Neuropathy, Neuropathic Pain, and Painful Peripheral Neuropathy
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
SCIATICA Sciatica Describes Nerve Pain in the Leg That Is Caused by Irritation And/Or Compression of the Sciatic Nerve
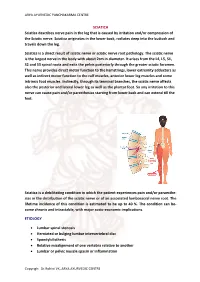
ARYA AYURVEDIC PANCHAKARMA CENTRE SCIATICA Sciatica describes nerve pain in the leg that is caused by irritation and/or compression of the Sciatic nerve. Sciatica originates in the lower back, radiates deep into the buttock and travels down the leg. Sciatica is a direct result of sciatic nerve or sciatic nerve root pathology. The sciatic nerve is the largest nerve in the body with about 2cm in diameter. It arises from the L4, L5, S1, S2 and S3 spinal roots and exits the pelvis posteriorly through the greater sciatic foramen. This nerve provides direct motor function to the hamstrings, lower extremity adductors as well as indirect motor function to the calf muscles, anterior lower leg muscles and some intrinsic foot muscles. Indirectly, through its terminal branches, the sciatic nerve affects also the posterior and lateral lower leg as well as the plantar foot. So any irritation to this nerve can cause pain and/or paresthesias starting from lower back and can extend till the feet. Sciatica is a debilitating condition in which the patient experiences pain and/or paraesthe- sias in the distribution of the sciatic nerve or of an associated lumbosacral nerve root. The lifetime incidence of this condition is estimated to be up to 40 %. The condition can be- come chronic and intractable, with major socio-economic implications. ETIOLOGY • Lumbar spinal stenosis • Herniated or bulging lumbar intervertebral disc • Spondylolisthesis • Relative misalignment of one vertebra relative to another • Lumbar or pelvic muscle spasm or inflammation Copyrigh: Dr.Rohini VK, ARYA AYURVEDIC CENTRE ARYA AYURVEDIC PANCHAKARMA CENTRE • Spinal or Paraspinal masses included malignancy, epidural haematoma or epidural abscess • Lumbar degenerative disc disease • Sacroiliac joint dysfunction EPIDEMIOLOGY GENDER: There appears to be no gender predominance. -

Radiculopathy Vs. Spinal Stenosis: Evocative Electrodiagnosis Identifies the Main Pain Generator
Functional Electromyography Loren M. Fishman · Allen N. Wilkins Functional Electromyography Provocative Maneuvers in Electrodiagnosis 123 Loren M. Fishman, MD Allen N. Wilkins, MD College of Physicians & Surgeons Manhattan Physical Medicine Columbia University and Rehabilitation New York, NY 10028, USA New York, NY 10013, USA [email protected] ISBN 978-1-60761-019-9 e-ISBN 978-1-60761-020-5 DOI 10.1007/978-1-60761-020-5 Springer New York Dordrecht Heidelberg London Library of Congress Control Number: 2010935087 © Springer Science+Business Media, LLC 2011 All rights reserved. This work may not be translated or copied in whole or in part without the written permission of the publisher (Springer Science+Business Media, LLC, 233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection with reviews or scholarly analysis. Use in connection with any form of information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed is forbidden. The use in this publication of trade names, trademarks, service marks, and similar terms, even if they are not identified as such, is not to be taken as an expression of opinion as to whether or not they are subject to proprietary rights. While the advice and information in this book are believed to be true and accurate at the date of going to press, neither the authors nor the editors nor the publisher can accept any legal responsibility for any errors or omissions that may be made. The publisher makes no warranty, express or implied, with respect to the material contained herein. -

