By a Treatise Submitted in Partial Fulfilment of the Requirements for The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Property Information Pack
RETAIL INVESTMENT FOR SALE BY GILLITTS SHOPPING CENTRE, 16 YORK AUCTION ROAD, GILLITTS, KWAZULU-NATAL WEB#: AUCT-000344 | www.in2assets.com ADDRESS: Gillitts Shopping Centre, 16 York Road, Gillitts, Kwa-Zulu Natal AUCTION VENUE: The Durban Country Club, Isaiah Ntshangase Road, Durban AUCTION DATE & TIME: 06 December 2016 | 11h00 VIEWING: By Appointment CONTACT: Carl Kleinhans | 082 467 5664 | 031 574 7600 | [email protected] REGISTRATION FEE: R 50 000-00 (Refundable Bank Guaranteed Cheque) AUCTIONEER: Andrew Miller The Rules of Auction can be viewed at www.In2assets.com or at Unit 504, 5th Floor, Strauss Daly Place, 41 Richefond Circle, Ridgeside Office Park, Umhlanga Ridge. Bidders must register to bid and provide original proof of identity and residence on registration. The Rules of Auction contain the registration requirements if you intend to bid on behalf of another person or an entity. The above property is subject to a reserve price and the sale by auction is subject to a right to bid by or on behalf of the owner or auctioneer. CONTENTS GILLITTS SHOPPING CENTRE, 16 YORK ROAD, GILLITTS, KWAZULU-NATAL 1318 Old North Coast Road, Avoca CPA LETTER 2 PROPERTY DESCRIPTION 3 PROPERTY LOCATION 5 PICTURE GALLERY 6 ADDITIONAL INFORMATION 8 LETTER OF INTEREST 10 TERMS AND CONDITIONS 12 SG DIAGRAM 13 ZONING CERTIFICATE 16 SECTIONAL TITLE PLANS 18 BODY CORPORATE RULES 31 CERTIFICATE OF REAL RIGHT 35 TITLE DEED 38 DISCLAIMER: Whilst all reasonable care has been taken to provide accurate information, neither In2assets Properties (Pty) Ltd nor the Seller/s guarantee the correctness of the information, provided herein and neither will be held liable for any direct or indirect damages or loss, of whatsoever nature, suffered by any person as a result of errors or omissions in the information provided, whether due to the negligence or otherwise of In2assets Properties (Pty) Ltd or the Sellers or any other person. -

Directory of Organisations and Resources for People with Disabilities in South Africa
DISABILITY ALL SORTS A DIRECTORY OF ORGANISATIONS AND RESOURCES FOR PEOPLE WITH DISABILITIES IN SOUTH AFRICA University of South Africa CONTENTS FOREWORD ADVOCACY — ALL DISABILITIES ADVOCACY — DISABILITY-SPECIFIC ACCOMMODATION (SUGGESTIONS FOR WORK AND EDUCATION) AIRLINES THAT ACCOMMODATE WHEELCHAIRS ARTS ASSISTANCE AND THERAPY DOGS ASSISTIVE DEVICES FOR HIRE ASSISTIVE DEVICES FOR PURCHASE ASSISTIVE DEVICES — MAIL ORDER ASSISTIVE DEVICES — REPAIRS ASSISTIVE DEVICES — RESOURCE AND INFORMATION CENTRE BACK SUPPORT BOOKS, DISABILITY GUIDES AND INFORMATION RESOURCES BRAILLE AND AUDIO PRODUCTION BREATHING SUPPORT BUILDING OF RAMPS BURSARIES CAREGIVERS AND NURSES CAREGIVERS AND NURSES — EASTERN CAPE CAREGIVERS AND NURSES — FREE STATE CAREGIVERS AND NURSES — GAUTENG CAREGIVERS AND NURSES — KWAZULU-NATAL CAREGIVERS AND NURSES — LIMPOPO CAREGIVERS AND NURSES — MPUMALANGA CAREGIVERS AND NURSES — NORTHERN CAPE CAREGIVERS AND NURSES — NORTH WEST CAREGIVERS AND NURSES — WESTERN CAPE CHARITY/GIFT SHOPS COMMUNITY SERVICE ORGANISATIONS COMPENSATION FOR WORKPLACE INJURIES COMPLEMENTARY THERAPIES CONVERSION OF VEHICLES COUNSELLING CRÈCHES DAY CARE CENTRES — EASTERN CAPE DAY CARE CENTRES — FREE STATE 1 DAY CARE CENTRES — GAUTENG DAY CARE CENTRES — KWAZULU-NATAL DAY CARE CENTRES — LIMPOPO DAY CARE CENTRES — MPUMALANGA DAY CARE CENTRES — WESTERN CAPE DISABILITY EQUITY CONSULTANTS DISABILITY MAGAZINES AND NEWSLETTERS DISABILITY MANAGEMENT DISABILITY SENSITISATION PROJECTS DISABILITY STUDIES DRIVING SCHOOLS E-LEARNING END-OF-LIFE DETERMINATION ENTREPRENEURIAL -

