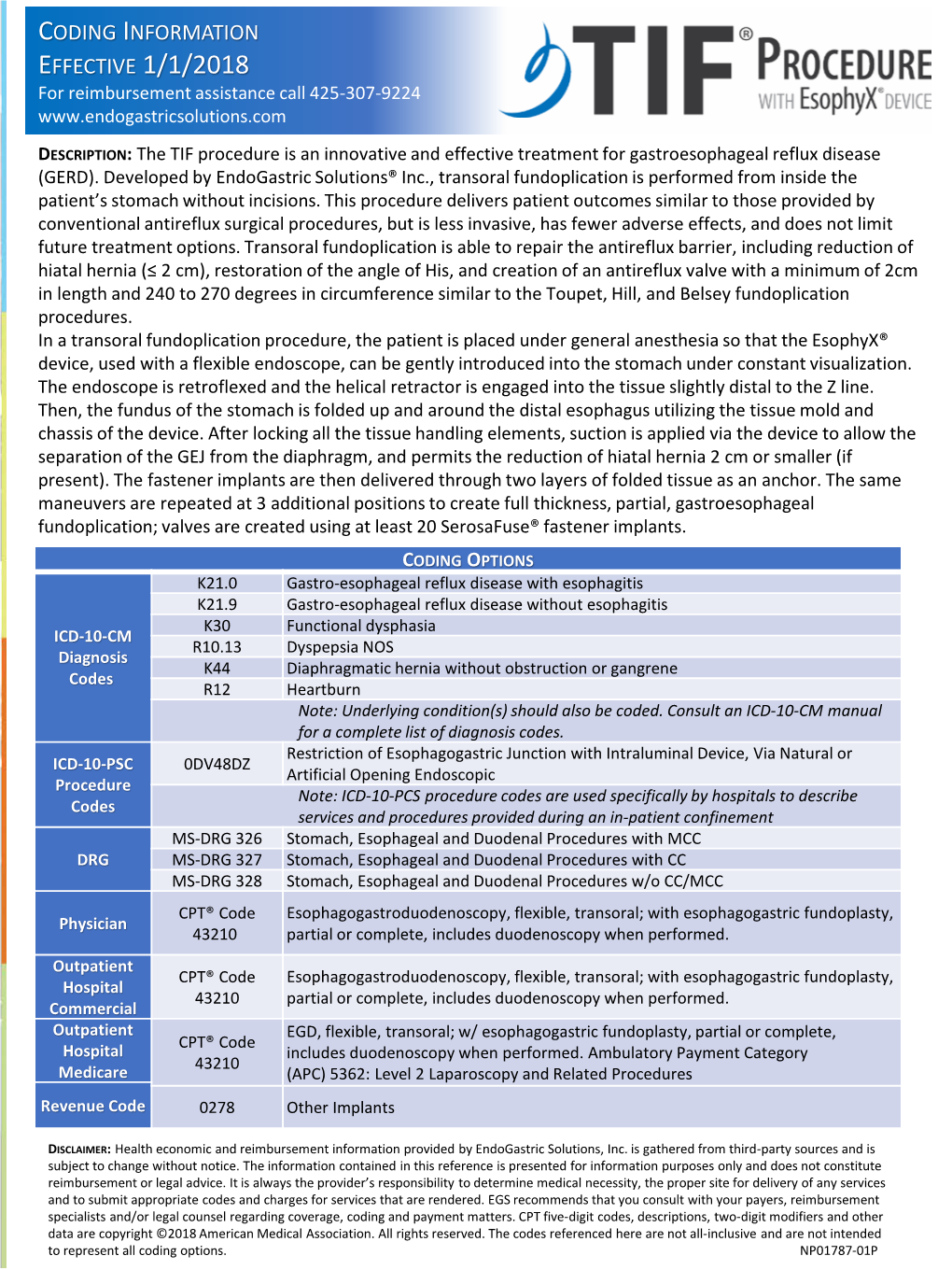
CODING INFORMATION EFFECTIVE 1/1/2018 for Reimbursement Assistance Call 425-307-9224
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