Managing Post-Traumatic Trigeminal Neuropathic Pain: Is Surgery Enough? John R
Zuniga JR, Renton T. J Neurol Neuromedicine (2016) 1(7): 10-14 Neuromedicine www.jneurology.com www.jneurology.com Journal of Neurology & Neuromedicine Mini Review Open Access Managing post-traumatic trigeminal neuropathic pain: is surgery enough? John R. Zuniga1*, Tara F. Renton2 1Departments of Surgery and Neurology and Neurotherapeutics, The University of Texas Southwestern Medical Center at Dallas, Dallas, Texas, USA 2Department of Oral Surgery, Kings College London Dental Institute, Denmark Hill Campus, London SE5 9RS, UK ABSTRACT Article Info In the absence of effective non-surgical methods to permanently Article Notes resolve neuropathic pain involving the lip, chin, or tongue following inferior Received: September 19, 2016 alveolar and/or lingual nerve injury, microsurgery of these nerves has been a Accepted: October 08, 2016 recommended modality. In two ambispective clinical trials, we demonstrated Keywords: *Correspondence: that phenotypic differences exist between individuals with neuropathic Multiple sclerosis John R. Zuniga DMD, MS, PhD, Departments of Surgery and pain and those without neuropathic pain of the trigeminal nerve. In those Obesity Neurology and Neurotherapeutics, The University of Texas without neuropathic pain before microsurgery there was a 2% incidence of Body mass index Southwestern Medical Center at Dallas, Dallas, Texas, USA, Autoimmune disease neuropathic pain after microsurgery whereas there was a 67% incidence of Email: [email protected] Epidemiology neuropathic pain after microsurgery, some reporting an increase in pain levels, Susceptibility © 2016 Zuniga JR. This article is distributed under the terms of when neuropathic pain was present before microsurgery. The recurrence of the Creative Commons Attribution 4.0 International License neuropathic pain after trigeminal microsurgery is likely multifactorial and might not depend on factors that normally affect useful or functional sensory Keywords: recovery in those who have no neuropathic pain. -

Hereditary Hypertrophic Neuropathy Combining Features of Tic Douloureux, Charcot- Marie-Tooth Disease, and Deafness
Hereditary hypertrophic neuropathy combining features of tic douloureux, Charcot- Marie-Tooth disease, and deafness Hereditary hypertrophic sensorimotor poly- neuropathy combining the features of Charcot- Marie-Tooth disease, trigeminal neuralgia, and Robert P. Cruse, D.O. deafness occurred through four generations of John P. Conomy, M.D. a family originating in Haywood County, North Asa J. Wilbourn, M.D. Carolina. Fourteen individuals had pes cavus, Maurice R. Hanson, M.D. distal muscle atrophy, depressed or absent mus- cle stretch reflexes, cutaneous sensory deficits, Department of Neurology and defective proprioception. Six family mem- bers had recurrent, lancinating, trigeminal pain, and seven were deaf. The family was brought under scrutiny when the propositus, a 60-year-old woman, was examined for treat- ment of tic douloureux. Neurologic informa- tion was ultimately obtained regarding 52 family members. No history of consanguinity could be ascertained within this kinship. The genealogy of the family we studied is presented in Figure 1. In addition to clinical neurologic examinations, electromyographic and nerve conduction stud- ies were obtained on those individuals indicated in the genealogy diagram. Audiometric studies were obtained when there was clinical indication of defective hearing. Quantitative cutaneous sensory testing was obtained in the propositus. 107 Downloaded from www.ccjm.org on October 1, 2021. For personal use only. All other uses require permission. 108 Cleveland Clinic Quarterly Vol. 44, No. 3 ' • CMT a TIC Deaf CMT He Examined MS f Died O Not Affected 0 D led before age onset (O Multiple normal d1 ond j si be. -1—i Two Marriages —Indicates number of slbs. -