Ward Councillors Pr Councillors Executive Committee
EXECUTIVE COMMITTEE KNOW YOUR CLLR WEZIWE THUSI CLLR SIBONGISENI MKHIZE CLLR NTOKOZO SIBIYA CLLR SIPHO KAUNDA CLLR NOMPUMELELO SITHOLE Speaker, Ex Officio Chief Whip, Ex Officio Chairperson of the Community Chairperson of the Economic Chairperson of the Governance & COUNCILLORS Services Committee Development & Planning Committee Human Resources Committee 2016-2021 MXOLISI KAUNDA BELINDA SCOTT CLLR THANDUXOLO SABELO CLLR THABANI MTHETHWA CLLR YOGISWARIE CLLR NICOLE GRAHAM CLLR MDUDUZI NKOSI Mayor & Chairperson of the Deputy Mayor and Chairperson of the Chairperson of the Human Member of Executive Committee GOVENDER Member of Executive Committee Member of Executive Committee Executive Committee Finance, Security & Emergency Committee Settlements and Infrastructure Member of Executive Committee Committee WARD COUNCILLORS PR COUNCILLORS GUMEDE THEMBELANI RICHMAN MDLALOSE SEBASTIAN MLUNGISI NAIDOO JANE PILLAY KANNAGAMBA RANI MKHIZE BONGUMUSA ANTHONY NALA XOLANI KHUBONI JOSEPH SIMON MBELE ABEGAIL MAKHOSI MJADU MBANGENI BHEKISISA 078 721 6547 079 424 6376 078 154 9193 083 976 3089 078 121 5642 WARD 01 ANC 060 452 5144 WARD 23 DA 084 486 2369 WARD 45 ANC 062 165 9574 WARD 67 ANC 082 868 5871 WARD 89 IFP PR-TA PR-DA PR-IFP PR-DA Areas: Ebhobhonono, Nonoti, Msunduzi, Siweni, Ntukuso, Cato Ridge, Denge, Areas: Reservoir Hills, Palmiet, Westville SP, Areas: Lindelani C, Ezikhalini, Ntuzuma F, Ntuzuma B, Areas: Golokodo SP, Emakhazini, Izwelisha, KwaHlongwa, Emansomini Areas: Umlazi T, Malukazi SP, PR-EFF Uthweba, Ximba ALLY MOHAMMED AHMED GUMEDE ZANDILE RUTH THELMA MFUSI THULILE PATRICIA NAIR MARLAINE PILLAY PATRICK MKHIZE MAXWELL MVIKELWA MNGADI SIFISO BRAVEMAN NCAYIYANA PRUDENCE LINDIWE SNYMAN AUBREY DESMOND BRIJMOHAN SUNIL 083 7860 337 083 689 9394 060 908 7033 072 692 8963 / 083 797 9824 076 143 2814 WARD 02 ANC 073 008 6374 WARD 24 ANC 083 726 5090 WARD 46 ANC 082 7007 081 WARD 68 DA 078 130 5450 WARD 90 ANC PR-AL JAMA-AH 084 685 2762 Areas: Mgezanyoni, Imbozamo, Mgangeni, Mabedlane, St. -
MCCURACH SWART Homegrown Qualities
MCCURACH MCCURACH SWART Homegrown Qualities McCurrach & Swart has been a family-owned and family-run business since its beginnings BUSINESS in 1969. Master Builder Rupert Swart and INFORMATION son Brett share the same unwavering Business Name: commitment to delivering quality builds. McCurrach & Swart Together, they are highly experienced in Construction CC a diversity of builds including commercial, Business Address: 13 Eagle Rock, industrial, new builds, developments, 90 St. Helier Rd, renovations and specialised alterations. Gillitts, KZN, South Africa Over the decades, McCurrach & Swart has constructed NHBRC-registered a rock solid industry reputation as the go-to business for challenging projects requiring high levels of personal attention, as well as rapid turnaround time without compromise on top end finishes. Our hands on approach has led many top architects and engineers to choose to partner specifically with McCurrach & Swart. Our collaborative style often sees us working closely with these