“A Dissertation on Endoscopic Biopsy Yield in Upper Gastrointestinal Malignancies” Dissertation Submitted To
“A DISSERTATION ON ENDOSCOPIC BIOPSY YIELD IN UPPER GASTROINTESTINAL MALIGNANCIES” DISSERTATION SUBMITTED TO THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY In partial fulfillment of the regulations for the award of the M.S.DEGREE EXAMINATION BRANCH I GENERAL SURGERY DEPARTMENT OF GENERAL SURGERY STANLEY MEDICAL COLLEGE AND HOSPITAL THE TAMILNADU DR.M.G.R MEDICAL UNIVERSITY CHENNAI APRIL 2015 CERTIFICATE This is to certify that the dissertation titled “A DISSERTATION ON ENDOSCOPIC BIOPSY YIELD IN UPPER GASTROINTESTINAL MALIGNANCIES” is the bonafide work done by Dr. P.ARAVIND, Post Graduate student (2012 – 2015) in the Department of General Surgery, Government Stanley Medical College and Hospital, Chennai under my direct guidance and supervision, in partial fulfillment of the regulations of The Tamil Nadu Dr. M.G.R Medical University, Chennai for the award of M.S., Degree (General Surgery) Branch - I, Examination to be held in April 2015. Prof.DR.C.BALAMURUGAN M.S Prof.DR.S.VISWANATHAN M.S Professor of Surgery Professor and Dept. of General Surgery, Head of the Department, Stanley Medical College, Dept. of General Surgery, Chennai-600001. Stanley Medical College, Chennai-600001. PROF. DR.AL.MEENAKSHISUNDARAM, M.D., D.A., The Dean, Stanley Medical College, Chennai - 600001. DECLARATION I, DR.P.ARAVIND solemnly declare that this dissertation titled “A DISSERTATION ON ENDOSCOPIC BIOPSY YIELD IN UPPER GASTROINTESTINAL MALIGNANCIES” is a bonafide work done by me in the Department of General Surgery, Government Stanley Medical College and Hospital, Chennai under the guidance and supervision of my unit chief. Prof. DR.C.BALAMURUGAN, Professor of Surgery. This dissertation is submitted to The Tamilnadu Dr.M.G.R. -

Abdominal Pain - Gastroesophageal Reflux Disease
ACS/ASE Medical Student Core Curriculum Abdominal Pain - Gastroesophageal Reflux Disease ABDOMINAL PAIN - GASTROESOPHAGEAL REFLUX DISEASE Epidemiology and Pathophysiology Gastroesophageal reflux disease (GERD) is one of the most commonly encountered benign foregut disorders. Approximately 20-40% of adults in the United States experience chronic GERD symptoms, and these rates are rising rapidly. GERD is the most common gastrointestinal-related disorder that is managed in outpatient primary care clinics. GERD is defined as a condition which develops when stomach contents reflux into the esophagus causing bothersome symptoms and/or complications. Mechanical failure of the antireflux mechanism is considered the cause of GERD. Mechanical failure can be secondary to functional defects of the lower esophageal sphincter or anatomic defects that result from a hiatal or paraesophageal hernia. These defects can include widening of the diaphragmatic hiatus, disturbance of the angle of His, loss of the gastroesophageal flap valve, displacement of lower esophageal sphincter into the chest, and/or failure of the phrenoesophageal membrane. Symptoms, however, can be accentuated by a variety of factors including dietary habits, eating behaviors, obesity, pregnancy, medications, delayed gastric emptying, altered esophageal mucosal resistance, and/or impaired esophageal clearance. Signs and Symptoms Typical GERD symptoms include heartburn, regurgitation, dysphagia, excessive eructation, and epigastric pain. Patients can also present with extra-esophageal symptoms including cough, hoarse voice, sore throat, and/or globus. GERD can present with a wide spectrum of disease severity ranging from mild, intermittent symptoms to severe, daily symptoms with associated esophageal and/or airway damage. For example, severe GERD can contribute to shortness of breath, worsening asthma, and/or recurrent aspiration pneumonia. -