Scalp Dysesthesia. Case Report Disestesia Do Escalpo
BrJP. São Paulo, 2020 jan-mar;3(1):86-7 CASE REPORT Scalp dysesthesia. Case report Disestesia do escalpo. Relato de caso Letícia Arrais Rocha1, João Batista Santos Garcia1, Thiago Alves Rodrigues1 DOI 10.5935/2595-0118.20200016 ABSTRACT RESUMO BACKGROUND AND OBJECTIVES: Scalp dysesthesia is JUSTIFICATIVA E OBJETIVOS: A disestesia do escalpo ca- characterized by the presence of several localized or diffuse symp- racteriza-se pela presença de diversos sintomas localizados ou toms, such as burning, pain, pruritus or stinging sensations, wi- difusos, como queimação, dor, prurido ou sensações de picada, thout objective findings in the physical examination of the pa- sem achados objetivos no exame físico do paciente que possam tient that can explain and link the existing symptomatology to explicar e ligar os sintomas existentes à alguma outra etiologia. some other etiology. The aim of this study was to describe a case O objetivo deste estudo foi descrever um caso de disestesia de of scalp dysesthesia, from its clinical and laboratory investigation escalpo, desde a sua investigação clínica e laboratorial, até a con- and the conduct adopted. duta adotada. CASE REPORT: A 38-year-old male patient, first assigned to RELATO DO CASO: Paciente do sexo masculino, 38 anos. Pri- the Dermatology Service, with complaints of pruritus in the meiramente foi ao serviço de Dermatologia com queixa de pru- scalp for 5 years. In the consultation at the Pain Service, the pa- rido em couro cabeludo há cinco anos. Na consulta do Serviço tient complained of daily, intermittent and burning dysesthetic de Dor, o paciente queixava-se de sensações disestésicas como: sensations, such as tingling and pruritus in the bipariethoccipital formigamento e prurido em região biparieto-occipital que piora region, worsening with heat and associated with severe pain in com o calor, associada à dor de forte intensidade, diária, intermi- the cervical region. -

Neuropathy, Radiculopathy & Myelopathy
Neuropathy, Radiculopathy & Myelopathy Jean D. Francois, MD Neurology & Neurophysiology Purpose and Objectives PURPOSE Avoid Confusing Certain Key Neurologic Concepts OBJECTIVES • Objective 1: Define & Identify certain types of Neuropathies • Objective 2: Define & Identify Radiculopathy & its causes • Objective 3: Define & Identify Myelopathy FINANCIAL NONE DISCLOSURE Basics What is Neuropathy? • The term 'neuropathy' is used to describe a problem with the nerves, usually the 'peripheral nerves' as opposed to the 'central nervous system' (the brain and spinal cord). It refers to Peripheral neuropathy • It covers a wide area and many nerves, but the problem it causes depends on the type of nerves that are affected: • Sensory nerves (the nerves that control sensation>skin) causing cause tingling, pain, numbness, or weakness in the feet and hands • Motor nerves (the nerves that allow power and movement>muscles) causing weakness in the feet and hands • Autonomic nerves (the nerves that control the systems of the body eg gut, bladder>internal organs) causing changes in the heart rate and blood pressure or sweating • It May produce Numbness, tingling,(loss of sensation) along with weakness. It can also cause pain. • It can affect a single nerve (mononeuropathy) or multiple nerves (polyneuropathy) Neuropathy • Symptoms usually start in the longest nerves in the body: Feet & later on the hands (“Stocking-glove” pattern) • Symptoms usually spread slowly and evenly up the legs and arms. Other body parts may also be affected. • Peripheral Neuropathy can affect people of any age. But mostly people over age 55 • CAUSES: Neuropathy has a variety of forms and causes. (an injury systemic illness, an infection, an inherited disorder) some of the causes are still unknown. -

Sciatica and Chronic Pain
Sciatica and Chronic Pain Past, Present and Future Robert W. Baloh 123 Sciatica and Chronic Pain Robert W. Baloh Sciatica and Chronic Pain Past, Present and Future Robert W. Baloh, MD Department of Neurology University of California, Los Angeles Los Angeles, CA, USA ISBN 978-3-319-93903-2 ISBN 978-3-319-93904-9 (eBook) https://doi.org/10.1007/978-3-319-93904-9 Library of Congress Control Number: 2018952076 © Springer International Publishing AG, part of Springer Nature 2019 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifically the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfilms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specific statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors, and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made. The publisher remains neutral with regard to jurisdictional claims in published maps and institutional affiliations. -

