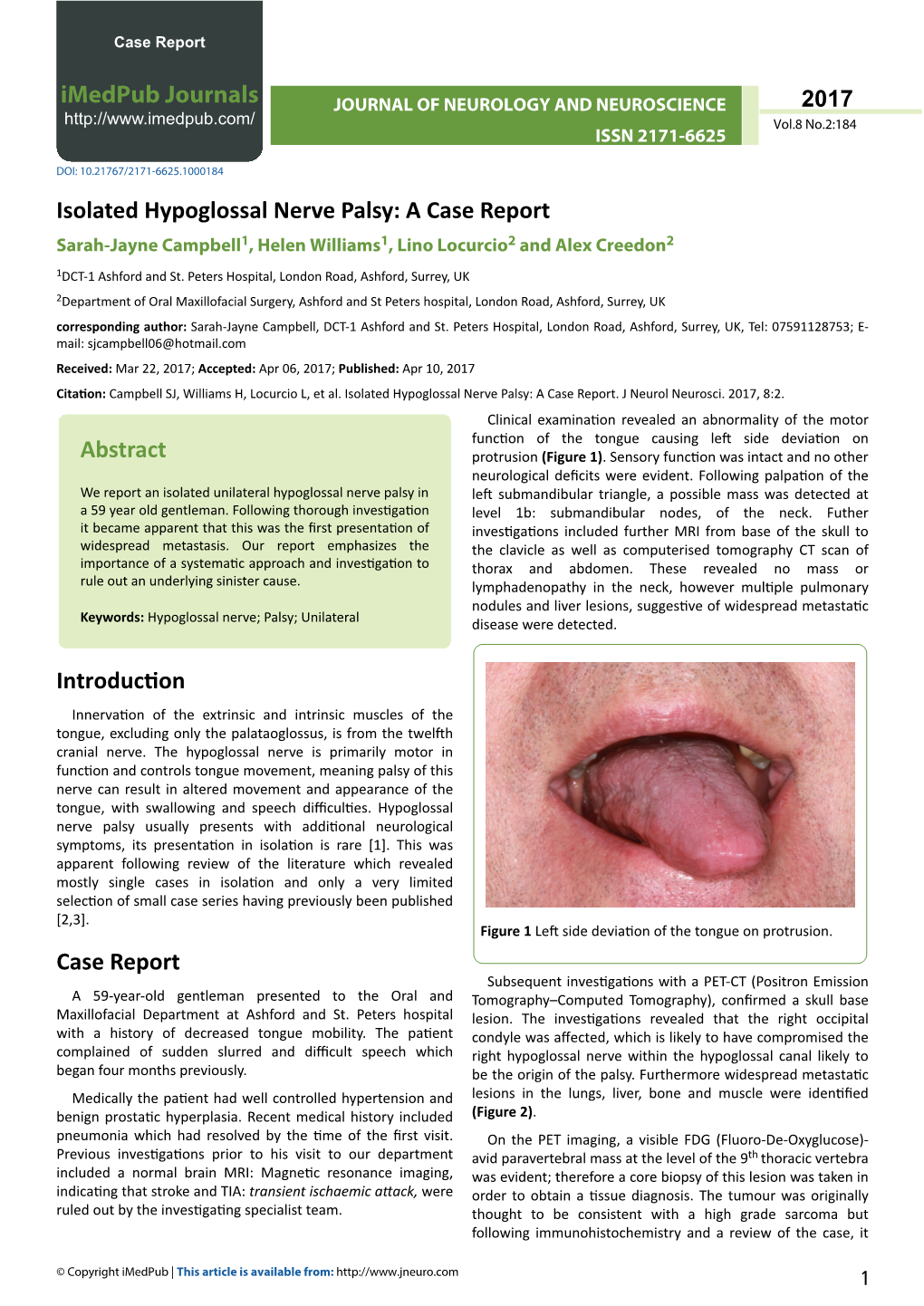
Isolated Hypoglossal Nerve Palsy: a Case Report Sarah-Jayne Campbell1, Helen Williams1, Lino Locurcio2 and Alex Creedon2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Rare Case of Collett–Sicard Syndrome After Blunt Head Trauma
Case Report Dysphagia and Tongue Deviation: A Rare Case of Collett–Sicard Syndrome after Blunt Head Trauma Eric Tamrazian 1,2 and Bijal Mehta 1,2,* 1 Department of Neurology, David Geffen School of Medicine, Harbor-UCLA Medical Center, Torrance, CA 90502, USA; [email protected] 2 Los Angeles Biomedical Institute, Los Angeles, CA 90095, USA * Correspondence: [email protected] Received: 28 October 2019; Accepted: 14 November 2019; Published: 21 December 2020 Abstract: The jugular foramen and the hypoglossal canal are both apertures located at the base of the skull. Multiple lower cranial nerve palsies tend to occur with injuries to these structures. The pattern of injuries tend to correlate with the combination of nerves damaged. Case Report: A 28-year-old male was involved in an AVP injury while crossing the highway. Exam showed a GCS of 15 AAOx3, with dysphagia, tongue deviation to the right, uvula deviation to the left and a depressed palate. Initial imaging showed B/L frontal traumatic Sub-Arachnoid Hemorrhages (tSAH), Left Frontal Epidural Hematoma and a Basilar Skull Fracture. On second look by a trained Neuroradiologist c At 3 month follow up, patient’s tongue normalized to midline and his dysphagia resolved. Discussion: Collette-Sicard syndrome is a rare condition/syndrome characterized by unilateral palsy of CN: IX, X, XII. This condition has been rarely described as a consequence of blunt head trauma. In most cases, the condition is self-limiting with patients regaining most to all of their neurological functions within 6 months. Nerve traction injuries and soft tissue edema compressing the cranial nerves are the leading two hypothesis. -

Cranial Nerve Disorders: Clinical Manifestations and Topographyଝ
Radiología. 2019;61(2):99---123 www.elsevier.es/rx UPDATE IN RADIOLOGY Cranial nerve disorders: Clinical manifestations and topographyଝ a,∗ a b c M. Jorquera Moya , S. Merino Menéndez , J. Porta Etessam , J. Escribano Vera , a M. Yus Fuertes a Sección de Neurorradiología, Hospital Clínico San Carlos, Madrid, Spain b Servicio de Neurología, Hospital Clínico San Carlos, Madrid, Spain c Neurorradiología, Hospital Ruber Internacional, Madrid, Spain Received 17 November 2017; accepted 27 September 2018 KEYWORDS Abstract The detection of pathological conditions related to the twelve cranial pairs rep- Cranial pairs; resents a significant challenge for both clinicians and radiologists; imaging techniques are Cranial nerves; fundamental for the management of many patients with these conditions. In addition to knowl- Cranial neuropathies; edge about the anatomy and pathological entities that can potentially affect the cranial pairs, Neuralgia; the imaging evaluation of patients with possible cranial pair disorders requires specific exami- Cranial nerve palsy nation protocols, acquisition techniques, and image processing. This article provides a review of the most common symptoms and syndromes related with the cranial pairs that might require imaging tests, together with a brief overview of the anatomy, the most common underlying processes, and the most appropriate imaging tests for different indications. © 2018 SERAM. Published by Elsevier Espana,˜ S.L.U. All rights reserved. PALABRAS CLAVE Sintomatología derivada de los pares craneales: Clínica y topografía Pares craneales; Resumen La detección de la patología relacionada con los doce pares craneales representa Nervios craneales; un importante desafío, tanto para los clínicos como para los radiólogos. Las técnicas de imagen Neuropatía de pares craneales; son fundamentales para el manejo de muchos de los pacientes. -

