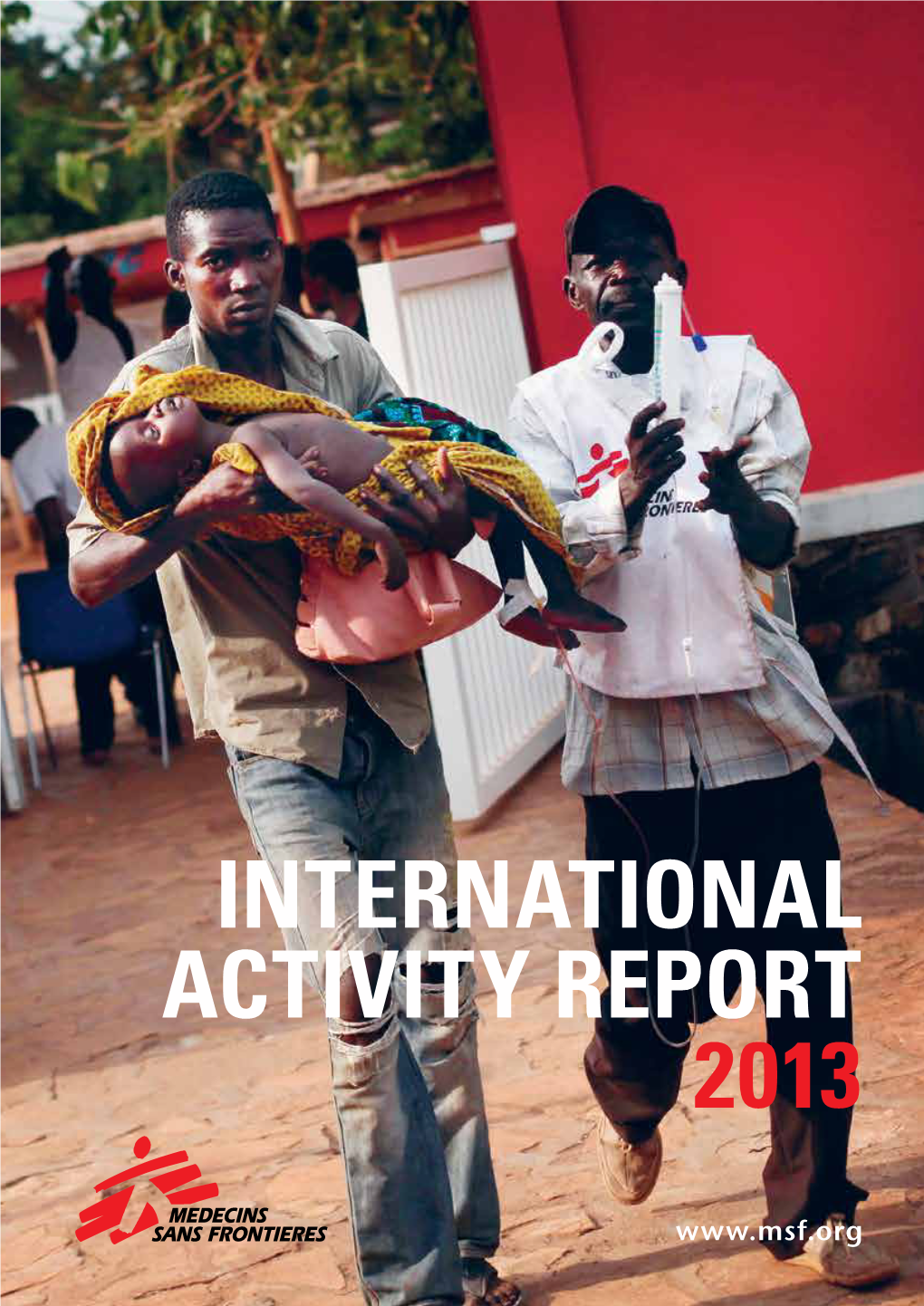
Msf.Org the Médecins Sans Frontières Charter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Photojournalism
ASSOCIATION VISA POUR L’IMAGE - PERPIGNAN Couvent des Minimes, 24, rue Rabelais - 66000 Perpignan tel: +33 (0)4 68 62 38 00 e-mail: [email protected] - www.visapourlimage.com FB Visa pour l’Image - Perpignan @visapourlimage PRESIDENT RENAUD DONNEDIEU DE VABRES rd VICE-PRESIDENT/TREASURER PIERRE BRANLE AUGUST 28 TO SEPTEMBER 26, 2021 COORDINATION ARNAUD FELICI & JÉRÉMY TABARDIN ASSISTANTS (COORDINATION) CHRISTOPHER NOU & NATHAN NOELL PRESS/PUBLIC RELATIONS 2e BUREAU 18, rue Portefoin - 75003 Paris INTERNATIONAL FESTIVAL OF tel: +33 (0)1 42 33 93 18 e-mail: [email protected] 33 www.2e-bureau.com Instagram & Twitter@2ebureau DIRECTOR GENERAL, COORDINATION SYLVIE GRUMBACH MANAGEMENT/ACCREDITATIONS VALÉRIE BOURGOIS PRESS RELATIONS MARTIAL HOBENICHE, DANIELA JACQUET ANNA ROUFFIA PHOTOJOURNALISM FESTIVAL MANAGEMENT Program subject to change due to Covid-19 health restrictions IMAGES EVIDENCE 4, rue Chapon - Bâtiment B - 75003 Paris tel: +33 (0)1 44 78 66 80 e-mail: [email protected] / [email protected] FB Jean Francois Leroy Twitter @jf_leroy Instagram @visapourlimage DIRECTOR GENERAL JEAN-FRANÇOIS LEROY EXECUTIVE DIRECTOR DELPHINE LELU COORDINATION CHRISTINE TERNEAU ASSISTANTJEANNE RIVAL SENIOR ADVISOR JEAN LELIÈVRE SENIOR ADVISOR – USA ELIANE LAFFONT SUPERINTENDENCE ALAIN TOURNAILLE TEXTS FOR SCREENINGS, PRESENTATIONS & RECORDED VOICE - FRENCH PAULINE CAZAUBON “MEET THE PHOTOGRAPHERS” MODERATOR CAROLINE LAURENT-SIMON BLOG & “MEET THE PHOTOGRAPHERS” CO-MODERATOR VINCENT JOLLY PROOFREADING OF FRENCH TEXTS & -

A Film by BORIS LOJKINE NINA MEURISSE
UNITÉ DE PRODUCTION PRESENTS Piazza Grande NINA MEURISSE a film by BORIS LOJKINE with FIACRE BINDALA BRUNO TODESCHINI GRÉGOIRE COLIN Unité de Production presents NINA MEURISSE a film by BORIS LOJKINE with VENTES INTERNATIONALES FIACRE BINDALA BRUNO TODESCHINI GRÉGOIRE COLIN Pyramide International (+33) 1 42 96 02 20 [email protected] / [email protected] DISTRIBUTION FRANCE Pyramide Distribution Running time : 90 MN 01 42 96 01 01 32 rue de l’Echiquier, 75010 Paris RELATIONS PRESSE FRANCE Hassan Guerrar / Julie Braun 01 40 34 22 95 [email protected] Photos and Press Kit downloadable on www.pyramidefilms.com SYNOPSIS Camille, a young idealistic photojournalist, goes to the Central African Republic to cover the civil war that is brewing up. What she sees there will change her destiny forever. Jeune photojournaliste éprise d'idéal, Camille part en Centrafrique couvrir la guerre civile qui se prépare. Ce qu’elle voit là-bas changera son destin. the following days… but they could not stop the spiral international community was focusing on other of violence. Because while the French disarmed and conflicts, Camille searched a way to dig deeper. She confined the Séléka to their barracks, the Christian notably tried to establish contacts with the Anti- community, hungry for revenge, turned against the balaka, in the hope of telling their story from within. by Boris Lojkine ABOUT THE FEATURE Muslim community. In May, as she was travelling in the western part of the country, she met a young Anti-balaka chief, Rocka Camille Lepage photographed it all. Mokom, who agreed to let her come along while he The burst of violence, the tragedy, the madness, the patrolled the CAR border with Cameroon, in an area A PROPOS DU FILM killing frenzy, death. -

L'exode Des « Plumes Indomptées »