Recent Insights Into the Biology of Barrett's Esophagus
Recent insights into the biology of Barrett’s esophagus Henry Badgery,1 Lynn Chong,1 Elhadi Iich,2 Qin Huang,3 Smitha Rose Georgy,4 David H. Wang,5 and Matthew Read1,6 1Department of Upper Gastrointestinal Surgery, St Vincent’s Hospital, Melbourne, Australia 2Cancer Biology and Surgical Oncology Laboratory, Peter MacCallum Cancer Centre, Melbourne, Australia 3Department of Pathology and Laboratory Medicine, Veterans Affairs Boston Healthcare System and Harvard Medical School, West Roxbury, Massachusetts 4Department of Anatomic Pathology, Faculty of Veterinary and Agricultural Sciences, The University of Melbourne, Melbourne, Australia 5Department of Hematology and Oncology, UT Southwestern Medical Centre and VA North Texas Health Care System, Dallas, Texas 6Department of Surgery, The University of Melbourne, St Vincent’s Hospital, Melbourne, Australia Address for correspondence: Dr Henry Badgery Department of Surgery St Vincent’s Hospital 41 Victoria Parade, Fitzroy, Vic, Australia, 3065 [email protected] Short title: Barrett’s biology This is the author manuscript accepted for publication and has undergone full peer review but has not been through the copyediting, typesetting, pagination and proofreading process, which may lead to differences between this version and the Version of Record. Please cite this article as doi: 10.1111/nyas.14432. This article is protected by copyright. All rights reserved. Keywords: Barrett’s esophagus; signaling pathways; esophageal adenocarcinoma; epithelial barrier function; molecular reprogramming Abstract Barrett’s esophagus (BE) is the only known precursor to esophageal adenocarcinoma (EAC), an aggressive cancer with a poor prognosis. Our understanding of the pathogenesis and of Barrett’s metaplasia is incomplete, and this has limited the development of new therapeutic targets and agents, risk stratification ability, and management strategies. -

Mechanisms Protecting Against Gastro-Oesophageal Reflux: a Review
Gut: first published as 10.1136/gut.3.1.1 on 1 March 1962. Downloaded from Gut, 1962, 3, 1 Mechanisms protecting against gastro-oesophageal reflux: a review MICHAEL ATKINSON From the Department of Medicine, University ofLeeds, The General Infirmary at Leeds Thomas Willis in his Pharmaceutice Rationalis pub- tion which function to close this orifice. During the lished in 1674-5 clearly recognized that the oeso- 288 years which have elapsed since this description, phagus may be closed off from the stomach and it has become abundantly clear that a closing described 'a very rare case of a certain man of mechanism does indeed exist at the cardia but its Oxford [who did] show an almost perpetual vomit- nature remains the subject of dispute. ing to be stirred up by the shutting up of left orifice Willis was chiefly concerned with the failure of this [of the stomach]'. His diagrams (Fig. 1) of the mechanism to open and does not appear to have anatomy of the normal stomach show a band of appreciated its true physiological importance. Al- muscle fibres encircling the oesophagogastric junc- though descriptions of oesophageal ulcer are to be found in the writings ofJohn Hunter and of Carswell (1838), the pathogenesis of these lesions remained uncertain until 1879, when Quincke described three cases with ulcers of the oesophagus resulting from digestion by gastric juice. Thereafter peptic ulcer of the oesophagus became accepted as a pathological entity closely resembling peptic ulcer in the stomach http://gut.bmj.com/ in macroscopic and microscopic appearances. The clinical picture of peptic ulcer of the oesophagus was clearly described by Tileston in 1906 who noted substernal pain radiating to between the shoulders, dysphagia, vomiting, haematemesis, and melaena as the principal presenting features. -

The Short Esophagus—Lengthening Techniques
10 Review Article Page 1 of 10 The short esophagus—lengthening techniques Reginald C. W. Bell, Katherine Freeman Institute of Esophageal and Reflux Surgery, Englewood, CO, USA Contributions: (I) Conception and design: RCW Bell; (II) Administrative support: RCW Bell; (III) Provision of the article study materials or patients: RCW Bell; (IV) Collection and assembly of data: RCW Bell; (V) Data analysis and interpretation: RCW Bell; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Reginald C. W. Bell. Institute of Esophageal and Reflux Surgery, 499 E Hampden Ave., Suite 400, Englewood, CO 80113, USA. Email: [email protected]. Abstract: Conditions resulting in esophageal damage and hiatal hernia may pull the esophagogastric junction up into the mediastinum. During surgery to treat gastroesophageal reflux or hiatal hernia, routine mobilization of the esophagus may not bring the esophagogastric junction sufficiently below the diaphragm to provide adequate repair of the hernia or to enable adequate control of gastroesophageal reflux. This ‘short esophagus’ was first described in 1900, gained attention in the 1950 where various methods to treat it were developed, and remains a potential challenge for the contemporary foregut surgeon. Despite frequent discussion in current literature of the need to obtain ‘3 or more centimeters of intra-abdominal esophageal length’, the normal anatomy of the phrenoesophageal membrane, the manner in which length of the mobilized esophagus is measured, as well as the degree to which additional length is required by the bulk of an antireflux procedure are rarely discussed. Understanding of these issues as well as the extent to which esophageal shortening is due to factors such as congenital abnormality, transmural fibrosis, fibrosis limited to the esophageal adventitia, and mediastinal fixation are needed to apply precise surgical technique. -

