Chapter 10 Head and Neck Trauma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tbi): Progress in Treating the Sig- Nature Wounds of the Current Conflicts
S. HRG. 111–866 OVERSIGHT HEARING ON TRAUMATIC BRAIN IN- JURY (TBI): PROGRESS IN TREATING THE SIG- NATURE WOUNDS OF THE CURRENT CONFLICTS HEARING BEFORE THE COMMITTEE ON VETERANS’ AFFAIRS UNITED STATES SENATE ONE HUNDRED ELEVENTH CONGRESS FIRST SESSION MAY 5, 2010 Printed for the use of the Committee on Veterans’ Affairs ( Available via the World Wide Web: http://www.access.gpo.gov/congress/senate U.S. GOVERNMENT PRINTING OFFICE 64–440 PDF WASHINGTON : 2011 For sale by the Superintendent of Documents, U.S. Government Printing Office Internet: bookstore.gpo.gov Phone: toll free (866) 512–1800; DC area (202) 512–1800 Fax: (202) 512–2104 Mail: Stop IDCC, Washington, DC 20402–0001 VerDate Nov 24 2008 12:21 Feb 28, 2011 Jkt 000000 PO 00000 Frm 00001 Fmt 5011 Sfmt 5011 H:\ACTIVE\050510.TXT SVETS PsN: PAULIN COMMITTEE ON VETERANS’ AFFAIRS DANIEL K. AKAKA, Hawaii, Chairman JOHN D. ROCKEFELLER IV, West Virginia RICHARD BURR, North Carolina, Ranking PATTY MURRAY, Washington Member BERNARD SANDERS, (I) Vermont LINDSEY O. GRAHAM, South Carolina SHERROD BROWN, Ohio JOHNNY ISAKSON, Georgia JIM WEBB, Virginia ROGER F. WICKER, Mississippi JON TESTER, Montana MIKE JOHANNS, Nebraska MARK BEGICH, Alaska SCOTT P. BROWN, Massachusetts ROLAND W. BURRIS, Illinois ARLEN SPECTER, Pennsylvania WILLIAM E. BREW, Staff Director LUPE WISSEL, Republican Staff Director (II) VerDate Nov 24 2008 12:21 Feb 28, 2011 Jkt 000000 PO 00000 Frm 00002 Fmt 5904 Sfmt 5904 H:\ACTIVE\050510.TXT SVETS PsN: PAULIN CONTENTS MAY 5, 2010 SENATORS Page Akaka, Hon. Daniel K., Chairman, U.S. Senator from Hawaii ........................... 1 Burr, Hon. -

Chapter 42 – Facial Trauma
CrackCast Show Notes – Facial Trauma– September 2016 www.canadiem.org/crackcast Chapter 42 – Facial Trauma Episode Overview: 1) Describe the anatomy of the bones, glands, and ducts of the face. At what ages do the sinuses appear? 2) List 5 types of facial fractures. 3) Describe the clinical presentation and associated radiographic findings of an orbital blowout fracture. 4) Describe an orbital tripod fracture and its management. 5) List the indications for antibiotics in a patient with facial trauma? 6) What is the importance of perioral electrical burns? 7) What are the indications for specialist repair of an eyelid laceration? 8) Describe the classification and management of dental fractures. a. What is the management of an avulsed tooth? b. What is a luxed tooth? How is it managed? c. What is an alveolar ridge fracture? 9) Describe the method for reducing a jaw dislocation? What is the usual direction of the dislocation? Rosen’s in Perspective mechanism of facial trauma varies significantly age highly associated with alcohol use o 49% of maxillofacial trauma was ETOH related in one study . Of these, 78% were related to violence and assaults, and 13% to motor vehicle collisions. other common mechanisms include falls, animal bites, sports, and flying debris. much more common in unprotected vehicle users such as ATVs and motorcycles o 32% of injured ATV riders will have facial injuries. facial injury in these patients correlates with injury severity score children < 17 years old, sports injuries are the largest source of facial injuries (20%) children < 6 years old most commonly suffer facial injuries from family pets such as dogs in young children the face is the most common location of trauma associated with abuse. -

