Biomedical Engineering: Advancing Uk Healthcare
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Department of Biomedical Engineering (GRAD) 1
Department of Biomedical Engineering (GRAD) 1 Candidates for the UNC–Chapel Hill/North Carolina State University DEPARTMENT OF BIOMEDICAL jointly issued degrees in biomedical engineering must have met the general requirements of The Graduate School of the University of North ENGINEERING (GRAD) Carolina at Chapel Hill or the North Carolina State University Graduate School. Contact Information *Currently matriculating* master’s students are required to take a Department of Biomedical Engineering comprehensive examination encompassing coursework and thesis Visit Program Website (http://www.bme.unc.edu) research. The master’s comprehensive exam may be either written or oral and is administered by the student’s advisory committee. Nancy L. Allbritton, Chair Doctoral students qualify for the Ph.D. degree by meeting grade Biomedical engineering is a dynamic field stressing the application requirements in their core courses and then advancing to written and of engineering techniques and mathematical analysis to biomedical oral preliminary exams before admission to candidacy. Details can be problems. Faculty research programs are key to the program, and they found on the department's website (https://bme.unc.edu/). Degree include five primary research directions: rehabilitation engineering, candidates in this program are expected to obtain experience working biomedical imaging, pharmacoengineering, regenerative medicine, and in a research laboratory during their residence and to demonstrate biomedical microdevices. The department offers graduate education in proficiency in research. The Ph.D. dissertation should be judged by the biomedical engineering leading to the master of science and doctor of graduate committee to be of publishable quality. philosophy degrees. Also, a joint graduate certificate in medical devices is offered. -

BET Bionanotechnology and Advanced Biomanufacturing - 1B
Course Package BET Bionanotechnology and Advanced Biomanufacturing - 1B Name module BET - Bionanotechnology and Advanced Biomanufacturing – 1B Educational programme MSc Biomedical Engineering Period Second quartile of the first semester (Block 1B) Study load 15 ECTS Coordinator J. Huttenhuis BET - Bionanotechnology and Advanced Biomanufacturing block 1A block 1B block 2A block 2B Biomedical Materials Engineering - 201400283 (5 EC) Nanomedicine - 201200220 (5 EC) Lab on a Chip - 191211120 (5 EC) Required preliminary knowledge: Followed the course 201600127 Introduction to Bionanotech & adv. Biomanufacturing in block 1A. A proven knowledge of Organic chemistry, polymer chemistry, biomaterials, cell-material interactions. 201400283 Biomedical Materials Engineering This course deals with the basic principles of tissue-biomaterial interactions, surface modification of biomaterials and polymer processing for regenerative medicine. Moreover, groups of 4-5 students draw up a research proposal that has to be defended during a plenary session. The modules are tentative and subject to change. Please check the website regularly. 201200220 Nanomedicine Nanomedicine is one of the most dynamic fields, which holds a high potential to make a huge impact on the medical science. Nanomedicine is in general defined as medical applications of nanotechnology. In recent years, nanotechnologies have been applied for drug delivery, imaging/diagnostics, biosensing, in vitro diagnostics, and tissue engineering. One of the largest areas for nanomedicine is the drug delivery/targeting. Conventional medicine, which are either administered orally or with injections, are not always successful for achieving the desired therapeutic effects but rather show high side effects. Therefore, novel drug delivery systems are highly crucial to develop, using which the drugs can be specially delivered at the targeted site or even to the specific cell types. -
Biomedical Engineering Year 2 Course Description