Hypoglossal-Facial Nerve Side-To-End Anastomosis for Preservation of Hypoglossal Function: Results of Delayed Treatment With
Hypoglossalfacial nerve side-to-end anastomosis for preservation of hypoglossal function: results of delayed treatment with a new technique Yutaka Sawamura, M.D., and Hiroshi Abe, M.D. Department of Neurosurgery, University of Hokkaido, School of Medicine, Sapporo, Japan This report describes a new surgical technique to improve the results of conventional hypoglossalfacial nerve anastomosis that does not necessitate the use of nerve grafts or hemihypoglossal nerve splitting. Using this technique, the mastoid process is partially resected to open the stylomastoid foramen and the descending portion of the facial nerve in the mastoid cavity is exposed by drilling to the level of the external genu and then sectioning its most proximal portion. The hypoglossal nerve beneath the internal jugular vein is exposed at the level of the axis and dissected as proximally as possible. One-half of the hypoglossal nerve is transected: use of less than one-half of the hypoglossal nerve is adequate for approximation to the distal stump of the atrophic facial nerve. The nerve endings, the proximally cut end of the hypoglossal nerve, and the distal stump of the facial nerve are approximated and anastomosed without tension. This technique was used in four patients with long-standing facial paralysis (greater than 24 months), and it provided satisfactory facial reanimation, with no evidence of hemitongue atrophy or dysfunction. Because it completely preserves glossal function, the hemihypoglossalfacial nerve anastomosis described here constitutes a successful -

Brainstem Reflexes Herniation Syndromes (CN IX-XII) Lab 7 March 24, 2021 - Dr
Brainstem Reflexes Herniation Syndromes (CN IX-XII) Lab 7 March 24, 2021 - Dr. Krebs ([email protected]) Objectives: 1. Describe the relationship of the functional anatomy of CN IX - XII and the location of their respective nuclei to a neurological exam which examines the brainstem. 2. Explain the neuroanatomical pathways associated with brainstem reflexes tested in the conscious and unconscious patient. 3. Describe the relationship between the sympathetic and parasympathetic innervation of the eye to the clinical assessment of eye reflexes. 4. Describe the relationship of changes in upper limb posture of unconscious patient to underlying damage to the brainstem. 5. Describe the consequences of herniation syndromes associated with increases in intracranial pressure. Videos for Review: Notes: • For identification of the cranial nerves, use online modules and videos, your atlas and micrographs to locate the nuclei listed. • On the brain and brainstem specimens, locate cranial nerves IX, X, XI and XII. Note the level at which they are attached to the brainstem. ** NOTE: Interactive PDFs are best viewed on desktop/laptop computers - functionality is not reliable on mobile devices ** Design & Artwork: The HIVE (hive.med.ubc.ca) 1 Brainstem Reflexes Herniation Syndromes (CN IX-XII) Lab 7 March 24, 2021 - Dr. Krebs ([email protected]) Glossopharyngeal Nerve (CN IX) Modality Associated Nucleus Function Motor Nucleus ambiguus Motor to stylopharyngeus muscle (SVE) Parasympathetic Inferior salivatory nucleus Stimulation of parotid gland (GVE) Taste Solitary nucleus and tract Taste from posterior 1/3 of tongue (SVA) Somatic Sensory Spinal trigeminal nucleus and General sensation from posterior 1/3 of tongue, (GSA) tract pharynx, external ear/tympanic membrane Visceral Sensory Solitary nucleus and tract Carotid body, gag sensation from oropharynx (GVA) Which foramen does CN IX exit through? Highlight and label the nuclei associated with CN IX in this diagram and show the types of fibres that comprise this peripheral nerve. -

