Pompe-Position-Statement.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

AHFS Pharmacologic-Therapeutic Classification System
AHFS Pharmacologic-Therapeutic Classification System Abacavir 48:24 - Mucolytic Agents - 382638 8:18.08.20 - HIV Nucleoside and Nucleotide Reverse Acitretin 84:92 - Skin and Mucous Membrane Agents, Abaloparatide 68:24.08 - Parathyroid Agents - 317036 Aclidinium Abatacept 12:08.08 - Antimuscarinics/Antispasmodics - 313022 92:36 - Disease-modifying Antirheumatic Drugs - Acrivastine 92:20 - Immunomodulatory Agents - 306003 4:08 - Second Generation Antihistamines - 394040 Abciximab 48:04.08 - Second Generation Antihistamines - 394040 20:12.18 - Platelet-aggregation Inhibitors - 395014 Acyclovir Abemaciclib 8:18.32 - Nucleosides and Nucleotides - 381045 10:00 - Antineoplastic Agents - 317058 84:04.06 - Antivirals - 381036 Abiraterone Adalimumab; -adaz 10:00 - Antineoplastic Agents - 311027 92:36 - Disease-modifying Antirheumatic Drugs - AbobotulinumtoxinA 56:92 - GI Drugs, Miscellaneous - 302046 92:20 - Immunomodulatory Agents - 302046 92:92 - Other Miscellaneous Therapeutic Agents - 12:20.92 - Skeletal Muscle Relaxants, Miscellaneous - Adapalene 84:92 - Skin and Mucous Membrane Agents, Acalabrutinib 10:00 - Antineoplastic Agents - 317059 Adefovir Acamprosate 8:18.32 - Nucleosides and Nucleotides - 302036 28:92 - Central Nervous System Agents, Adenosine 24:04.04.24 - Class IV Antiarrhythmics - 304010 Acarbose Adenovirus Vaccine Live Oral 68:20.02 - alpha-Glucosidase Inhibitors - 396015 80:12 - Vaccines - 315016 Acebutolol Ado-Trastuzumab 24:24 - beta-Adrenergic Blocking Agents - 387003 10:00 - Antineoplastic Agents - 313041 12:16.08.08 - Selective -
WO 2017/173059 Al 5 October 2017 (05.10.2017) P O P C T
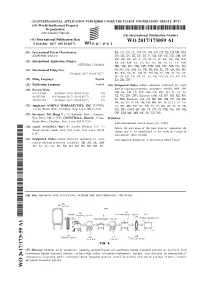
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization I International Bureau (10) International Publication Number (43) International Publication Date WO 2017/173059 Al 5 October 2017 (05.10.2017) P O P C T (51) International Patent Classification: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DJ, DK, DM, C12N 9/26 (2006.01) DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KH, KN, (21) International Application Number: KP, KR, KW, KZ, LA, LC, LK, LR, LS, LU, LY, MA, PCT/US20 17/024981 MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, (22) International Filing Date: NI, NO, NZ, OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, 30 March 2017 (30.03.2017) RU, RW, SA, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, (25) Filing Language: English ZA, ZM, ZW. (26) Publication Language: English (84) Designated States (unless otherwise indicated, for every (30) Priority Data: kind of regional protection available): ARIPO (BW, GH, 62/3 15,400 30 March 2016 (30.03.2016) US GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, 62/457,584 10 February 2017 (10.02.2017) US TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, 15/473,994 30 March 2017 (30.03.2017) US TJ, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, (71) Applicant: AMICUS THERAPEUTICS, INC. -

Enzyme Replacement Therapy Srx-0019 Policy Type ☒ Medical ☐ Administrative ☐ Payment
MEDICAL POLICY STATEMENT Original Effective Date Next Annual Review Date Last Review / Revision Date 06/15/2011 03/15/2017 10/04/2016 Policy Name Policy Number Enzyme Replacement Therapy SRx-0019 Policy Type ☒ Medical ☐ Administrative ☐ Payment Medical Policy Statements prepared by CSMG Co. and its affiliates (including CareSource) are derived from literature based on and supported by clinical guidelines, nationally recognized utilization and technology assessment guidelines, other medical management industry standards, and published MCO clinical policy guidelines. Medically necessary services include, but are not limited to, those health care services or supplies that are proper and necessary for the diagnosis or treatment of disease, illness, or injury and without which the patient can be expected to suffer prolonged, increased or new morbidity, impairment of function, dysfunction of a body organ or part, or significant pain and discomfort. These services meet the standards of good medical practice in the local area, are the lowest cost alternative, and are not provided mainly for the convenience of the member or provider. Medically necessary services also include those services defined in any Evidence of Coverage documents, Medical Policy Statements, Provider Manuals, Member Handbooks, and/or other policies and procedures. Medical Policy Statements prepared by CSMG Co. and its affiliates (including CareSource) do not ensure an authorization or payment of services. Please refer to the plan contract (often referred to as the Evidence of Coverage) for the service(s) referenced in the Medical Policy Statement. If there is a conflict between the Medical Policy Statement and the plan contract (i.e., Evidence of Coverage), then the plan contract (i.e., Evidence of Coverage) will be the controlling document used to make the determination. -