Proceedings of Réanimation 2019, the French Intensive Care Society International Congress
Ann. Intensive Care 2019, 9(Suppl 1):40 https://doi.org/10.1186/s13613-018-0474-7 MEETING ABSTRACTS Open Access Proceedings of Réanimation 2019, the French Intensive Care Society International Congress France. 23–25 January 2019 Published: 29 March 2019 Oral communications Oral communications: Physiotherapists Conclusion: We found that peak expiratory was higher with than with- out collapsible tube. In vivo measurements in patients should be done COK‑1 to confrm this fnding. Bench assessment of the efect of a collapsible tube on the efcacy of a mechanical insufation‑exsufation device Romain Lachal (speaker) Réanimation médicale, Hôpital de la Croix‑Rousse, Hospices Civils de Lyon, Lyon, FRANCE Correspondence: Romain Lachal ‑ [email protected] Annals of Intensive Care 2019, 9(Suppl 1):COK-1 Introduction: Mechanical Insufation-Exsufation (MI-E) by using a specifc device is commonly used to increase weak cough, as in patients with chronic neuromuscular weakness or in intensive care unit (ICU) patients with ICU-acquired neuro-myopathy. The assess- ment of the efcacy of MI-E device is commonly done by measuring peak cough fow (PCF). Upper airways collapse is frequently associated with neuromuscular disease and may compromise MI-E efcacy. Tra- cheomalacia is another disease that may impede PCF to increase with MI-E device. The goal of present study was to carry out a bench study to assess the efect of MI-E on PCF with and without the presence of a collapsible tube. Our hypothesis was that PCF was lower with than without collapsible tube. COK‑2 Patients and methods: We used a lung simulator (TTL Michigan Early verticalization in neurologic intensive care units Instruments) with adjustable compliance (C) and resistance (R) to with a weight suspension system which a MI-E (CoughAssist E70, Philips-Respironics) was attached, Margrit Ascher (speaker), Francisco Miron Duran, Fanny Pradalier, Claire with or without a latex collapsible tube. -

Approach to the Trauma Patient Will Help Reduce Errors
The Approach To Trauma Author Credentials Written by: Nicholas E. Kman, MD, The Ohio State University Updated by: Creagh Boulger, MD, and Benjamin M. Ostro, MD, The Ohio State University Last Update: March 2019 Case Study “We have a motor vehicle accident 5 minutes out per EMS report.” 47-year-old male unrestrained driver ejected 15 feet from car arrives via EMS. Vital Signs: BP: 100/40, RR: 28, HR: 110. He was initially combative at the scene but now difficult to arouse. He does not open his eyes, withdrawals only to pain, and makes gurgling sounds. EMS placed a c-collar and backboard, but could not start an IV. What do you do? Objectives Upon completion of this self-study module, you should be able to: ● Describe a focused rapid assessment of the trauma patient using an organized primary and secondary survey. ● Discuss the components of the primary survey. ● Discuss possible pathology that can occur in each domain of the primary survey and recommend treatment/stabilization measures. ● Describe how to stabilize a trauma patient and prioritize resuscitative measures. ● Discuss the secondary survey with particular attention to head/central nervous system (CNS), cervical spine, chest, abdominal, and musculoskeletal trauma. ● Discuss appropriate labs and diagnostic testing in caring for a trauma patient. ● Describe appropriate disposition of a trauma patient. Introduction Nearly 10% of all deaths in the world are caused by injury. Trauma is the number one cause of death in persons 1-50 years of age and results in significant life years lost. According to the National Trauma Data Bank, falls were the leading cause of trauma followed by motor vehicle collisions (MVCs) and firearm related injuries with an overall mortality rate of 4.39% in 2016. -

Maxillofacial Trauma
Case Report 2019 iMedPub Journals International Journal of Anesthesiology & Pain Medicine www.imedpub.com ISSN 2471-982X Vol.5 No.1:3 DOI: 10.36648/2471-982X.5.1.27 Maxillofacial Trauma: Peri Operative Bulbulia BA*, Vally IM and Challenges in the Management of Facial Bone Vally U Ahmed Kathrada Private Hospital, Fractures Lenasia, South Africa *Corresponding author: Bulbulia BA Abstract Facial trauma and fractures of the facial bones may have associated brain and [email protected] cervical spine injuries. Assault, gunshot wounds and motor vehicle accidents (MVA) are major contributory causes. Trauma units must be competent in airway Ahmed Kathrada Private Hospital, Lenasia, management. Death may result from trauma itself, haemorrhage, aspiration or South Africa. hypoxia. Initial screening of neurological injury must be followed by neural imaging studies and neurological examination. Tel: 27834173527 Keywords: Facial bone fracture; Airway management; Cognitive assessment; High resolution brain scan; Definitive surgery delayed; Post-operative ventilation Citation: Bulbulia BA, Vally IM, Vally U Received: October 30, 2019; Accepted: October 30, 2019; Published: November 10, (2019) Maxillofacial Trauma: Peri Operative 2019 Challenges in the Management of Facial Bone Fractures. Int J Anesth Pain Med. Vol.5 Introduction No.1:3 Maxillofacial and neck trauma frequently present as emergencies. Sports related injuries, falls and industrial These injuries are daunting surgically and present unique accidents are other remaining causes challengers for anaesthesiologists. Airway management skills in head and neck trauma are essential as the anatomy may be The skeletal region of isolated facial bone fractures: red, frontal distorted and compromised by bleeding and aspiration of blood bone (0.4%); yellow, orbital bone (9.2%); green, nasal bone and vomitus into the lungs [1]. -