Tongue Fasciculations with Denervation Pattern in Osmotic Demyelination Syndrome: a Case Report of Diagnostic Dilemma H
Herath et al. BMC Res Notes (2018) 11:177 https://doi.org/10.1186/s13104-018-3287-8 BMC Research Notes CASE REPORT Open Access Tongue fasciculations with denervation pattern in osmotic demyelination syndrome: a case report of diagnostic dilemma H. M. M. T. B. Herath*, S. P. Pahalagamage and Sunethra Senanayake Abstract Background: The pathogenesis of osmotic demyelination syndrome is not completely understood and usually occurs with severe and prolonged hyponatremia, particularly with rapid correction. It can occur even in normo- natremic patients, especially who have risk factors like alcoholism, malnutrition and liver disease. Bilateral tongue fasciculations with denervation pattern in electromyogram is a manifestation of damage to the hypoglossal nucleus or hypoglossal nerves. Tongue fasciculations were reported rarely in some cases of osmotic demyelination syndrome, but the exact mechanism is not explained. Case presentation: A 32-year-old Sri Lankan male, with a history of daily alcohol consumption and binge drinking, presented with progressive difculty in walking, dysphagia, dysarthria and drooling of saliva and alteration of con- sciousness. On examination he was akinetic and rigid resembling Parkinsonism with a positive Babinski sign. Clinical features were diagnostic of osmotic demyelination syndrome and MRI showed abnormal signal intensity within the central pons and basal ganglia. He also had tongue fasciculations. The electromyogram showed denervation pattern in the tongue with normal fndings in the limbs. Medulla and bilateral hypoglossal nerves were normal in MRI. Conclusion: We were unable to explain the exact mechanism for the denervation of the tongue, which resulted in fasciculations in this chronic alcoholic patient who developed osmotic demyelination syndrome. -

Unilateral Laryngeal and Hypoglossal Paralysis (Tapia’S Syndrome) in a Patient
G Model CLINEU-3181; No. of Pages 3 ARTICLE IN PRESS Clinical Neurology and Neurosurgery xxx (2012) xxx–xxx Contents lists available at SciVerse ScienceDirect Clinical Neurology and Neurosurgery journa l homepage: www.elsevier.com/locate/clineuro Case reports Unilateral laryngeal and hypoglossal paralysis (Tapia’s syndrome) in a patient with an inflammatory pseudotumor of the neck a,1 b,1 a b,∗ Antonio Lo Casto , Rossella Spataro , Pierpaolo Purpura , Vincenzo La Bella a Department of Radiological Sciences, DIBIMEF, University of Palermo, 90129 Palermo, Italy b ALS Clinical Research Center, Department of Experimental Biomedicine and Clinical Neurosciences, BioNeC, University of Palermo, 90129 Palermo, Italy a r t i c l e i n f o Article history: Received 25 October 2012 Accepted 25 November 2012 Available online xxx Keywords: Inflammatory pseudotumor Tapia’s syndrome Laryngeal nerve Hypoglossal nerve 1. Introduction tongue, which was deviated to the right side (Fig. 1A), a voice hoarseness and dysphonia. Of note, the patient was unaware of Tapia’s syndrome (TS) is a rare condition thought to be caused by the tongue hemiatrophy. She was not significantly dysphagic, as injury to the extracranial course of both recurrent laryngeal branch the 100 ml water swallow test was within normal range. All other of the vagal nerve and hypoglossal nerve. First described in 1904, cranial nerves appeared undamaged. it occurs with unilateral paralysis of the vocal cord and tongue, An extensive biochemical and immunological work-up were with normal function of the soft palate. Commonly reported causes negative (including blood cell counts and a search for onconeural are direct trauma, neurofibromatosis of X and XII nerves, carotid and anti-ganglioside antibodies). -