1 the Anatomy and Physiology of the Oesophagus
111 2 3 1 4 5 6 The Anatomy and Physiology of 7 8 the Oesophagus 9 1011 Peter J. Lamb and S. Michael Griffin 1 2 3 4 5 6 7 8 911 2011 location deep within the thorax and abdomen, 1 Aims a close anatomical relationship to major struc- 2 tures throughout its course and a marginal 3 ● To develop an understanding of the blood supply, the surgical exposure, resection 4 surgical anatomy of the oesophagus. and reconstruction of the oesophagus are 5 ● To establish the normal physiology and complex. Despite advances in perioperative 6 control of swallowing. care, oesophagectomy is still associated with the 7 highest mortality of any routinely performed ● To determine the structure and function 8 elective surgical procedure [1]. of the antireflux barrier. 9 In order to understand the pathophysiol- 3011 ● To evaluate the effect of surgery on the ogy of oesophageal disease and the rationale 1 function of the oesophagus. for its medical and surgical management a 2 basic knowledge of oesophageal anatomy and 3 physiology is essential. The embryological 4 Introduction development of the oesophagus, its anatomical 5 structure and relationships, the physiology of 6 The oesophagus is a muscular tube connecting its major functions and the effect that surgery 7 the pharynx to the stomach and measuring has on them will all be considered in this 8 25–30 cm in the adult. Its primary function is as chapter. 9 a conduit for the passage of swallowed food and 4011 fluid, which it propels by antegrade peristaltic 1 contraction. It also serves to prevent the reflux Embryology 2 of gastric contents whilst allowing regurgita- 3 tion, vomiting and belching to take place. -

Endoscopic Techniques in Bariatric Patients: Obesity Basics and Normal Postbariatric Surgery Anatomy Dan E
Techniques in Gastrointestinal Endoscopy (2010) 12, 124-129 Techniques in GASTROINTESTINAL ENDOSCOPY www.techgiendoscopy.com Endoscopic techniques in bariatric patients: Obesity basics and normal postbariatric surgery anatomy Dan E. Azagury, MD, David B. Lautz, MD Brigham and Women’s Hospital and Harvard Medical School, Department of Surgery, Boston, Massachusetts. KEYWORDS With the sharp rise in the number of bariatric surgical procedures over the past 15 y, the number and Gastric bypass; array of complications have also risen. Many of these complications are now either diagnosed or Vertical banded managed endoscopically. However, the rising diversity of surgical options requires endoscopists to gastroplasty; have a good working knowledge of normal postoperative anatomy for each procedure. This article Laparoscopic gastric reviews basic obesity epidemiology and describes postsurgical anatomy of the upper gastrointestinal banding; tract, separating the procedures into those with normal small bowel anatomy (restrictive procedures) Biliopancreatic diversion; and procedures resulting in small bowel modifications (procedures with a “malabsorptive” component). Laparoscopic sleeve © 2010 Elsevier Inc. All rights reserved. gastrectomy Many classifications have been used to measure and million potential candidates qualifying for a bariatric surgi- define obesity, of which body mass index (BMI) is the most cal procedure. The often dramatic results of this surgery widely used. BMI is calculated by dividing weight in kilo- have lead to a sharp rise in the interest and number of grams by the square of height in meters. Normal weight bariatric surgical procedures performed over the past 15 y. ranges from 18.5 to 24.9 kg/m2. A BMI between 25 and The number of bariatric procedures performed in the United 29.9 kg/m2 is defined as overweight and an individual is States and Canada was 14,000 in 1998,6 compared with an obese when his or her BMI is Ն30 kg/m2. -

Gastroesophageal Reflux: Anatomy and Physiology
26th Annual Scientific Conference | May 1-4, 2017 | Hollywood, FL Gastroesophageal Reflux: Anatomy and Physiology Amy Lowery Carroll, MSN, RN, CPNP- AC, CPEN Children’s of Mississippi at The University of Mississippi Medical Center Jackson, Mississippi Disclosure Information I have no disclosures. Objectives • Review embryologic development of GI system • Review normal anatomy and physiology of esophagus and stomach • Review pathophysiology of Gastroesophageal Reflux 1 26th Annual Scientific Conference | May 1-4, 2017 | Hollywood, FL Embryology of the Gastrointestinal System GI and Respiratory systems are derived from the endoderm after cephalocaudal and lateral folding of the yolk sack of the embryo Primitive gut can be divided into 3 sections: Foregut Extends from oropharynx to the liver outgrowth Thyroid, esophagus, respiratory epithelium, stomach liver, biliary tree, pancreas, and proximal portion of duodenum Midgut Liver outgrowth to the transverse colon Develops into the small intestine and proximal colon Hindgut Extends from transverse colon to the cloacal membrane and forms the remainder of the colon and rectum Forms the urogenital tract Embryology of the Gastrointestinal System Respiratory epithelium appears as a bud of the esophagus around 4th week of gestation Tracheoesophageal septum develops to separate the foregut into ventral tracheal epithelium and dorsal esophageal epithelium Esophagus starts out short and lengthens to final extent by 7 weeks Anatomy and Physiology of GI System Upper GI Tract Mouth Pharynx Esophagus Stomach -