Making Opportunity Affordable in Texas: A Student-Centered Approach Tuning of Biomedical Engineering Texas Higher Education Coordinating Board Austin, Texas with grant support from Lumina Foundation for Education Completion date: May 2012 Tuning Oversight Council for Engineering and Science Biomedical Engineering Committee John C. Criscione, M.D., Ph.D. (Chair) Lennine Bashiri (Co-Chair) Associate Professor of Biomedical Engineering Instructor Department of Biomedical Engineering South Texas College Texas A&M University 3201 W. Pecan Blvd. 3120 TAMUS McAllen, TX 78502 College Station, TX 77843-3131 [email protected] [email protected] Leonidas Bleris, Ph.D. Ting Chen, Ph.D. Assistant Professor Instructional Assistant Professor,Research Assistant Professor, Department of Bioengineering Academic Advising Coordinator The University of Texas at Dallas Department of Biomedical Engineering 800 W. Campbell Rd Cullen College of Engineering Richardson, TX 75080 University of Houston [email protected] 3605 Cullen Blvd, Room 2018 Houston, TX 77204-5060 [email protected] Cheng-Jen "Charles" Chuong, Ph.D. Charlene Cole Professor Chair, Department of Life Sciences The University of Texas at Arlington Tarrant County Community College NE Arlington, TX 76019-0019 Department of Life Sciences [email protected] Hurst, TX 78054 [email protected] Harvinder Singh Gill, Ph.D. Joo L. Ong, Ph.D. Assistant Professor UTSA Distinguished Professor and Chair Department of Chemical Engineering The University of Texas at San Antonio Texas Tech University Department of Biomedical Engineering Lubbock, TX 79409-3121 San Antonio, TX 78249 [email protected] [email protected] Patrice Parsons, Ph.D. Chandeshwar Sharma, Ph.D. Professor Instructor, Coleman College for Health Sciences Grayson Community College Houston Community College Denison, TX 75020 Houston, TX 77030 [email protected] [email protected] James Tunnell, Ph.D. -

Introducing Bionanotechnology Into Undergraduate Biomedical Engineering
AC 2009-504: INTRODUCING BIONANOTECHNOLOGY INTO UNDERGRADUATE BIOMEDICAL ENGINEERING Aura Gimm, Duke University J. Aura Gimm is Assistant Professor of the Practice and Associated Director of Undergraduate Studies in the Department of Biomedical Engineering at Duke University. She teaches courses in biomaterials, thermodynamics/kinetics, engineering design, and a new course in bionanotechnology. Dr. Gimm received her S.B. in Chemical Engineering and Biology from MIT, and her Ph.D. in Bioengineering from UC-Berkeley. Page 14.802.1 Page © American Society for Engineering Education, 2009 Introducing Bionanotechnology in Undergraduate Biomedical Engineering Abstract As a part of the NSF-funded Nanotechnology Undergraduate Education Program, we have developed and implemented a new upper division elective course in Biomedical Engineering titled “Introduction to Bionanotechnology Engineering”. The pilot course included five hands- on “Nanolab” modules that guided students through specific aspects of nanomaterials and engineering design in addition to lecture topics such as scaling effects, quantum effects, electrical/optical properties at nanoscale, self-assembly, nanostructures, nanofabrication, biomotors, biological designing, biosensors, etc. Students also interacted with researchers currently working in the areas of nanomedicine, self-assembly, tribiology, and nanobiomaterials to learn first-hand the engineering and design challenges. The course culminated with research or design proposals and oral presentations that addressed specific engineering/design issues facing nanobiotechnology and/or nanomedicine. The assessment also included an exam (only first offering), laboratory write-ups, reading of research journal articles and analysis, and an essay on ethical/societal implications of nanotechnology, and summative questionnaire. The course exposed students to cross-disciplinary intersections that occur between biomedical engineering, materials science, chemistry, physics, and biology when working at the nanoscale. -

Biomedical Engineering Department Medical
BIOMEDICAL ENGINEERING DEPARTMENT MEDICAL ENGINEERING UNDERGRADUATE CURRICULUM 2014-15 (as of 5/10/13) The Medical Engineering Program is an option for HPME student only. This program is not accredited by the Engineering Accreditation Commission of ABET, http://www.abet.org. However, our Biomedical Engineering Program is accredited by this organization. Students entering this program are expected to have advanced work in high school such that they can be placed into MATH 230 and CHEM 171, or higher. All courses must be passed with a C grade or higher, and no courses within the 48 required for the degree may be taken P/N without approval. I. MATHEMATICS (4 courses) AP placement-Math 220, 224 MATH 230 Calculus MATH 234 Multiple Integration and Vector Calculus II. BASIC SCIENCES (4 courses) PHYSICS 135-2, 3 General Physics CHEM 171, 172 Accelerated Chemistry III. ENGINEERING ANALYSIS (4 courses) GEN ENG 205-1 Computational Methods and Linear Algebra GEN ENG 205-2 Linear Algebra and Mechanics GEN ENG 205-3 Dynamic System Modeling GEN ENG 205-4 Differential Equations IV. ENGINEERING DESIGN AND COMMUNICATION (3 courses) Speech 102, or 103 or Taken at Medical School IDEA 106-1, 2 Engineering Design and Communication (0.5 each) plus English 106-1,2 (0.5 each). V. BASIC ENGINEERING (5 courses) A. Thermodynamics - 1 course listed from those below BMD_ENG 250 Thermodynamics CHEM 342-1 Thermodynamics MECH ENG 220 Thermodynamics I B. Fluids and Solids - 2 courses as specified below BMD_ENG 271 Introduction to Biomechanics and BMD_ENG 270 Fluid Mechanics or MECH ENG 241 Fluid Mechanics I C. -