Trimestriel Hiver 2014 2 € www.rsf.org LA REVUE DE REPORTERS SANS FRONTIÈRES POUR LA LIBERTÉ DE L’informaTION - N°09 PRIX REPORTERS SANS FRONTIÈRES SANJUANA MARTINEZ : « RSF M’A SAUVÉ LA VIE PLUS d’UNE FOIS » ÉTHIOPIE L’ExODE DES « PLUMES INDOMPTÉES » EN VUES 1. BAYEUX OU L’HOMMAGE AUX JOURNALISTES DISPARUS Le secrétaire général Christophe Deloire a dévoilé le 9 octobre 2014 à Bayeux la stèle des 113 noms de journalistes tués entre avril 2013 et août 2014. Un hommage particulier a été rendu à six d’entre eux : James Foley, décapité le 19 août par le groupe État islamique ; Camille Lepage, victime d’une fusillade en mai en Centrafrique ; Anja Niedringhaus, photographe allemande tuée en avril en Afghanistan ; Sardar Ahmad, abattu en Afghanistan en mars avec sa femme et deux de ses enfants par un commando taliban ; Ghislaine Dupont et Claude Verlon, journalistes à RFI assassinés au Mali en novembre 2013. © AFP PHOTO / CHARLY TRIBALLEAU / CHARLY © AFP PHOTO 2. #FIGHTIMPUNITY À l’occasion du 2 novembre 2014, première édition de la « Journée internationale de la fin de l’impunité pour les crimes commis contre les journalistes », Reporters sans frontières a lancé une campagne internationale intitulée #FightImpunity afin de faire pression sur les autorités pour traduire en justice les responsables de crimes contre les journalistes. La campagne se décline à travers dix cas d’impunité – torture, disparitions, assassinats -, et pointe du doigt les manquements des systèmes judiciaires et policiers. Les internautes ont pu agir à titre personnel en s’adressant directement par message électronique ou tweet aux chefs d’État ou de gouvernement des pays concernés. -

Special Feature the Crisis in the Central African Republic
HPN Humanitarian Practice Network Managed by Humanitarian Humanitarian Policy Group Exchange Commissioned and published by the Humanitarian Practice Network at ODI Number 62 September 2014 Special feature The crisis in the Central African Republic HPN Humanitarian Humanitarian Practice Network Managed by Humanitarian Policy Group Exchange Number 62 September 2014 Contents Editorial The crisis in the Central African Republic 3 Central African Republic: fragile state, fragile response 5 Prioritising Protection of Civilians in peacekeeping in the Central African Republic 8 Safeguarding distinction in Central African Republic 12 Humanitarian evacuations in the Central African Republic 14 Supporting social cohesion in the Central African Republic 16 Promoting accountability in the Central African Republic response 19 Why not digital? Technology as an interagency tool in the Central African Republic 21 Supporting local media in the Central African Republic 24 Adapting to anarchy: the ICRC in the Central African Republic 26 Gender-based violence in the Central African Republic: IRC’s response 28 Needs assessments in the Central African Republic Practice and policy notes 32 Protection of civilians sites: a new type of displacement settlement? This edition of Humanitarian Exchange focuses on the crisis in the Central 34 Using social protection systems to implement African Republic (CAR), where spiralling violence has left thousands dead emergency cash transfers: the case of Lesotho and more than a million displaced. In her lead article, Enrica Picco highlights 37 Gaining acceptance: lessons from the slow and inadequate response to the crisis, and questions whether the engagement with armed groups in humanitarian system has the will and capacity to respond in such contexts. -
2014 NMUN BGG Template
