs that is constituted by a network membrane protein families is the GPCRs, which are encoded by more of non-covalent contacts between residues on the transmembrane (TM) than 800 genes in the human genome1. GPCRs function by detecting a helices. -

Appendix A: Potentially Inappropriate Prescriptions (Pips) for Older People (Modified from ‘STOPP/START 2’ O’Mahony Et Al 2014)
Appendix A: Potentially Inappropriate Prescriptions (PIPs) for older people (modified from ‘STOPP/START 2’ O’Mahony et al 2014) Consider holding (or deprescribing - consult with patient): 1. Any drug prescribed without an evidence-based clinical indication 2. Any drug prescribed beyond the recommended duration, where well-defined 3. Any duplicate drug class (optimise monotherapy) Avoid hazardous combinations e.g.: 1. The Triple Whammy: NSAID + ACE/ARB + diuretic in all ≥ 65 year olds (NHS Scotland 2015) 2. Sick Day Rules drugs: Metformin or ACEi/ARB or a diuretic or NSAID in ≥ 65 year olds presenting with dehydration and/or acute kidney injury (AKI) (NHS Scotland 2015) 3. Anticholinergic Burden (ACB): Any additional medicine with anticholinergic properties when already on an Anticholinergic/antimuscarinic (listed overleaf) in > 65 year olds (risk of falls, increased anticholinergic toxicity: confusion, agitation, acute glaucoma, urinary retention, constipation). The following are known to contribute to the ACB: Amantadine Antidepressants, tricyclic: Amitriptyline, Clomipramine, Dosulepin, Doxepin, Imipramine, Nortriptyline, Trimipramine and SSRIs: Fluoxetine, Paroxetine Antihistamines, first generation (sedating): Clemastine, Chlorphenamine, Cyproheptadine, Diphenhydramine/-hydrinate, Hydroxyzine, Promethazine; also Cetirizine, Loratidine Antipsychotics: especially Clozapine, Fluphenazine, Haloperidol, Olanzepine, and phenothiazines e.g. Prochlorperazine, Trifluoperazine Baclofen Carbamazepine Disopyramide Loperamide Oxcarbazepine Pethidine -

Emerging Evidence for a Central Epinephrine-Innervated A1- Adrenergic System That Regulates Behavioral Activation and Is Impaired in Depression
Neuropsychopharmacology (2003) 28, 1387–1399 & 2003 Nature Publishing Group All rights reserved 0893-133X/03 $25.00 www.neuropsychopharmacology.org Perspective Emerging Evidence for a Central Epinephrine-Innervated a1- Adrenergic System that Regulates Behavioral Activation and is Impaired in Depression ,1 1 1 1 1 Eric A Stone* , Yan Lin , Helen Rosengarten , H Kenneth Kramer and David Quartermain 1Departments of Psychiatry and Neurology, New York University School of Medicine, New York, NY, USA Currently, most basic and clinical research on depression is focused on either central serotonergic, noradrenergic, or dopaminergic neurotransmission as affected by various etiological and predisposing factors. Recent evidence suggests that there is another system that consists of a subset of brain a1B-adrenoceptors innervated primarily by brain epinephrine (EPI) that potentially modulates the above three monoamine systems in parallel and plays a critical role in depression. The present review covers the evidence for this system and includes findings that brain a -adrenoceptors are instrumental in behavioral activation, are located near the major monoamine cell groups 1 or target areas, receive EPI as their neurotransmitter, are impaired or inhibited in depressed patients or after stress in animal models, and a are restored by a number of antidepressants. This ‘EPI- 1 system’ may therefore represent a new target system for this disorder. Neuropsychopharmacology (2003) 28, 1387–1399, advance online publication, 18 June 2003; doi:10.1038/sj.npp.1300222 Keywords: a1-adrenoceptors; epinephrine; motor activity; depression; inactivity INTRODUCTION monoaminergic systems. This new system appears to be impaired during stress and depression and thus may Depressive illness is currently believed to result from represent a new target for this disorder. -