Engineering Solutions for Health: Biomedical Engineering Research Strategy March 2015
Engineering Solutions for Health: Biomedical Engineering Research Strategy March 2015 Biomedical engineering is the application of engineering tools and approaches to advance knowledge and solve problems in animal and human biology, medicine and health care. Engineering Solutions for Health: Biomedical Engineering Research Strategy Biomedical engineering has dramatically advanced health care and health- related research over the past half-century for both human and animal populations, and will have an even greater influence in the future. High- quality health care is the foundation of a healthy society: health is at the core of quality of life and also drives social and economic development. Biomedical engineering makes important differences every day to individuals by extending their lives, ensuring the safety of their food and water supplies, improving their quality of life, promoting independence, and providing more effective options for front-line health care professionals. The University of Calgary has a strong track record This strategy will target health problems with of great accomplishments in biomedical engineering, the highest burden in terms of decreased quality based on making significant investments in this area of life, financial cost, mortality and morbidity to build a solid foundation of truly interdisciplinary — particularly cardiovascular disease, cancer, research and training. Engineering Solutions for injuries, musculoskeletal diseases and neurological Health: Biomedical Engineering is one of the conditions. Biomedical -

Biomedical Engineering (BME)
COURSE DESCRIPTIONS Fall 2008: updates since Spring 2007 are in red BME 301 Bioelectricity medical engineering, biological signal measurement, Theoretical concepts and experimental approaches conditioning, digitizing, and analysis. Advanced appli- BME used to characterize electric phenomena that arise in cations of LabVIEW, a graphics programming tool for live cells and tissues. Topics include excitable mem- virtual instrumentation. Helps students develop skills Biomedical Engineering branes and action potential generation, cable theory, to build virtual instrumentation for laboratory equivalent dipoles and volume conductor fields, bio- research and prototyping medical devices. Prerequisite: BME 212 BME 100 Introduction to Biomedical electric measurements, electrodes and electric stimu- lation of cells and tissues. 3 credits Engineering Prerequisites: BME 212; ESE 271; ESG 111 (or ESE A rigorous introduction to biomedical engineering 124); BIO 202 or 203 BME 353 Biomaterials: Manufacture, that provides the historical and social context of BME 3 credits Properties, and Applications though contemporary emerging areas within BME. The engineering characteristics of materials, includ- Specific areas covered in depth include: bioelectricity ing metals, ceramics, polymers, composites, coatings, and biosensors (action potentials to signal process- BME 303 Biomechanics and adhesives, that are used in the human body. ing), bioimaging (invasive and non-invasive), genetic Illuminates the principles of mechanics and dynamics Emphasizes the need of materials that are considered engineering (with ethical discussions), and biostatis- that apply to living organisms, from cells to humans to for implants to meet the material requirements speci- tics. Hands-on computational modeling introduces the Sequoia trees. The behavior of organisms is examined fied for the device application (e.g., strength, modu- physiological concept of positive and negative feed- to observe how they are constrained by the physical lus, fatigue and corrosion resistance, conductivity) back loops in the body. -
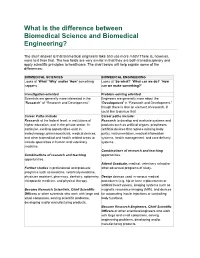
What Is the Difference Between Biomedical Science and Biomedical Engineering?