Hereditary Spastic Paraparesis: a Review of New Developments
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.69.2.150 on 1 August 2000. Downloaded from 150 J Neurol Neurosurg Psychiatry 2000;69:150–160 REVIEW Hereditary spastic paraparesis: a review of new developments CJ McDermott, K White, K Bushby, PJ Shaw Hereditary spastic paraparesis (HSP) or the reditary spastic paraparesis will no doubt Strümpell-Lorrain syndrome is the name given provide a more useful and relevant classifi- to a heterogeneous group of inherited disorders cation. in which the main clinical feature is progressive lower limb spasticity. Before the advent of Epidemiology molecular genetic studies into these disorders, The prevalence of HSP varies in diVerent several classifications had been proposed, studies. Such variation is probably due to a based on the mode of inheritance, the age of combination of diVering diagnostic criteria, onset of symptoms, and the presence or other- variable epidemiological methodology, and wise of additional clinical features. Families geographical factors. Some studies in which with autosomal dominant, autosomal recessive, similar criteria and methods were employed and X-linked inheritance have been described. found the prevalance of HSP/100 000 to be 2.7 in Molise Italy, 4.3 in Valle d’Aosta Italy, and 10–12 Historical aspects 2.0 in Portugal. These studies employed the In 1880 Strümpell published what is consid- diagnostic criteria suggested by Harding and ered to be the first clear description of HSP.He utilised all health institutions and various reported a family in which two brothers were health care professionals in ascertaining cases aVected by spastic paraplegia. The father was from the specific region. -

Pain and Dysesthesia in Patients with Spinal Cord Injury: a Postal Survey
Spinal Cord (2001) 39, 256 ± 262 ã 2001 International Medical Society of Paraplegia All rights reserved 1362 ± 4393/01 $15.00 www.nature.com/sc Original Article Pain and dysesthesia in patients with spinal cord injury: A postal survey NB Finnerup*,1, IL Johannesen2, SH Sindrup3, FW Bach1 and TS Jensen1 1Department of Neurology and Danish Pain Research Centre, University Hospital of Aarhus, Denmark; 2Department of Rheumatology, Viborg Hospital, Denmark; 3Department of Neurology, Odense University Hospital, Denmark Study design: A postal survey. Objectives: To assess the prevalence and characteristics of pain and dysesthesia in a community based sample of patients with spinal cord injury (SCI) with special focus on neuropathic pain. Setting: Community. Western half of Denmark. Methods: We mailed a questionnaire to all outpatients (n=436) of the Viborg rehabilitation centre for spinal cord injury. The questionnaire contained questions regarding cause and level of spinal injury and amount of sensory and motor function below this level. The words pain and unpleasant sensations were used to describe pain (P) and dysesthesia (D) respectively. Questions included location and intensity of chronic pain or dysesthesia, degree of interference with daily activity and sleep, presence of paroxysms and evoked pain or dysesthesia, temporal aspects, alleviating and aggravating factors, McGill Pain Questionnaire (MPQ) and treatment. Results: Seventy-six per cent of the patients returned the questionnaire, (230 males and 100 females). The ages ranged from 19 to 80 years (median 42.6 years) and time since spinal injury ranged from 0.5 to 39 years (median 9.3 years). The majority (475%) of patients had traumatic spinal cord injury. -

Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies
17_Lupski 3/30/06 1:47 PM Page 243 NeuroMolecular Medicine Copyright © 2006 Humana Press Inc. All rights of any nature whatsoever reserved. ISSN0895-8696/06/08:243–254/$30.00 doi: 10.1385/NMM:8:1:243 REVIEW ARTICLE Molecular Diagnostics of Charcot-Marie-Tooth Disease and Related Peripheral Neuropathies Kinga Szigeti,1 Eva Nelis,2,3 and James R. Lupski*,1,4 1Departments of Molecular and Human Genetics, Baylor College of Medicine, Houston, TX; 2Molecular Genetics, Flanders Interuniversity Institute for Biotechnology, Institute Born-Bunge, University of Antwerp, Antwerpen, Belgium; 3Laboratory of Neurogenetics, Institute Born-Borge, University of Antwerp, Antwerpen, Belgium; and 4Pediatrics, Baylor College of Medicine, and Texas Children Hospital, Houston, TX 77030 Received January 10, 2006; Revised January 13, 2006; Accepted January 13, 2006 Abstract DNAdiagnostics plays an important role in the characterization and management of patients manifesting inherited peripheral neuropathies. We describe the clinical integration of molecular diagnostics with medical history, physical examination, and electrophysiological studies. Mole- cular testing can help establish a secure diagnosis, enable genetic counseling regarding recurrence risk, potentially provide prognostic information, and in the near future may be important for the choice of therapies. doi: 10.1385/NMM:8:1:243 Index Entries:Molecular diagnostics; Charcot-Marie-Tooth disease; CMT; hereditary neuropathy with liability to pressure palsies; HNPP; Dejerine-Sottas neuropathy; DSN; congenital hypomyelinating neuropathy; CHN; CMT1A duplication; HNPP deletion. Introduction genetic testing, one needs to be familiar with the diagnostic tests available, choose the appropriate Molecular genetic diagnosis has become an inte- patients for testing, and utilize the diagnostic tools gral part of the evaluation of patients with hered- in a logical fashion to optimize the use of resources. -