Acute Liver Failure in Adults: an Evidence- Based Management Protocol for Clinicians
Acute Liver Failure in Adults: An Evidence- Based Management Protocol for Clinicians Heather Patton, MD, Michael Misel, PharmD, and Robert G. Gish, MD Dr. Patton is an Assistant Clinical Abstract: With the goal of providing guidance on the provision Professor of Medicine in the Division of optimal intensive care to adult patients with acute liver fail- of Gastroenterology at the University ure (ALF), this paper defines ALF and describes a protocol for of California (UC) San Diego School of appropriately diagnosing this relatively rare clinical entity and Medicine; she is also affiliated with the ascertaining its etiology, where possible. This paper also identi- Center for Hepatobiliary Disease and fies the few known therapies that may be effective for specific Abdominal Transplantation (CHAT) in the UC San Diego Health System, both causes of ALF and provides a comprehensive approach for antici- in San Diego, California. Dr. Misel is an pating, identifying, and managing complications. Finally, one of Assistant Clinical Professor at the UC the more important aspects of care for patients with ALF is the San Diego Skaggs School of Pharmacy determination of prognosis and, specifically, the need for liver & Pharmaceutical Sciences; he is also a transplantation. Prognostic tools are provided to help guide the Pharmacist Specialist in Hepatobiliary clinician in this critical decision process. Management of patients Disease and Abdominal Transplant at CHAT in the UC San Diego Health with ALF is complex and challenging, even in centers where staff System. Dr. Gish is Chief of Clinical members have high levels of expertise and substantial experience. Hepatology and a Professor of Clinical This evidence-based protocol may, therefore, assist in the delivery Medicine in the Division of Gastroen- of optimal care to this critically ill patient population and may terology at the UC San Diego School of substantially increase the likelihood of positive outcomes. -
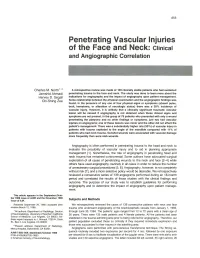
Penetrating Vascular Injuries of the Face and Neck: Clinical and Angiographic Correlation
855 Penetrating Vascular Injuries of the Face and Neck: Clinical and Angiographic Correlation Charles M. North 1. 2 A retrospective review was made of 139 clinically stable patients who had sustained Jamshid Ahmadi penetrating trauma to the face and neck. The study was done to learn more about the Hervey D. Segall indications for angiography and the impact of angiography upon patient management. Chi-Shing Zee Some relationship between the physical examination and the angiographic findings was found. In the presence of anyone of four physical signs or symptoms (absent pulse, bruit, hematoma, or alteration of neurologic status) there was a 30% incidence of vascular injury. However, it is unlikely that a clinically significant traumatic vascular lesion will be missed if angiography is not obtained when these clinical signs and symptoms are not present. In the group of 78 patients who presented with only a wound penetrating the ' platysma and no other findings or symptoms, just two had vascular injuries on angiograms; one of these lesions was minor and the other did not affect the patient's management. There was a substantially higher rate (50%) of vascular injury in patients with trauma cephalad to the angle of the mandible compared with 11 % of patients who had neck trauma. Gunshot wounds were associated with vascular damage more frequently than were stab wounds. Angiography is often performed in penetrating trauma to the head and neck to evaluate the possibility of vascular injury and to aid in planning appropriate management [1]. Nonetheless, the role of angiography in penetrating head and neck trauma has remained controversial. -