Ketamine As a General Anesthesia Adjunct Michaela Wilcox, DNP
Ketamine as a General Anesthesia Adjunct Michaela Wilcox, DNP (c), RN Dept. of Nurse Anesthesia, Moffett & Sanders School of Nursing, Samford University Structured Abstract Background Ketamine is a unique anesthetic agent with both anesthetic and analgesic properties. Ketamine is primarily a N-Methyl-D-Aspartic acid (NMDA) antagonist that also works on glutamine, nicotinic, muscarinic, monoaminergic and opioid receptors. The uses of ketamine are numerous and include treatment of chronic pain, acute pain, depression, as a multimodal pain adjunct, opioid-sparing agent and as an adjunct in enhanced recovery after surgery (ERAS) protocols. A 49-year-old female presented for a lumbar lateral interbody fusion extreme, anterior lumbar spine arthrodesis L3/4 with revision and instrumentation. Based on the surgical need for both sensory and motor nerve monitoring intraoperatively, the anesthetic plan included minimal sevoflurane, succinylcholine for induction and a propofol intravenous (IV) infusion with boluses of ketamine to maintain unconsciousness. A bispectral index (BIS) monitor (Aspect Medical Systems, Natick, MA) was placed on the patient’s forehead prior to induction and utilized intraoperatively to maintain a goal of 40-60. General anesthesia was achieved with fentanyl 100 mcg, lidocaine 100 mg, propofol 200 mg, ketamine 50 mg and succinylcholine 160 mg IV. Laryngoscopy was successfully performed using a McGrath MAC video laryngoscope (Medtronic, Minneapolis, MN). Following induction, a propofol IV infusion was initiated and sevoflurane maintained at 0.3 minimum alveolar concentration. Ketamine 10 mg IV was administered every hour. Upon conclusion of the procedure, the patient was extubated and transported to postoperative recovery unit, where she had no complaints of nausea, vomiting or pain. -

(Antimuscarinic) Drugs?
© July - August 2018 How well do you know your anticholinergic (antimuscarinic) drugs? nticholinergic drugs, prescribed for a variety of clini- Acal conditions, are amongst the most frequently used prescription drugs in BC (Table 1). Also referred to as “an- timuscarinics,” such drugs specifically block muscarinic receptors for acetylcholine (ACh).1 Muscarinic ACh recep- tors are important in the parasympathetic nervous system that governs heart rate, exocrine glands, smooth muscles, clude drugs whose active metabolites are potent- as well as brain function. In contrast, nicotinic ACh recep- ly antimuscarinic,5 or which often cause typical tors stimulate contraction of striated muscles. This Letter is AC adverse effects such as dry mouth or urinary intended to remind clinicians of commonly used drugs that retention.6 People taking antihistamines, antide- have anticholinergic (AC), or technically, antimuscarinic pressants, antipsychotics, opioids, antimuscarinic properties, and of their potential adverse effects. inhalers, or many other drugs need to know that Beneficial and harmful effects of anticholinergic drugs have blockade of ACh receptors can cause bothersome been known for centuries. In Homer’s Odyssey, the nymph or even dangerous adverse effects (Table 3). pharmacologist Circe utilized central effects of atropinics Subtle and not-so-subtle toxicity in the common plant jimson weed (Datura stramonium) to cause delusions in the crew of Odysseus. Believing they Students often learn the adverse effects of anticho- had been turned into pigs, they could be herded.2 linergics from a mnemonic, e.g.: “Blind as a bat, Sometimes a drug is recommended specifically for its an- mad as a hatter, red as a beet, hot as a hare, dry as ticholinergic potency. -