parties and with the client, all the way from project inception to the final selection of finishes. House of the Year Contender 2015, H+L. KwaZulu-Natal, S.A. Our Strategy PURPOSE To be a leader in the construction industry by building close relationships with our esteemed key clients and suppliers. VISION To provide a quality service that exceeds expectations, rather than simply meeting them. CORE VALUES We treat our staff and our clients with complete trust and respect. Our company culture is supportive and promotes skills development. We thrive on innovation and its application. We demonstrate transparency and integrity in all aspects of our business dealings. We aim to streamline costs and resource utilisation while minimising environmental impact. -

Highway Heritage Society Newsletter 101- 2018-03
HIGHWAY HERITAGE SOCIETY P.O. Box 1295 3640 KLOOF Tel/Fax 031 7644721 [email protected] MARCH 2018 NEWSLETTER CHAIRMAN’S CHATTER As a result of comments made at our meeting on 3 February about the Halsted farmhouse at Emberton having been demolished, I decided to go to Emberton Estate to check for myself. I am grateful to Mr Paul Smith, the estate manager, who kindly allowed me access to the old house which has been refurbished beautifully as the Estate Clubhouse. Some leeway was needed to allow for it now being used by many people and it will be seen that the left and right front veranda has been closed in to make way for toilet facilities. Back and side verandas have also been added. I am sure that William & Elizabeth Gillitt would approve! As will be seen from some of the photos in the article below the weather was a little overcast as has been the case on numerous days of late! The presentation at our upcoming meeting will be a longish one and it will be necessary to start promptly so as not to encroach too much into teatime and you are therefore requested not to be late! TALK AND SLIDE PRESENTATION ON 24 MARCH 2018 Subject: “The fate of Convoy DN21 - 1943” Speakers: Adrian Rowe will speak on a subject which is dear to his heart, as his grandfather was a military veterinary surgeon aboard SS Nirpura when it was torpedoed by U-160. Date & time: Saturday 24 March 2018 at 14h00 sharp (2.00 p.m.). -

Hillcrest and Its Contribution to Natal Education
55 Hillcrest and its contribution to Natal Education The town of Hillcrest, with an official population in 1985 of 5291,' a borough register in 1987 of 1 345 properties and an estimated municipal expenditure in 1987-88 of approximately R1 million,2 lies amid the hills, thirty five kilometres west of Durban, on the old main road to Pietermaritzburg. Many of its residents commute daily to the multifarious enterprises of the Pinetown-Durban conurbation. Hillcrest has enjoyed town status only since 1971 and the older inhabitants, who once retired to the country, recall nostalgically the village days, when no traffic lights were necessary and when a single store served the needs of the entire community. Even among these senior citizens, however, are few who can remember the days when Hill Crest (as it was originally written) had as many as five schools and made a significant if small contribution to education in Natal. The Hillcrest railway station was (in times pre-metric) recorded as being 2 225 ft above sea-IeveJ.3 The climate, therefore, is temperate and less taxing, especially at midsummer, than the humidity of the coast. The entire region, furthermore, is well watered, with numerous streams draining in the north to the Umgeni and in the south to the Umhlatuzana, which rises a few kilometres north-west of Hillcrest, behind the eminence known as Botha's Hill. Many farm names in the area (Sterkspruit, LangeJontein, BuJfelJjontein) attest to the abundance of water, which is supplemented by characteristic seasonal mists, keeping the hills green even in the grip of winter. -