Real and Illusory Perceptions of Patients in Induced Coma
REVIEW Real and illusory perceptions of patients in induced coma Percepções reais e ilusórias de pacientes em coma induzido Percepciones reales e ilusorias de pacientes en coma inducido ABSTRACT Simone Costa SilvaI Objective: To identify, in the scientific literature, real and illusory perceptions of adult patients in induced coma. Methods: This is an integrative review of 15 primary studies from ORCID: 0000-0001-9220-6310 the Medline, Web of Science, LILACS, CINAHL and SCOPUS databases. Results: The main I memories reported after induced coma were thirst, cold, and pain. In some studies, patients Laura Menezes Silveira reported they were unable to tell whether they were awake or dreaming, whether it was ORCID: 0000-0002-2397-2553 real or unreal. Satisfactory memories were reported by patients related to the care received I and the use of bedside journals. Conclusion: Evidence showed a number of studies aiming Leila Maria Marchi-Alves to identify delirium, but without a focus on analyzing real or illusory perceptions of patients ORCID: 0000-0001-9374-8074 after induced coma. Thus, this integrative review identified scientific evidence of memories related to perceptions of sedated patients in the intensive care unit. I Isabel Amélia Costa Mendes Descriptors: Deep Sedation; Memory; Delirium; Critical Care; Nursing. ORCID: 0000-0002-0704-4319 I RESUMO Simone de Godoy Objetivo: Identificar, a partir da literatura científica, percepções reais e ilusórias de pacientes ORCID: 0000-0003-0020-7645 adultos em coma induzido. Método: Revisão integrativa de 15 estudos primários localizados nas bases de dados Medline, Web of Science, LILACS, CINAHL e SCOPUS. Resultados: As principais memórias relatadas após o coma induzido são sede, frio e dor. -
Basic Trauma Overview - ABC
Basic Trauma Overview - ABC Dale Dangleben, MD, FACS 1 2 Team 3 Extended Team 4 Team Leader Decrease chaos / optimize care. – Remains calm – Maintains control and provides direction – Stays decisive – Sees the big picture (situational awareness) – Is open to other team members input – Directs resuscitation – Makes early decision to transfer the patients that exceed the local capabilities 5 Team Members − Know your roles in the trauma team − Remain calm − Be responsive to team leader −Voice suggestions or concerns 6 Responsibilities – Perform the Primary and secondary survey – Verbalize patient care – Report completed tasks 7 Responsibilities – Monitors the patient – Manual BP – Obtains IV access – Administers medications – Dresses wounds – Performs or assists in resuscitative procedures 8 Responsibilities Records data Ensures documentation accompanies patient upon transfer Assists team members as needed 9 Responsibilities – Obtains needed supplies – Coordinates communication with local and external resources – Assists team members as needed 10 Responsibilities • Place Oxygen on patient • Manage airway • Hold C spine • Manage ventilator if • Manage rapid infuser line patient intubated where indicated • Assists team members as needed 11 Organization of trauma resuscitation area – Basic adult and pediatric equipment for: • Airway management (cart) • IV access with warm fluids • Chest tube insertion • Hemorrhage control (tourniquets, pelvic binders) • Immobilization • Medications • Pediatric length/weight based tape (Broselow Tape) – Warming -

Coma, Delirium, and Cognitive Dysfunction in Critical Illness Robert D
Crit Care Clin 22 (2007) 787–804 Coma, Delirium, and Cognitive Dysfunction in Critical Illness Robert D. Stevens, MD*, Paul A. Nyquist, MD, MPH Departments of Anesthesiology/Critical Care Medicine, Neurology, Neurological Surgery, Johns Hopkins University School of Medicine, 600 N Wolfe St, Baltimore, MD 21287, USA Syndromes of global cerebral dysfunction associated with critical illness include acute disorders such as coma and delirium, and chronic processes namely cognitive impairment. These syndromes can result from direct cere- bral injury, but in many instances develop as a complication of a systemic in- sult such as cardiac arrest, hypoxemia, sepsis, metabolic derangements, and pharmacological exposures. Coma frequently evolves into phenomenologi- cally distinct disorders of consciousness such as the vegetative state and the minimally conscious state, and it must be differentiated from conditions in which consciousness is preserved, as in the locked-in state. Coma and de- lirium are independently associated with increased short-term mortality, while cognitive impairment has been linked to the poor long term functional status and quality of life observed in critical illness survivors. Advances have been made in defining, scoring, and delineating the epidemiology of cerebral dysfunction in the intensive care unit, but research is needed to elucidate underlying mechanisms, with the goal of identifying targets for prevention and therapy. Acute brain dysfunction A high proportion of patients who are admitted to the ICU develops a global alteration in cognitive function that is associated with an underlying cerebral process that can be structural or metabolic [1,2]. Terms that are used commonly to describe these disturbances include coma, delirium, encephalop- athy, acute confusional state, organic brain syndrome, acute organic reaction, * Corresponding author. -