ROME, ITALY NMUN • EUROPE 23 - 29 November 2014 ROME 2014 nmun.org/nmun_europe14.html SECURITY COUNCIL BACKGROUND GUIDE 2014 Written By: Cara Wagner, Director; Maria Antonietta Coppola, Assistant Director NATIONAL COLLEGIATE CONFERENCE associationTM Dear Delegates, Welcome to the 2014 National Model United Nations held in Rome, Italy (NMUN•Europe) and particularly to the United Nations Security Council. As part of the volunteer staff for NMUN•Europe, we are looking forward to facilitating your experience at the conference. The Director for this committee is Cara Wagner, and Maria Antonietta Coppola will serve as the Assistant Director. Cara holds a Master of Science in Global Studies and International Affairs from Northeastern University and a B.A. in International Affairs and Certificate in Peace and Conflict Studies from the University of Colorado at Boulder. Maria Antonietta holds a master’s degree with Honors in International Affairs and a bachelor’s degree in Political Science and International Affairs from Sapienza University of Rome. The topics under discussion for the Security Council are: I. Protection of Journalists in Armed Conflict II. Women Peace and Security: Sexual Violence in Conflict The Security Council is one of the principle bodies of the UN and the only body in the UN system whose decisions are legally binding. Charged with the maintenance of international peace and security, the Security Council’s reach extends to all corners of the world and affects the entirety of the global population. Simulating this committee at NMUN•Europe gives you the opportunity to engage with the world’s most pressing issues and the most complex topics in peace and security, and to work towards consensus to address them. -

33Rd International Festival of Photojournalism
33rd International Festival of Photojournalism preliminary SaveDate àthe retenir dates program FESTIVAL July 30, 2021 AUGUST 28 - SEPTEMBER 26 exhibitions PROFESSIONAL WEEK SCREENINGS evening screenings PORTFOLIO REVIEWS visa d’or, grants & awards AUGUST 30 - SEPTEMBER 4 meetings & events partners SCHOOL GROUPS SEPTEMBER 13-17 contacts + SEPTEMBER 20-24 ADDITIONAL WEEKENDS SEPTEMBER 18-19 + SEPTEMBER 25-26 Program subject to change due www.visapourlimage.com to Covid-19 health restrictions. #visapourlimage21 editorial We certainly missed the light of the projectors on the giant screen in Perpignan, but in September this year the lights should be on again for the evening shows at Campo Santo. Six programs will be screened featuring around one hundred of the best stories produced by photojournalists over the past year. The reports sent in from so many different countries provide clear proof that the world has not ground to a halt. While the pandemic has turned societies upside down, and now stands as the major worldwide event of the early 21st century, there have been other crises, as seen for example in Myanmar, Nagorno-Karabakh, Ethiopia and Colombia where Covid-19 has not stopped the relentless course of events and conflicts. As is always the case, photojournalists have been present there, providing invaluable reports on these chapters in history. Their work is of course the result of talent and dedication, but we must not overlook certain outlets in the printed press and agencies which, despite an increasingly difficult financial situation, both in France and other regions, have continued to secure a reliable supply of fact-checked reports by sending their own journalists into the field. -

The Safety of Journalists and the Danger of Impunity