What is the difference between Biomedical Science and Biomedical Engineering? The short answer is that Biomedical engineers take and use more math! There is, however, more to it than that. The two fields are very similar in that they are both transdisciplinary and apply scientific principles to healthcare. The chart below will help explain some of the differences: BIOMEDICAL SCIENCES BIOMEDICAL ENGINEERING Looks at ‘What’ ‘Why’ and/or ‘How’ something Looks at ‘So what?’ ‘What can we do?’ ‘How happens. can we make something?’ Investigation-oriented Problem-solving oriented Scientists are generally more interested in the Engineers are generally more about the “Research” of “Research and Development.” “Development” in “Research and Development,” though there is also an element of research, if you'd like to pursue that. Career Paths include Career paths include: Research at the federal level, in institutions of Research to develop and evaluate systems and higher education, and in the private sector. In products such as artificial organs, prostheses particular, exciting opportunities exist in (artificial devices that replace missing body biotechnology, pharmaceuticals, medical devices, parts), instrumentation, medical information and other biomedical and health related areas to systems, health management, and care delivery include specialties in human and veterinary systems. medicine. Combinations of research and teaching Combinations of research and teaching opportunities. opportunities. Attend Graduate, medical, veterinary school or Further -

Biomedical Engineering and Medicine Dual Degree
BIOMEDICAL ENGINEERING AND MEDICINE DUAL DEGREE PROGRAM Doctor of Philosophy (Ph.D.) Degree in Biomedical Engineering and Doctor of Medicine (M.D.) Degree in Medicine DEGREE INFORMATION Program Admission Deadlines: Fall: November 1 Spring: No Admit Summer: No Admit Minimum Total Hours: 90/ Program Level: Doctoral/Professional CIP Code: 14.0501 Dept Code: ECH Program (Major/College): EBI EN CONTACT INFORMATION Colleges: Engineering/Medicine Departments: Chemical & Biomedical Engineering; Medicine Contact Information: www.grad.usf.edu PROGRAM INFORMATION The objectives of the M.D./Ph.D. program are: 1) produce highly trained professionals who can work effectively in the area of Biomedical Translational Research, more specifically, Engineer‐Physicians who can conduct research in a Biomedical engineering area that addresses a significant clinical problem, and bring that research through to clinical application; and 2) provide an integrated educational experience leading to both the M.D. degree and the Ph.D. (BME) degree. In order to accomplish the first objective, advances in health care increasingly involve the application of emerging science and technology (i.e., engineering) to clinical problems, including problems in diagnostic treatment and the healthcare system itself. Unlike more basic research that often aims to increase science and technology knowledge in itself, translational research seeks to specifically address the science and technology needed to solve problems with the end goal of creating an actual application or product (of course, adding new significant knowledge in the process). In order to conduct effective biomedical translational research, the investigator must be trained in both clinical science (i.e., the M.D. degree) and engineering (specifically, Biomedical Engineering). -

Biomedical Engineering Course Plan (16-17)
Biomedical Engineering Course Plan (16-17) Freshman Year Sophomore Year ENGI 1100 – Intro to Engineering CHEM 3331 & 3221 – Organic Chemistry I & Lab BIOL 1361 & 1161 – Biological Science 1 & Lab BIOE 2100– Intro to Biomedical Engr CHEM 1331 & 1111 – Chemistry I & Lab ENGL 1304/1310 – Freshman Comp II Fall Fall ENGL 1303/1309 – Freshman Comp I MATH 2433 – Calculus III MATH 1431 – Calculus I PHYS 1322 – University Physics II ENGI 1331 – Computers & Problem-Solving CHEE 2331 – Chemical Processes BIOL 1362 & 1162 – Biological Science 2 & Lab ECE 2201 – Circuit Analysis I CHEM 1332 & 1112 – Chemistry 2 & Lab BCHS 3304 – Biochemistry I Spring MATH 1432 – Calculus II Spring MATH 3321 – Engineering Math PHYS 1321 – University Physics I Core Course/Social & Behavioral Sciences Core Course/Creative Arts Junior Year Senior Year MECE 3400 – Intro to Mechanics BIOE 4315 & 4115 – Intro to Bioinstrumentation & Lab BIOE 3340 & 3140 – Quantitative Physiology & Lab BIOE 4335 – Capstone Design I Core Course/HIST 1377 – US History to 1877 BIOE Track Course* Fall Fall ENGI 2304 – Technical Communication BIOE Track Course* INDE 2333 – Engineering Statistics Core Course/POLS 1337 – US Government BIOE 3341 - Biothermodynamics BIOE 4336 – Capstone Design II BIOE Track Course* BIOE Track Course* BIOE Track Course* BIOE Track Course* Spring Core Course/HIST 1378 – US History Since 1877 Spring BIOE Track Course* Core Course/POLS 1336 – US & TX Constitutions Core Course/Language, Philosophy, & Culture *Choose One Track: Neural, Cognitive, & Rehabilitation Bionanoscience -