Nansook, Ahsha Thesis 2008.Pdf
DECLARATION Submitted in partial fulfilment of the requirements for the degree of Masters of Town and Regional Planning, in the Graduate Programme in the School of Architecture, Planning and Housing, University of KwaZulu-Natal, Durban, South Africa. I declare that this dissertation is my own unaided work. All citations, references and borrowed ideas have been duly acknowledged. It is being submitted for the degree of Masters of Town and Regional Planning in the Faculty of Humanities, Development and Social Science, University of KwaZulu-Natal, Durban, South Africa. None of the present work has been submitted previously for any degree or examination in any other University. AHSHA NANSOOK Student Name 10 MARCH 2009 Date i ACKNOWLEDGEMENTS First and foremost I would like to thank Lord Krishna for giving me the strength and determination to complete the dissertation. I humbly bow down to your lotus feet. I would like to express my sincere gratitude to a number of people who have supported me throughout this process. Thank you to my Supervisor, Professor Peter Robinson for your guidance and direction. Thank you professor for your knowledge, expertise and kindness. I am forever indebted to you. To my dear husband, Ashok, thank you for your patience and support. I could not have done this without your strong belief in my ability. Thank you so much for your encouragement and for being a wonderful husband. To my precious son, Nikhil, I am sorry to have spent so much of time on the computer and so little time with you in the last few months. Thank you for constantly making sure that I was facing my responsibility as a mum. -

C/O Chairman 14 Edgecliffe Park 14 Bartle Road Gillitts 3610 THE
C/O Chairman 14 Edgecliffe Park 14 Bartle Road Gillitts 3610 www.durbanramblers.co.za Banking Details: Standard Bank Musgrave Rd. Branch Code: 042626 Account No: 051257653 THE OFFICIAL MAGAZINE OF THE DURBAN RAMBLERS’ HIKING CLUB 3rd QUARTER: JULY – SEPTEMBER 2013 CHAIRMAN’S RAMBLINGS The KwaZulu Natal autumn and winter months are just wonderful, just the right temperature for hiking. And if that is not what gets you outdoors, it must be the aloes in bloom. In July we normally join Francois from the Pietermaritzburg Ramblers for their annual Mpushini Aloe walk. I am sure this year it will again be well attended by our members. In the quarter July to end September, Lois and I will again host the Potjie competition. I am sure a number of our members will volunteer to be cooks and many others of you will be those, oh so critical, but all important judges. If you are the winning cook you may feel that you are up to joining the Braai Master competition. Look out for the date in the programme and book early as space is limited. I must thank Trevor, ably assisted by Philip Collyer and Linda Smith, for leading a hike for the Getaway Magazine, co-sponsored by Hi-Tec Footwear. I just hope that both HI-Tec and The Getaway magazine appreciate their hard work which contributed to making it a success. It is most important that when hiking you walk in a group. I do not want to be alarmist, but on the Burman Bush hike someone who was not feeling well, together with a friend (thus not alone) decided to turn back, and they were mugged. -