CI-16/COUNCIL-30/4 Rev. PARIS, 7 October 2016 Original: English THE SAFETY OF JOURNALISTS AND THE DANGER OF IMPUNITY REPORT BY THE DIRECTOR-GENERAL TO THE INTERGOVERNMENTAL COUNCIL OF THE IPDC (THIRTIETH SESSION) INTRODUCTION This document is submitted to the Intergovernmental Council of the International Programme for the Development of Communication’s (IPDC) in accordance with its Decision on the Safety of Journalists and the Issue of Impunity adopted at its 26th session (27 March 2008) and renewed at subsequent sessions in 2010, 2012, and 2014. The latest Decision from 2014 reiterated “the continuing relevance of [previous] IPDC Decisions that request the Director-General of UNESCO to provide to the Intergovernmental Council of the IPDC, on a two-year basis at its biennial session, an analytical report on the Director- General’s condemnations of the killings of journalists, media workers and social media producers who are engaged in journalistic activities and who are killed or targeted in their line of duty”. The present report offers an overview of the killings of journalists condemned by the Director-General in 2014-2015 as well as providing an analysis of the killings condemned over the last 10 years, between 2006 and 2015. It presents an update on the status of investigations into these killings based on the information provided by Member States. Background information is also provided on the latest developments in the implementation of the UN Plan of Action on the Safety of Journalists and the Issue of Impunity and on UNESCO’s specific contribution to this process. Communication and Information Sector 2 Communication and Information Sector TABLE OF CONTENTS 1. -

Central African Republic Freedomhouse.Org
https://freedomhouse.org/report/freedom-world/2015/central-african-republic#.VS_QSAn5uh0.cleanprint Central African Republic freedomhouse.org The political landscape of the conflict-torn Central African Republic (CAR) took a potential step toward stability in January 2014 following the resignation of president and Muslim military leader Michel Djotodia and the election of interim president Catherine Samba-Panza. Samba-Panza has no affiliation to any of the rebel groups involved in the conflict. Political instability, violence, religious cleansing, and the massive internal displacement of more than one million people in the ongoing conflict between the largely Muslim Séléka forces responsible for the 2013 coup and Christian militias known as anti-Balaka, who include supporters of ousted president François Bozizé, continued to worsen the country’s humanitarian crisis. In February 2014, UN secretary-general Ban Ki-moon launched the UN Multidimensional Integrated Stabilization Mission in Central African Republic (MINUSCA), authorizing more than 11,000 UN troops to join the African-led peacekeeping forces already stationed in CAR since 2013. In July 2014, Séléka and anti-Balaka signed a cease-fire agreement, but implementation of the accord proved short-lived. Séléka military chief Joseph Zoundeiko ignored the cease-fire and called for a partition of the country along religious lines. In September 2014, the International Criminal Court (ICC) opened a probe into the CAR conflict, citing widespread incidences of rape, murder, forced displacement, persecution, and pillaging since 2012. According to the Associated Press, more than 5,000 people were killed from December 2013 to September 2014, and this is likely a vast underestimation due to the difficulty of collecting accurate data. -

Women War Reporters' Resistance and Silence In