Control at the Cardia Richard K
POSTGRAD. MED. J.. (1966), 42, 301 CONTROL AT THE CARDIA RICHARD K. GREENWOOD, M.D., M.Chir., F.R.C.S. Surgical Tutor *St. Thomas' Hospital Medical School, London, S.E.1. DESPITE many recent advances, a thorough DIAPHRAGM understanding of the physiological action of the ilower segment of Ithe oesophagus is still incomplete. The precise location of the gastro- MUCOSAL JUNCIONI esophageal junction requires definition. Clearly CARDIAC ORIFICE it is where oesophagus terminates and stomach commences. Unfortunately there is no unanimity of opinion on this matter. Barrett (1958) defines LOOP OF WILLI the oesophagus as the tubular structure inter- - % posed between the ph'arynx and ,bag of the stomach, receiving its blood supply from the aorta rather than ,the left gastric artery and having no peritoneal covering. This places the FIG. l.-Anatomy of the gastroesophageal junction. gastroesophageal junction at the level of the incisuria cardia where the fundus of the stomach commences (Ingelfinger 1958). The opening into phragmatic hiatus -to enter the abdomen. As the stomach is referred to as ,the cardiac orifice it does so it deviates -forwards and to the left. and the region immediately above it as the The oesophageal opening in the diaphragm is cardia. Earlier however Barrett (1950) had closed by the phreno-esophageal Imembrane. suggested that the mucosal junction offered a This is morphologically part of the transversailis convenient and distinct landmark between the fascia which 'lines the interior of the whole two organs. He and Palmer (1953) postulated abdominal cavity. It passes from the under- that anything lined with squamous epithelium surface of the diaphragm to the wall of the was oesophagus, and any structure with gastric oesophagus where it splits into ascending and glandular mucosa was stomach. -

Gastroesophageal Reflux Disease
Gastroesophageal Reflux Disease a,b, a,b Hayat Mousa, MD *, Maheen Hassan, MD KEYWORDS Gastroesophageal reflux Endoscopy Impedance Proton pump inhibitors Lifestyle changes Extraesophageal symptoms Pediatrics KEY POINTS Gastroesophageal reflux is a normal physiologic process that does not require treatment. In infants, reducing feeding volumes, offering smaller, more frequent meals, thickening feeds, and positioning can reduce reflux episodes; these infants should not be placed on acid suppression. Gastroesophageal reflux disease (GERD) occurs when reflux of gastric contents causes troublesome symptoms or complications. First-line treatment in children and adolescents includes lifestyle modification and acid suppression. GERD can have atypical presentations, such as recurrent pneumonia, upper airway symp- toms, nocturnal or difficult to control asthma, dental erosions, and Sandifer syndrome. Diagnosis of GERD is largely based upon history and physical, but endoscopy and pH impedance can be used to help support the diagnosis in atypical presentations. INTRODUCTION Gastroesophageal reflux (GER) is a normal physiologic process. It is defined as the involuntary flow of stomach content back into the esophagus.1 Most episodes of reflux are into the distal esophagus, brief, and asymptomatic. GER disease (GERD) occurs when reflux causes troublesome symptoms or complications.2 PHYSIOLOGY Multiple mechanisms are in place to protect from reflux: the antireflux barrier, esophageal clearance, and esophageal mucosal resistance. The antireflux barrier is composed of the lower esophageal sphincter (LES), the angle of His, the crural Disclosure Statement: The authors have no commercial or financial conflicts of interest or any funding sources to disclose. a University of California, San Diego, 3020 Children’s Way, MOB 211, MC 5030, San Diego, CA 92123, USA; b Division of Pediatric Gastroenterology, Hepatology, and Nutrition, Rady Chil- dren’s Hospital, 7960 Birmingham Way, Room 2110, MC 5030, San Diego, CA 92123, USA * Corresponding author. -