The 12 Cranial Nerves
The 12 Cranial Nerves Nerve # Name Function 1st Olfactory Relays smell 2nd Optic Transmits visual information 3rd Oculomotor External muscles of the eye 4th Trochlear Also supplies muscles of the eye 5th Trigeminal Chewing and sensation in the face 6th Abducent Controls lateral eye movement 7th Facial Muscles of facial expression, taste buds, sensation in fingers and toes, blinking 8th Auditory Hearing and balance 9th Glossopharyngeal Sensation, taste and swallowing 10th Vagus Organs in chest and abdomen 11th Accessory Supplies two neck muscles, the sternomastoid and trapezius 12th Hypoglossal Muscles of the tongue and neck The 12 Cranial Nerves—Detail Cranial Nerve 1 Sensory nerve – Olfactory Nerve – controls sense of smell Cranial Nerve 2 Sensory nerve- Optic Nerve- controls vision by sending information from retina Cranial Nerve 3 Motor nerve- Oculomotor Nerve-Controls most eye muscles. Works closely with Cranial Nerves 4 & 6. Controls eye movement, pupil dilation, and pupillary constriction. It also controls the muscles that elevate the upper eyelids. Cranial Nerve 4 Motor nerve- Trochlear Nerve- Controls the downward and outward movement of the eye. Works closely with Cranial Nerves 3 & 6. Can cause vertical Diplopia (double vision). Weakness of downward gaze can cause difficulty in descending stairs. Cranial Nerve 5 Motor and sensory nerve-Trigeminal Nerve-Carries sensory information from most of the head, neck, sinuses, and face. Also carries sensory information for ear and tympanic membrane. Provides motor supply to the muscles of masticulation (chewing), and to some of the muscles on the floor of the mouth. Also provides motor supply to tensor tympani (small muscle in the middle ear which tenses to protect the eardrum). -

Hypoglossal Nerve Palsy
PICTORIAL MEDICINE Hypoglossal nerve palsy The hypoglossal nerve receives only brief mention metastatic carcinomas, chordomas, nasopharyngeal in most textbooks and compared with other cranial carcinomas, gliomas, and acoustic neuromas.1,2 In the nerve palsies, 12th nerve palsy is much less common. only large series, 100 cases reported by Keane,1 the We report a 52-year-old woman who presented with next most common category was trauma—usually right-sided headaches for over a year. It was only on penetrating injuries. Uncommon causes include examination that we discovered she had an abnormal multiple sclerosis and idiopathic isolated hypoglossal tongue. She had wasting and fasciculations on the right nerve palsy, which is a diagnosis of exclusion. Acute side of her tongue, which was deviated to the right side, onset of pain with tongue weakness points to due to the unopposed action of the unaffected left dissection of the extracranial internal carotid artery, side (Fig 1). The rest of the neurological examination a medical emergency.3 Bilateral tongue wasting is was unremarkable. On further questioning she said usually due to neurological disorders such as motor she had no problems with speech, mastication, or neurone disease and Kennedy’s disease.4,5 Even with swallowing. Magnetic resonance imaging confirmed bilateral involvement it is uncommon for patients a well-defined mass lesion encroaching on the right to complain specifically about tongue function. side of the foramen magnum and the hypoglossal Occasionally we see psychogenic or hysterical 12th canal, with displacement of the right medulla and nerve palsy in which the tongue may be deviated to the inferior cerebellar hemisphere (Figs 2, 3). -