Chemotherapy-Induced Neuropathy and Diabetes: a Scoping Review
Review Chemotherapy-Induced Neuropathy and Diabetes: A Scoping Review Mar Sempere-Bigorra 1,2 , Iván Julián-Rochina 1,2 and Omar Cauli 1,2,* 1 Department of Nursing, University of Valencia, 46010 Valencia, Spain; [email protected] (M.S.-B.); [email protected] (I.J.-R.) 2 Frailty Research Organized Group (FROG), University of Valencia, 46010 Valencia, Spain * Correspondence: [email protected] Abstract: Although cancer and diabetes are common diseases, the relationship between diabetes, neuropathy and the risk of developing peripheral sensory neuropathy while or after receiving chemotherapy is uncertain. In this review, we highlight the effects of chemotherapy on the onset or progression of neuropathy in diabetic patients. We searched the literature in Medline and Scopus, covering all entries until 31 January 2021. The inclusion and exclusion criteria were: (1) original article (2) full text published in English or Spanish; (3) neuropathy was specifically assessed (4) the authors separately analyzed the outcomes in diabetic patients. A total of 259 papers were retrieved. Finally, eight articles fulfilled the criteria, and four more articles were retrieved from the references of the selected articles. The analysis of the studies covered the information about neuropathy recorded in 768 cancer patients with diabetes and 5247 control cases (non-diabetic patients). The drugs investigated are chemotherapy drugs with high potential to induce neuropathy, such as platinum derivatives and taxanes, which are currently the mainstay of treatment of various cancers. The predisposing effect of co-morbid diabetes on chemotherapy-induced peripheral neuropathy depends on the type of symptoms and drug used, but manifest at any drug regimen dosage, although greater neuropathic signs are also observed at higher dosages in diabetic patients. -

Dr Peter Heppner Consultant Neurosurgeon Auckland City Hospital Starship Childrens Hospital Ascot Hospital
Dr Peter Heppner Consultant Neurosurgeon Auckland City Hospital Starship Childrens Hospital Ascot Hospital 14:00 - 14:55 WS #55: Case Studies on Managing Cervical Radiculopathy 15:05 - 16:00 WS #67: Case Studies on Managing Cervical Radiculopathy (Repeated) Case Studies on Managing Cervical Radiculopathy: Peter Heppner Neurosurgeon Auckland City Hospital Starship Childrens Hospital Ascot Private Hospital www.neurosurgeon.org.nz DISCLOSURES I have no actual or potential conflict of interest in relation to this presentation WHAT ARE THE TAKE HOME POINTS? Evidence relating to cervical radiculopathy management is poor Natural history is generally very good In the absence of red flags, initial management with analgesia and physiotherapy appropriate NRIs can be a useful therapeutic and diagnostic tool Surgery ideally considered between 3-6 months from onset Either anterior or posterior surgical approaches can be selected depending on specifics of the case CASE 1 58 yr old lady 2 weeks radiating left arm pain (?after pilates) Taking paracetamol and NSAID Mild parasthesia in thumb Neuro exam normal Neck Disability Index 28% (mild) Clinically: Mild C6 radiculopathy of short duration CERVICAL RADICULOPATHY Radiating arm pain in a nerve distribution due to mechanical compression/chemical irritation of the nerve root Referred pain to inter-scapular and lateral neck common Weakness usually mild Pain or parasthesia non-dermatomal in almost half of patients Reduced reflex best predictor of imaging findings>motor weakness>sensory