WOMEN WAR REPORTERS’ RESISTANCE AND SILENCE IN THE FACE OF SEXISM AND SEXUAL VIOLENCE LINDA STEINER UNIVERSITY OF MARYLAND. PHILIP MERRILL COLLEGE OF JOURNALISM. COLLEGE PARK, MARYLAND 20742, EUA [email protected] RESUMO As mulheres começaram a fazer reportagens de guerra em meados do século XIX, cobrindo, entre outras guerras, as revoluções europeias e a Guerra Civil dos EUA. Com a Primeira e Segunda Guerras Mundiais e especialmente com a Guer- ra do Vietname, o número de mulheres repórteres de guerra aumentou ao longo do século XX. O seu número voltou mais recentemente a aumentar, quando muitas organizações noticiosas precisavam de jornalistas no Iraque, no Afeganistão e no Paquistão. No entanto, as reportagens de guerra permanecem amplamente consi- deradas como um campo dos homens. Continua a ser um campo altamente sexista. As jornalistas de guerra continuam a enfrentar condescendência, pseudo-protecio- nismo, desdém, comportamentos obscenos e hostilidade por parte dos seus patrões, rivais, militares e do público. São também sujeitas a violência sexual, embora sejam desencorajadas de queixar-se desses assaltos, para que possam continuar a traba- lhar. Esta investigação centra-se no sexismo e assédio sexual enfrentados por mu- lheres repórteres de guerra contemporâneas, com especial atenção a Lara Logan, cuja carreira demonstra muitas dessas altas tensões de género. PALAVRAS-chAVE Mulheres repórteres de guerra; sexismo; culpadas enquanto vítimas; violên- cia sexual ABSTRACT Women began reporting on war in the mid-nineteenth century, covering, among other wars, Europeans revolutions and the US Civil War. The numbers of women report- ing on war increased over the twentieth century with the First and Second World Wars and especially the Vietnam War. -

En Hommage À Camille Lepage, Une Jeune Journaliste Française Tuée Pendant Un Reportage En Centrafrique (Médias)
En hommage à Camille Lepage, une jeune journaliste française tuée pendant un reportage en Centrafrique (médias) ____________________________ Un prêtre catholique apporte des précisions sur les circonstances de l'assassinat de Camille Lepage Bangui le 14 mai Radio Sirriri et Kangbi-ndara - "Camille Lepage n'a pas été tuée à Galo comme le prétendent certaines agences de presse mais en pleine brousse". Telle est l'une des précisions apportées par un prêtre centrafricain officiant à Bouar sur les lieux et les circonstances de l'assassinat de la journaliste française Camille Lepage contrairement aux informations diffusées hier à ce sujet. "Camille Lepage était partie de Bangui via Berberati pour des reportages sur les antibalaka de la zone allant de Hamadagaza (sous-préfecture de Carnot) à Abba (Nana Mambéré). Le dimanche 11 mai, elle se rendait à Ngambia village situé à 135 Km de Abba pour la suite de son reportage escortée par des miliciens antibalaka. Camille se trouvait en position "fin de convoi" avec quatre antibalaka. Un groupe d’éléments de l’ex Séléka a ouvert le feu tuant Camille et les quatre antibalaka sur coup. Les ravisseurs ont emporté tout ce qui était appareils se et papiers par devers Camille et les quatre antibalaka. Les autres antibalaka ont rebroussé chemin, ont combattu durement avant de récupérer les corps sans vie de Camille Lepage et des quatre autres antibalaka, les prénommés Mokom, Sam, Blaise et Ali. Elle n'a pas été tuée sur le grand axe Galo – Baboua comme le prétendent certaines agences de presse mais en pleine brousse loin de Galo ", a publié le prêtre catholique, Toussaint Zoumaldé, sur sa page facebook après avoir passé toute la matinée de ce mercredi à la recherche des détails précis sur l'assassinat de la journaliste française Camille Lepage. -