Types of Brain Dysfunction in Critical Illness Robert D
Neurol Clin 26 (2008) 469–486 Types of Brain Dysfunction in Critical Illness Robert D. Stevens, MD*, Paul A. Nyquist, MD, MPH Departments of Anesthesiology Critical Care Medicine, Neurology, and Neurological Surgery, Johns Hopkins University School of Medicine, Meyer 8-140, 600 North Wolfe Street, Baltimore, MD 21287, USA Many patients in the ICU develop a global alteration in cognitive func- tion that may be structural or metabolic in origin [1]. Terms used to describe these disturbances include delirium, acute confusional state, organic brain syndrome, acute organic reaction, cerebral insufficiency, brain failure, ICU psychosis, and encephalopathy. Etiology-specific terms, such as septic encephalopathy or hepatic encephalopathy, have been used when there is a strong presumption regarding the causative mechanism. It has been pos- tulated that many of these disorders are clinical expressions of a pathophys- iologic spectrum, collectively referred to as ‘‘critical illness brain syndrome’’ [2], ‘‘critical illness–associated cognitive dysfunction’’ [3], or ‘‘critical illness encephalopathy’’ [1]. Recently, there has been an effort to rationalize this terminology and to classify brain dysfunction in the ICU as either delirium or coma, using validated clinical criteria [4–7]. Coma Clinical assessment In the clinical realm consciousness is described in terms of two primary neurologic functions: arousal or wakefulness, and awareness of self and of the environment [8]. Awareness is the content of consciousness and includes multiple cognitive domains including perception, attention, memory, This is an updated version of an article that originally appeared in Critical Care Clinics, volume 22, issue 4. * Corresponding author. Division of Neurosciences Critical Care, Johns Hopkins University School of Medicine, Meyer 8-140, 600 North Wolfe Street, Baltimore, MD 21287. -

COVID-19 and the Impact on the Cranio-Oro-Facial Trauma Care in Italy: an Epidemiological Retrospective Cohort Study
International Journal of Environmental Research and Public Health Article COVID-19 and the Impact on the Cranio-Oro-Facial Trauma Care in Italy: An Epidemiological Retrospective Cohort Study Fausto Famà 1, Roberto Lo Giudice 1,* , Gaetano Di Vita 2, João Paulo Mendes Tribst 3 , Giorgio Lo Giudice 4 and Alessandro Sindoni 5,6 1 Department of Human Pathology in Adulthood and Childhood “G. Barresi”, University Hospital “G. Martino” of Messina, Via Consolare Valeria 1, 98123 Messina, Italy; [email protected] 2 Department of Surgical Oncological and Stomatological Sciences, University of Palermo, Piazza Marina 61, 90133 Palermo, Italy; [email protected] 3 Department of Dentistry, University of Tautabé (UNITAU), Taubaté 12030-040, Brazil; [email protected] 4 Maxillofacial Surgery Unit, Multidisciplinary Department of Medical-Surgical and Dental Specialities, University of Campania “Luigi Vanvitelli”, Viale Abramo Lincoln 5, 80138 Naples, Italy; [email protected] 5 Department of Public Health and Infectious Diseases, Sapienza University of Rome, Piazzale Aldo Moro 5, 00185 Rome, Italy; [email protected] 6 Direzione Sanitaria, Azienda Ospedaliero-Universitaria Policlinico Umberto I, 00161 Rome, Italy * Correspondence: [email protected]; Tel.: +39-393-439-9197 Abstract: The coronavirus disease 2019 (COVID-19) has deeply modified the organization of hospitals, health care centers, and the patient’s behavior. The aim of this epidemiological retrospective cohort study is to evaluate if and how the COVID-19 pandemic has determined a modification in cranio- oro-facial traumatology service. Methods: The dataset included hospital emergency room access of Citation: Famà, F.; Lo Giudice, R.; Di a six-month pre-pandemic period and six months into pandemic outbreak.