Following Is a Load Shedding Schedule That People Are Advised to Keep
Following is a load shedding schedule that people are advised to keep. STAND-BY LOAD SHEDDING SCHEDULE Monday Tuesday Wednesday Thursday Friday Saturday Sunday Block A 04:00-06:30 08:00-10:30 04:00-06:30 08:00-10:30 04:00-06:30 08:00-10:30 08:00-10:30 Block B 06:00-08:30 14:00-16:30 06:00-08:30 14:00-16:30 06:00-08:30 14:00-16:30 14:00-16:30 Block C 08:00-10:30 16:00-18:30 08:00-10:30 16:00-18:30 08:00-10:30 16:00-18:30 16:00-18:30 Block D 10:00-12:30 12:00-14:30 10:00-12:30 12:00-14:30 10:00-12:30 12:00-14:30 12:00-14:30 Block E 12:00-14:30 10:00-12:30 12:00-14:30 10:00-12:30 12:00-14:30 10:00-12:30 10:00-12:30 Block F 14:00-16:30 18:00-20:30 14:00-16:30 18:00-20:30 14:00-16:30 18:00-20:30 18:00-20:30 Block G 16:00-18:30 20:00-22:30 16:00-18:30 20:00-22:30 16:00-18:30 20:00-22:30 20:00-22:30 Block H 18:00-20:30 04:00-06:30 18:00-20:30 04:00-06:30 18:00-20:30 04:00-06:30 04:00-06:30 Block J 20:00-22:30 06:00-08:30 20:00-22:30 06:00-08:30 20:00-22:30 06:00-08:30 06:00-08:30 Area Block Albert Park Block D Amanzimtoti Central Block B Amanzimtoti North Block B Amanzimtoti South Block B Asherville Block H Ashley Block J Assagai Block F Athlone Block G Atholl Heights Block J Avoca Block G Avoca Hills Block C Bakerville Gardens Block G Bayview Block B Bellair Block A Bellgate Block F Belvedere Block F Berea Block F Berea West Block F Berkshire Downs Block E Besters Camp Block F Beverly Hills Block C Blair Atholl Block J Blue Lagoon Block D Bluff Block E Bonela Block E Booth Road Industrial Block E Bothas Hill Block F Briardene Block G Briardene -
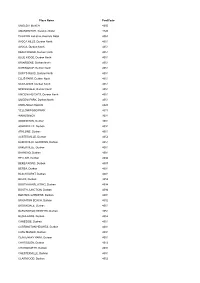
Place Name Postcode UMDLOTI BEACH 4350 AMANZIMTOTI
Place Name PostCode UMDLOTI BEACH 4350 AMANZIMTOTI, Kwazulu Natal 4126 PHOENIX Industria, Kwazulu Natal 4068 AVOCA HILLS, Durban North 4051 AVOCA, Durban North 4051 BEACHWOOD, Durban North 4051 BLUE RIDGE, Durban North 4051 BRIARDENE, Durban North 4051 DORINGKOP, Durban North 4051 DUFF'S ROAD, Durban North 4051 ELLIS PARK, Durban North 4051 NEWLANDS, Durban North 4051 SPRINGVALE, Durban North 4051 UMGENI HEIGHTS, Durban North 4051 UMGENI PARK, Durban North 4051 UMHLANGA ROCKS 4320 YELLOWWOOD PARK 4011 WANDSBECK 3631 ADDINGTON, Durban 4001 ASHERVILLE, Durban 4091 ATHLONE, Durban 4051 AUSTERVILLE, Durban 4052 BAKERVILLE GARDENS, Durban 4051 BAKERVILLE, Durban 4051 BAYHEAD, Durban 4001 BELLAIR, Durban 4094 BEREA ROAD, Durban 4007 BEREA, Durban 4001 BLACKHURST, Durban 4001 BLUFF, Durban 4052 BOOTH AANSLUITING, Durban 4094 BOOTH JUNCTION, Durban 4094 BOTANIC GARDENS, Durban 4001 BRIGHTON BEACH, Durban 4052 BROOKDALE, Durban 4051 BURLINGTON HEIGHTS, Durban 4051 BUSHLANDS, Durban 4052 CANESIDE, Durban 4051 CARRINGTON HEIGHTS, Durban 4001 CATO MANOR, Durban 4091 CENTENARY PARK, Durban 4051 CHATSGLEN, Durban 4012 CHATSWORTH, Durban 4092 CHESTERVILLE, Durban 4001 CLAIRWOOD, Durban 4052 CLARE Est/Lgd, Durban 4091 CLAYFIELD, Durban 4051 CONGELLA, Durban 4001 DALBRIDGE, Durban 4001 DORMERTON, Durban 4091 DURBAN NORTH, Durban 4051 DURBAN-NOORD, Durban 4051 Durban International Airport, Durban 4029 EARLSFIELD, Durban 4051 EAST END, Durban 4018 EASTBURY, Durban 4051 EFFINGHAM HEIGHTS, Durban 4051 FALLODEN PARK, Durban 4094 FLORIDA ROAD, Durban 4019 FOREST -