The Nervous System: the Brain and Cranial Nerves
16 The Nervous System: The Brain and Cranial Nerves PowerPoint® Lecture Presentations prepared by Steven Bassett Southeast Community College Lincoln, Nebraska © 2012 Pearson Education, Inc. Introduction • The brain is a complex three-dimensional structure that performs a bewildering array of functions • Think of the brain as an organic computer • However, the brain is far more versatile than a computer • The brain is far more complex than the spinal cord • The brain consists of roughly 20 billion neurons © 2012 Pearson Education, Inc. An Introduction to the Organization of the Brain • Embryology of the brain • The CNS begins as a neural tube • The lumen of the tube (neurocoel) is filled with fluid • In the fourth week of development, the cephalic area of the neural tube enlarges to form: • Prosencephalon • Mesencephalon • Rhombencephalon © 2012 Pearson Education, Inc. Table 16.1 Development of the Human Brain © 2012 Pearson Education, Inc. An Introduction to the Organization of the Brain • Embryology of the brain (continued) • Prosencephalon eventually develops to form: • Telencephalon: forms the cerebrum • Diencephalon: forms the epithalamus, thalamus, and hypothalamus © 2012 Pearson Education, Inc. An Introduction to the Organization of the Brain • Mesencephalon • Does not subdivide • Becomes the midbrain • Rhombencephalon • Eventually develops to form: • Metencephalon: forms the pons and cerebellum • Myelencephalon: forms the medulla oblongata © 2012 Pearson Education, Inc. Figure 16.1 Major Divisions of the Brain Left cerebral hemisphere -

Tongue Hemi Atrophy–Hypoglossal Neurolemmoma
International Journal of Radiology & Radiation Therapy Case Report Open Access Tongue hemi atrophy–hypoglossal neurolemmoma Abstract Volume 5 Issue 6- 2018 Neurolemmomas are benign nerve sheath tumours with extra vestibular cranial nerve Avni KP Skandhan involvement being very rare, rarest of them being hypoglossal nerve (cranial nerve Malabar Institute of Medical Sciences, India XII). We report the case of a hypoglossal nerve shcwannoma with extra cranial extension. Correspondence: Avni KP Skandhan, Malabar Institute of Keywords: neurolemmoma, hypoglossal nerve Medical Sciences, Kotakkal, Malappuram, 676 503, Kerala, India, Email Received: February 18, 2018 | Published: November 26, 2018 Key messages A hypoglossal nerve neurolemmoma might present as hypoglossal nerve palsy, muscle atrophy of tongue but sometimes may be asymptomatic initially. Early diagnosis may be achieved with detailed neurological examination and only a strong suspicion leads to a targeted imaging. Introduction Neurolemmomas (schwannoma, neuromas, neurilemmomas) are benign tumours originating from Schwann cells or nerve fibre sheath cells. Neurolemmomas of the hypoglossal nerve are exceedingly rare with less than 100 documented cases. Exact incidence is not available. Neurolemmomas of the hypoglossal nerve usually develop in the intracranial portion or both in the intracranial and the extra cranial components forming a dumb-bell shape. We present a case which on magnetic resonance imaging presented as an intensely enhancing Figure 1 STIR coronal images showing a hyper intense lesion arising posterior fossa mass with extension into the carotid space up to the from the medulla on the left side at the region of hypoglossal canal. Left carotid bifurcation. hypoglossal nerve not visualized separately. Case history A 40 year old male presented with recent onset of slurring of speech and fissuring of tongue. -