Reference List of Drugs with Potential Anticholinergic Effects 1, 2, 3, 4, 5
ANTICHOLINERGICS: Reference List of Drugs with Potential Anticholinergic Effects 1, 2, 3, 4, 5 J Bareham BSP © www.RxFiles.ca Aug 2021 WHENEVER POSSIBLE, AVOID DRUGS WITH MODERATE TO HIGH ANTICHOLINERGIC ACTIVITY IN OLDER ADULTS (>65 YEARS OF AGE) Low Anticholinergic Activity; Moderate/High Anticholinergic Activity -B in combo Beers Antibiotics Antiparkinsonian Cardiovascular Agents Immunosuppressants ampicillin *ALL AVAILABLE AS amantadine SYMMETREL atenolol TENORMIN azaTHIOprine IMURAN cefOXitin GENERIC benztropine mesylate COGENTIN captopril CAPOTEN cyclosporine NEORAL clindamycin bromocriptine PARLODEL chlorthalidone GENERIC ONLY hydrocortisone CORTEF gentamicin (Oint & Sol’n NIHB covered) carbidopa/levodopa SINEMET digoxin LANOXIN, TOLOXIN methylprednisolone MEDROL piperacillin entacapone COMTAN dilTIAZem CARDIZEM, TIAZAC prednisone WINPRED dipyridamole PERSANTINE, ethopropazine PARSITAN vancomycin phenelzine NARDIL AGGRENOX disopyramide RYTHMODAN Muscle Relaxants pramipexole MIRAPEX Antidepressants baclofen LIORESAL ( on intrathecal only) procyclidine KEMADRIN furosemide LASIX amitriptyline ELAVIL cyclobenzaprine FLEXERIL selegiline ELDEPRYL hydrALAZINE APRESOLINE clomiPRAMINE ANAFRANIL isosorbide ISORDIL methocarbamol ROBAXIN OTC trihexyphenidyl ARTANE desipramine NORPRAMIN metoprolol LOPRESOR orphenadrine NORFLEX OTC doxepin >6mg SINEQUAN Antipsychotics NIFEdipine ADALAT tiZANidine ZANAFLEX A imipramine TOFRANIL quiNIDine GENERIC ONLY C ARIPiprazole ABILIFY & MAINTENA -

Protocol for a Randomised Controlled Trial: Efficacy of Donepezil Against
BMJ Open: first published as 10.1136/bmjopen-2013-003533 on 25 September 2013. Downloaded from Open Access Protocol Protocol for a randomised controlled trial: efficacy of donepezil against psychosis in Parkinson’s disease (EDAP) Hideyuki Sawada, Tomoko Oeda To cite: Sawada H, Oeda T. ABSTRACT ARTICLE SUMMARY Protocol for a randomised Introduction: Psychosis, including hallucinations and controlled trial: efficacy of delusions, is one of the important non-motor problems donepezil against psychosis Strengths and limitations of this study in patients with Parkinson’s disease (PD) and is in Parkinson’s disease ▪ In previous randomised controlled trials for (EDAP). BMJ Open 2013;3: possibly associated with cholinergic neuronal psychosis the efficacy was investigated in patients e003533. doi:10.1136/ degeneration. The EDAP (Efficacy of Donepezil against who presented with psychosis and the primary bmjopen-2013-003533 Psychosis in PD) study will evaluate the efficacy of endpoint was improvement of psychotic symp- donepezil, a brain acetylcholine esterase inhibitor, for toms. By comparison, this study is designed to prevention of psychosis in PD. ▸ Prepublication history for evaluate the prophylactic effect in patients this paper is available online. Methods and analysis: Psychosis is assessed every without current psychosis. Because psychosis To view these files please 4 weeks using the Parkinson Psychosis Questionnaire may be overlooked and underestimated it is visit the journal online (PPQ) and patients with PD whose PPQ-B score assessed using a questionnaire, Parkinson (http://dx.doi.org/10.1136/ (hallucinations) and PPQ-C score (delusions) have Psychosis Questionnaire (PPQ) every 4 weeks. bmjopen-2013-003533). been zero for 8 weeks before enrolment are ▪ The strength of this study is its prospective randomised to two arms: patients receiving donepezil design using the preset definition of psychosis Received 3 July 2013 hydrochloride or patients receiving placebo. -