Biomedical Engineering (BME) 1
Biomedical Engineering (BME) 1 BIOMEDICAL ENGINEERING (BME) BME 100 BME 315 Introduction to the Profession Instrumentation and Measurement Laboratory Introduces the student to the scope of the biomedical engineering Laboratory exercises stress instrumentation usage and data profession and its role in society, and develops a sense of analysis used to determine physiological functions and variables professionalism in the student. Provides an overview of biomedical and the relations to the physiological variability. engineering through lectures, presentations by outside speakers, Prerequisite(s): ECE 211* and BME 200, An asterisk (*) designates a hands-on exercises, and scientific literature analyses. Develops course which may be taken concurrently. professional communication and teamwork skills. Lecture: 0 Lab: 3 Credits: 1 Lecture: 1 Lab: 2 Credits: 2 Satisfies: Communications (C) BME 320 Fluids Laboratory BME 200 Laboratory experiments in thermodynamics, biological fluid Biomedical Engineering Computer Applications flow, and heat transfer. Emphasis is placed on current methods, In this course, students will apply programming to solve quantitative instrumentation, and equipment used in biomedical engineering; oral biomedical engineering problems across cell/tissue engineering, presentation of results; and on the writing of comprehensive reports. neural engineering, and medical imaging. Students will also be Open only to Biomedical Engineering majors. exposed to additional engineering and product development Corequisite(s): BME 301 programming tools and environments. Prerequisite(s): BIOL 117 and BME 315 Prerequisite(s): MATH 252* and CS 104, An asterisk (*) designates a Lecture: 0 Lab: 3 Credits: 1 course which may be taken concurrently. Satisfies: Communications (C) Lecture: 1 Lab: 2 Credits: 2 BME 325 BME 301 Bioelectronics Laboratory Bio-Fluid Mechanics Practical hands on design, construction and testing of electric and Basic properties of fluids in motion. -
Nanoscale Bioengineering and Nanomedicine the Artech House Methods in Bioengineering Series Series Editors-In-Chief Martin L
Methods in Bioengineering Nanoscale Bioengineering and Nanomedicine The Artech House Methods in Bioengineering Series Series Editors-in-Chief Martin L. Yarmush, M.D., Ph.D. Robert S. Langer, Sc.D. Methods in Bioengineering: Biomicrofabrication and Biomicrofluidics, Jeffrey D. Zahn and Luke P. Lee, editors Methods in Bioengineering: Microdevices in Biology and Medicine, Yaakov Nahmias and Sangeeta N. Bhatia, editors Methods in Bioengineering: Nanoscale Bioengineering and Nanomedicine, Kaushal Rege and Igor Medintz, editors Methods in Bioengineering: Stem Cell Bioengineering, Biju Parekkadan and Martin L. Yarmush, editors Methods in Bioengineering: Systems Analysis of Biological Networks, Arul Jayaraman and Juergen Hahn, editors Series Editors Martin L. Yarmush, Harvard Medical School Christopher J. James, University of Southampton Advanced Methods and Tools for ECG Data Analysis, Gari D. Clifford, Francisco Azuaje, and Patrick E. McSharry, editors Advances in Photodynamic Therapy: Basic, Translational, and Clinical, Michael Hamblin and Pawel Mroz, editors Biomedical Surfaces, Jeremy Ramsden Intelligent Systems Modeling and Decision Support in Bioengineering, Mahdi Mahfouf Translational Approaches in Tissue Engineering and Regenerative Medi- cine, Jeremy Mao, Gordana Vunjak-Novakovic, Antonios G. Mikos, and Anthony Atala, editors Methods in Bioengineering Nanoscale Bioengineering and Nanomedicine Kaushal Rege Department of Chemical Engineering Arizona State University Igor L. Medintz Center for Biomolecular Science and Engineering U.S. Naval Research Laboratory Editors artechhouse.com Library of Congress Cataloging-in-Publication Data A catalog record for this book is available from the U. S. Library of Congress. British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library. ISBN-13: 978-1-59693-410-8 Text design by Darrell Judd Cover design by Igor Valdman © 2009 Artech House.