Cranial Nerves XI-XII
Cranial Nerves XI-XII Color Code Important (Accessory & Hypoglossal Nerves) Doctors Notes Notes/Extra explanation Please view our Editing File before studying this lecture to check for any changes. Objectives At the end of the lecture, the students should be able to: ✓ List the nuclei related to accessory and hypoglossal nerves in the brain stem. ✓ Describe the type and site of each nucleus. ✓ Describe site of emergence and course of accessory and hypoglossal nerves. ✓ Describe important relations of accessory and hypoglossal nerves in the neck. ✓ List the branches of accessory and hypoglossal nerves. ✓ Describe the main motor effects in case of lesion of accessory and hypoglossal nerves. Extra Slide: Mnemonics And Pictures To Help Memorise The Cranial Nerves 07:32 Big Brains Matter More Accessory (XI) 11th Cranial Nerve o Type: Motor o Has two parts (roots)*: • Cranial part • Spinal part Extra carries fibres that arises from motor originate in the neurones in ventral caudal part of horn of the spinal gray nucleus ambiguus. matter at levels C1-C5 (spinal nucleus) o Foramen of exit from skull: Jugular foramen. * يختلف هذا العصب بأنه الوحيد بين الباقين إلي يأخذ من جزئيين Accessory (XI) 11th Cranial Nerve Cranial Part o Emerges from lateral aspect of the medulla as a linear series of rootlets caudal to rootlets of the vagus nerve. o At the side of medulla it joins the spinal root briefly. o It separates once again as the nerve leaves the cranial cavity through the Jugular foramen. o At the level of jugular foramen these fibres join the vagus nerve and distribute with it to muscles of the soft plate, esophagus, pharynx and larynx. -

Brainstem Encephalitis Caused by Listeria Monocytogenes
pathogens Review Brainstem Encephalitis Caused by Listeria monocytogenes Pengxu Wei 1,2, Ruixue Bao 3 and Yubo Fan 1,2,* 1 School of Biological Science and Medical Engineering and Beijing Advanced Innovation Center for Biomedical Engineering, Beihang University, 37# Xueyuan Road, Haidian District, Beijing 100083, China; [email protected] 2 Beijing Key Laboratory of Rehabilitation Technical Aids for Old-Age Disability, Key Laboratory of Intelligent Control and Rehabilitation Technology of the Ministry of Civil Affairs, National Research Center for Rehabilitation Technical Aids, No. 1 Ronghuazhong Road, Beijing Economic and Technological Development Zone, Beijing 100176, China 3 School of Rehabilitation Medicine, China Rehabilitation Research Center, Capital Medical University, Beijing 100068, China; [email protected] * Correspondence: [email protected]; Tel.: +86-10-58122818 Received: 6 August 2020; Accepted: 28 August 2020; Published: 30 August 2020 Abstract: International outbreaks of listerial infections have become more frequent in recent years. Listeria monocytogenes, which usually contaminates food, can cause potentially fatal infections. Listerial cerebritis is a rare disease that is encountered mostly in immunocompromised or elderly patients. However, listerial brainstem encephalitis (mesenrhombencephalitis or rhombencephalitis) is found in persons who were formerly in good health, and recognizing this disease, particularly at its early stages, is challenging. Listerial brainstem encephalitis has high mortality, and serious sequelae are frequently reported in survivors. Early recognition and correct diagnosis, as well as the timely use of appropriate antibiotics, can reduce the severity of listerial infections. The trigeminal nerve is proposed as a pathway through which L. monocytogenes reaches the brainstem after entering damaged oropharyngeal mucosa or periodontal tissues.