The Role of Serotonin in Memory: Interactions with Neurotransmitters and Downstream Signaling
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Bushehr University of Medical Sciences Repository Exp Brain Res (2014) 232:723–738 DOI 10.1007/s00221-013-3818-4 REVIEW The role of serotonin in memory: interactions with neurotransmitters and downstream signaling Mohammad Seyedabadi · Gohar Fakhfouri · Vahid Ramezani · Shahram Ejtemaei Mehr · Reza Rahimian Received: 28 April 2013 / Accepted: 20 December 2013 / Published online: 16 January 2014 © Springer-Verlag Berlin Heidelberg 2014 Abstract Serotonin, or 5-hydroxytryptamine (5-HT), is there has been an alteration in the density of serotonergic found to be involved in many physiological or pathophysi- receptors in aging and Alzheimer’s disease, and serotonin ological processes including cognitive function. Seven dis- modulators are found to alter the process of amyloidogen- tinct receptors (5-HT1–7), each with several subpopulations, esis and exert cognitive-enhancing properties. Here, we dis- have been identified for serotonin, which are different in cuss the serotonin-induced modulation of various systems terms of localization and downstream signaling. Because involved in mnesic function including cholinergic, dopa- of the development of selective agonists and antagonists minergic, GABAergic, glutamatergic transmissions as well for these receptors as well as transgenic animal models as amyloidogenesis and intracellular pathways. of cognitive disorders, our understanding of the role of serotonergic transmission in learning and memory has Keywords Serotonin · Memory · Signaling pathways improved in recent years. A large body of evidence indi- cates the interplay between serotonergic transmission and Abbreviations other neurotransmitters including acetylcholine, dopamine, 2PSDT Two-platform spatial discrimination task γ-aminobutyric acid (GABA) and glutamate, in the neu- 3xTg-AD Triple-transgenic mouse model of Alzheimer’s robiological control of learning and memory. -

Nicotine and Neurotransmitters
Module 2 —Legal Doesn’t Mean Harmless Overview Overview Summary This module focuses on how two drugs, nicotine and alcohol, change the functioning of the brain and body. Both drugs are widely used in the community, and for adults, using them is legal. Nonetheless, both alcohol and nicotine can have a strong impact on the functioning of the brain. Each can cause a number of negative effects on the body and brain, ranging from mild symptoms to addiction. The goal of this module is to help students understand that, although nicotine and alcohol are legal for adults, they are not harmless substances. Students will learn about how nicotine and alcohol change or disrupt the process of neurotransmission. Students will explore information on the short- and long- term effects of these two drugs, and also learn why these drugs are illegal for children and teens. Through the media, students are exposed to a great deal of information about alcohol and tobacco, much of which is misleading or scientifically inaccurate. This module will provide information on what researchers have learned about how nicotine and alcohol change the brain, and the resulting implications for safety and health. Learning Objectives At the end of this module: • Students can explain how nicotine disrupts neurotransmission. • Students can explain how alcohol use may harm the brain and the body. • Students understand how alcohol can intensify the effect of other drugs. • Students can define addiction and understand its basis in the brain. • Students draw conclusions about why our society regulates the use of nicotine and alcohol for young people. -

Covalent Agonists for Studying G Protein-Coupled Receptor Activation
Covalent agonists for studying G protein-coupled receptor activation Dietmar Weicherta, Andrew C. Kruseb, Aashish Manglikb, Christine Hillera, Cheng Zhangb, Harald Hübnera, Brian K. Kobilkab,1, and Peter Gmeinera,1 aDepartment of Chemistry and Pharmacy, Friedrich Alexander University, 91052 Erlangen, Germany; and bDepartment of Molecular and Cellular Physiology, Stanford University School of Medicine, Stanford, CA 94305 Contributed by Brian K. Kobilka, June 6, 2014 (sent for review April 21, 2014) Structural studies on G protein-coupled receptors (GPCRs) provide Disulfide-based cross-linking approaches (17, 18) offer important insights into the architecture and function of these the advantage that the covalent binding of disulfide-containing important drug targets. However, the crystallization of GPCRs in compounds is chemoselective for cysteine and enforced by the active states is particularly challenging, requiring the formation of affinity of the ligand-pharmacophore rather than by the elec- stable and conformationally homogeneous ligand-receptor com- trophilicity of the cross-linking function (19). We refer to the plexes. Native hormones, neurotransmitters, and synthetic ago- described ligands as covalent rather than irreversible agonists nists that bind with low affinity are ineffective at stabilizing an because cleavage may be promoted by reducing agents and the active state for crystallogenesis. To promote structural studies on disulfide transfer process is a reversible chemical reaction the pharmacologically highly relevant class