Central African Republic
CENTRAL AFRICAN REPUBLIC: TIME FOR ACCOUNTABILITY Amnesty International is a global movement of more than 3 million supporters, members and activists in more than 150 countries and territories who campaign to end grave abuses of human rights. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and public donations. First published in 2014 by Amnesty International Ltd Peter Benenson House 1 Easton Street London WC1X 0DW United Kingdom © Amnesty International 2014 Index: AFR19/06/2014 Original language: English Printed by Amnesty International, International Secretariat, United Kingdom All rights reserved. This publication is copyright, but may be reproduced by any method without fee for advocacy, campaigning and teaching purposes, but not for resale. The copyright holders request that all such use be registered with them for impact assessment purposes. For copying in any other circumstances, or for reuse in other publications, or for translation or adaptation, prior written permission must be obtained from the publishers, and a fee may be payable. To request permission, or for any other inquiries, please contact [email protected] Cover photo : Body of a Muslim man killed by Anti-balaka fighters in the town of Boguera on 10 February 2014. © Amnesty International. amnesty.org CONTENTS Map of the Central African Republic.……………………………………………………………… 4 List of acronyms…...……………………………………………………………………………...… 5 INTRODUCTION ........................................................................................................... 6 Methodology ............................................................................................................. 8 1. CHALLENGES TO INVESTIGATE AND PROSECUTE CRIMES UNDER INTERNATIONAL LAW IN CAR........................................................................ -

USAID Fiscal Year 2013 Agency Financial Report
AGENCY FINANCIAL REPORT FISCAL YEAR 2013 A NEW MODEL FOR DEVELOPMENT ABOUT THIS REPORT he Reports Consolidation Act of 2000 autho- • Improper Payments Elimination and Recovery Act rizes federal agencies to consolidate various (IPERA) of 2010 – requires agencies to improve agency Treports in order to provide performance, efforts to reduce and recover improper payments; financial, and related information in a more meaningful and useful format. This report, along with the Annual • Improper Payments Elimination and Recovery Performance Report, satisfies the reporting requirements Improvement Act (IPERIA) of 2012 – requires federal of the following legislation: agencies to expand their efforts to identify, recover, and prevent improper payments. • Inspector General Act of 1978 [Amended] – requires information on management actions in response to Since FY 2007, the U.S. Agency for International the Office of Inspector General (OIG) audits; Development (USAID) has elected to continue the production of three separate reports in lieu of a • Federal Managers’ Financial Integrity Act (FMFIA) of consolidated Performance and Accountability 1982 – requires ongoing evaluations of, and reports Report (PAR). on, the adequacy of internal accounting systems and administrative controls, not just controls over financial • Agency Financial Report (AFR) – provides complete reporting but also controls over program areas; details on relevant financial results; • Chief Financial Officers (CFO) Act of 1990 – requires • Annual Performance Report (APR) – provides