22 Tewkesbury Crescent Cotswold Downs Estate, Hillcrest
RESIDENTIAL PROPERTY ONLINE LIVE AUCTION 22 TEWKESBURY CRESCENT COTSWOLD DOWNS ESTATE, HILLCREST TUESDAY, 23 JULY 2020 @ 11:00 AM ONLINE LIVE “ZOOM” AUCTION ANDREW GIDDY: 082 601 9278 |031 – 579 4403 www.ianwyles.co.za VIEW BY APPOINTMENT ONLY Terms & Conditions Please note that in order to be approved for bidding, you are required to send us: Proof of Payment & Original Proof of FICA Documents. R 50 000 refundable deposit (strictly cash transfer only). All bids are exclusive of commission + VAT. Ian Wyles Auctioneers may bid up to reserve on behalf of the sellers. subject to change without notification. Auctioneer: Ian Wyles 1 CONTENTS COTSWOLD DOWNS ESTATE, HILLCREST Property Summary Locality Maps Pictures Additional Information Auction Information Deposit 5% of bid price payable by The Purchaser on the fall of the hammer Commission 10% plus VAT thereon of the bid price payable by the Purchaser on the fall of the hammer Terms and Conditions If you are the successful bidder, the following is applicable: • 30 Day Guarantee Period from confirmation of sale by the Seller • Possession & occupation of property on registration • Electrical (including electric fencing), woodborer and gas compliance for the Purchaser’s account, if applicable Banking Details Ian Wyles Auctioneers and Appraisers (PTY) LTD Account Number – 40-9642-2381 Branch Name – Absa Bank Durban North Swift Code – ABSA ZA JJ Branch Code – 632005 Reference: Use Name and Property Address 2 Disclaimer Whilst all reasonable care has been taken to provide accurate information, neither -
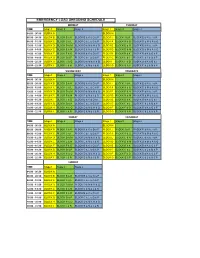
Load Schedule S4.Xlsx
EMERGENCY LOAD SHEDDING SCHEDULE MONDAY TUESDAY TIME Stage 1 Stage 2 Stage 3 Stage 1 Stage 2 Stage 3 04:00 - 06:30 BLOCK A BLOCK H 06:00 - 08:30 BLOCK B BLOCK B & K BLOCK B & K & O & F BLOCK J BLOCK J & R BLOCK E & N & J & R 08:00 - 10:30 BLOCK C BLOCK C & L BLOCK C & L & G & P BLOCK A BLOCK A & Q BLOCK D & M & A & Q 10:00 - 12:30 BLOCK D BLOCK D & M BLOCK D & M & H & Q BLOCK E BLOCK E & N BLOCK E & N & J & R 12:00 - 14:30 BLOCK E BLOCK E & N BLOCK E & N & J & R BLOCK D BLOCK D & M BLOCK D & M & A & Q 14:00 - 16:30 BLOCK F BLOCK F & O BLOCK B & K & O & F BLOCK B BLOCK B & K BLOCK B & K & O & F 16:00 - 18:30 BLOCK G BLOCK G & P BLOCK C & L & G & P BLOCK C BLOCK C & L BLOCK C & L & G & P 18:00 - 20:30 BLOCK H BLOCK H & Q BLOCK D & M & H & Q BLOCK F BLOCK F & O BLOCK B & K & O & F 20:00 - 22:30 BLOCK J BLOCK J & R BLOCK E & N & J & R BLOCK G BLOCK G & P BLOCK C & L & G & P WEDNESDAY THURDAYS TIME Stage 1 Stage 2 Stage 3 Stage 1 Stage 2 Stage 3 04:00 - 06:30 BLOCK A BLOCK H 06:00 - 08:30 BLOCK B BLOCK B & K BLOCK B & K & O & F BLOCK J BLOCK J & R BLOCK E & N & J & R 08:00 - 10:30 BLOCK C BLOCK C & L BLOCK C & L & G & P BLOCK A BLOCK A & Q BLOCK D & M & A & Q 10:00 - 12:30 BLOCK D BLOCK D & M BLOCK D & M & H & Q BLOCK E BLOCK E & N BLOCK E & N & J & R 12:00 - 14:30 BLOCK E BLOCK E & N BLOCK E & N & J & R BLOCK D BLOCK D & M BLOCK D & M & A & Q 14:00 - 16:30 BLOCK F BLOCK F & O BLOCK B & K & O & F BLOCK B BLOCK B & K BLOCK B & K & O & F 16:00 - 18:30 BLOCK G BLOCK G & P BLOCK C & L & G & P BLOCK C BLOCK C & L BLOCK C & L & G & P 18:00 - 20:30