Gastroesophageal Reflux
S218 Jornal de Pediatria - Vol. 76, Supl.2, 2000 0021-7557/00/76-Supl.2/S218 Jornal de Pediatria Copyright© 2000 by Sociedade Brasileira de Pediatria REVIEW ARTICLE Gastroesophageal reflux Rocksane C. Norton1, Francisco J. Penna2 Abstract Objective: to discuss clinical, diagnostic and therapeutic aspects of gastroesophageal reflux. Method: we accomplished a literature review of the last 30 years, by means of Lilacs and Medline databases. Results: the gastroesophageal reflux is one of the most frequent causes of medical appointments with pediatric gastroenterologists. It represents a benign condition, characterized by regurgitations that can be resolved with general measures. Medical management with prokinetics and antacid agents controls clinical manifestations and prevents complications. Fundoplication is reserved to a minority of cases. Comments: some aspects of the clinical treatment have to be emphasized. Thickened/Solid diet and erect posture must be always recommended. Cisapride, the most commonly employed prokinetic agent, may prolong ventricular repolarization. Other prokinetic agents should be used in children. Bronchospasm or clinical manifestations of esophagitis indicate the use of antacid drugs. J Pediatr (Rio J) 2000; 76 (Supl.2): S218-224: gastroesophageal reflux, child. Introduction Gastroesophageal reflux (GER) can be defined as the not compromising the child’s growth and development. On retrograde and repetitive flux of gastric content for the the other hand, the pathological reflux presents clinical esophagus. It is frequent in children, and usually presents a repercussions, such as growth deficit, abdominal pain, benign evolution. It is characterized by the presence of irritability, digestive hemorrhages, bronchospasm, repeated regurgitations. Besides abdominal pain and intestinal pneumonia, or otorhinolaryngological complications, which constipation, it constitutes one of the main reasons of require capacity on the diagnosis and attention on the appointments with pediatric gastroenterologists. -
GIT: Esophagus-Stomach- Small Intestine
GIT: Esophagus-Stomach- Small Intestine MUDr. Azzat Al-Redouan Overview of the anatomical development Primitive gut- 4 Weeks Organs Derivatives Foregut → Esophagus ↘ Duodenum ↗ Midgut → Small Intestine ↘ Large Intestine ↗ Hindgut Organ Differentiation and Proliferation ➢ Endodermal inner epithelium → endothelial layer of mucosa, ducts and glands. ➢ Splanchnopleuric mesenchyme → lamina propria and muscularis, submucosa, external muscles and connective tissue. ➢ Splanchnopleuric coelomic epithelium → outer peritonial epithelium. ➢ Local population of angiogenic mesenchyme → blood vessels and lymphatics. ➢ Neural crest → enteric and autonomic nervous system. The sequential genetic expression basics Hedgehog (Hh) Ligands Mutational Endodermal epithelium Endothelial cells Knockout Shh Ihh Dhh • Esophageal atrasia Patch1 Receptors • Gut malformation Patch 2 • Defective muscularis propria • Enteric neurone anomalies • Imperforate anus Transcription Promote GIT Factor Gli3 differentiation Esophagus “Oesophagus” 25cm Muscular Tube C6 STARTS Th1 Connects from Pharynx ➢At the level of the inferior border Superior Mediastinum of the cricoid cartilage Th4 Inferior Mediastinum Connects to Stomach Th10 ➢At the gastric cardiac orifice. ENDS Th11 Inferior Thyroid a. Esophageal branches Esophageal branches Esophageal branches anastomoses Thoracic Aorta Thoracic Esophageal branches Ascending branches chain Vascular Inferior phrenic a. Left gastric a. Inferior thyroid v. Bronchial vv. vv. Plexus Plexus Azygous venous network esophagus - Submucous Intercostal vv. Esophageal Peri *A site of the porto-caval anastomoses Oesophageal Varcies Liver disease → ↑Portal resistance ↓ Porto-systemic shunting *A site of the porto-caval anastomoses (short gastric coronary vv ↔ esophageal vv.) Longitudinal continuous submucosal lymphatic system Cervical esophagus → Deep cervical nn. l. ↘ ↑ Paratrachial nn. l. ↗ Thoracic esophagus → posterior mediastinal nn. l. Abdominal esophagus → left gastric nn. l. * Some may pass directly → Thoracic duct ANS: Sympathetic trunk + Vagus n.