BCBSVT Specialty Drug List Effective 2021.07.01.Xlsx
Effective Date: 07/01/2021 SPECIALTY DRUG LIST Revised Date: 05/07/2021 DOSAGE EXCLUDED ON NATIONAL DRUG CLASS DRUG NAME GENERIC NAME FORM PERFORMANCE FORMULARY ANEMIA ARANESP SOLN DARBEPOETIN ALFA SOLN INJ ANEMIA ARANESP SOSY DARBEPOETIN ALFA SOLN PREFILLED SYRINGE ANEMIA EPOGEN SOLN EPOETIN ALFA INJ X ANEMIA PROCRIT SOLN EPOETIN ALFA INJ X ANEMIA REBLOZYL SOLR LUSPATERCEPT-AAMT FOR SUBCUTANEOUS INJ ANEMIA RETACRIT SOLN EPOETIN ALFA-EPBX INJ ANTI-GOUT AGENT KRYSTEXXA SOLN PEGLOTICASE INJ (FOR IV INFUSION) ANTI-INFECTIVE PREVYMIS SOLN LETERMOVIR IV SOLN ANTI-INFECTIVE PREVYMIS TABS LETERMOVIR TAB ASTHMA CINQAIR SOLN RESLIZUMAB IV INFUSION SOLN ASTHMA FASENRA SOSY BENRALIZUMAB SUBCUTANEOUS SOLN PREFILLED SYRINGE ASTHMA FASENRA PEN SOAJ BENRALIZUMAB SUBCUTANEOUS SOLN AUTO-INJECTOR ASTHMA NUCALA SOAJ MEPOLIZUMAB SUBCUTANEOUS SOLUTION AUTO-INJECTOR ASTHMA NUCALA SOLR MEPOLIZUMAB FOR INJ ASTHMA NUCALA SOSY MEPOLIZUMAB SUBCUTANEOUS SOLUTION PREF SYRINGE ASTHMA XOLAIR SOLR OMALIZUMAB FOR INJ ASTHMA XOLAIR SOSY OMALIZUMAB SUBCUTANEOUS SOLN PREFILLED SYRINGE CARDIOVASCULAR VYNDAMAX CAPS TAFAMIDIS CAP CARDIOVASCULAR VYNDAQEL CAPS TAFAMIDIS MEGLUMINE (CARDIAC) CAP CENTRAL NERVOUS SYSTEM AGENTS AUSTEDO TABS DEUTETRABENAZINE TAB CENTRAL NERVOUS SYSTEM AGENTS ENSPRYNG SOSY SATRALIZUMAB-MWGE SUBCUTANEOUS SOLN PREF SYRINGE CENTRAL NERVOUS SYSTEM AGENTS HETLIOZ CAPS TASIMELTEON CAPSULE CENTRAL NERVOUS SYSTEM AGENTS HETLIOZ LQ SUSP TASIMELTEON ORAL SUSP CHEMOTHERAPY PROTECTANT AMIFOSTINE SOLR AMIFOSTINE CRYSTALLINE FOR INJ CHEMOTHERAPY PROTECTANT ELITEK -

Cipaglucosidase Alfa/Miglustat Phase 3 PROPEL Results
AT-GAA (ATB200/AT2221) Phase 3 PROPEL Topline Results February 11, 2021 Phase 3 PROPEL Topline Results 2 Forward-Looking Statements This presentation contains "forward-looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995, including statements relating to top-line data from a global Phase 3 study to investigate AT-GAA for the treatment of Pompe Disease and the potential implications on these data for the future advancement and development of AT-GAA. Words such as, but not limited to, “look forward t o ,” “believe,” “expect,” “anticipate,” “estimate,” “intend,” "confidence," "encouraged," “potential,” “plan,” “targets,” “likely,” “may,” “will,” “would,” “should” and “c o u l d ,” and similar expressions or words identify forward-looking statements. The forward looking statements included in this press release are based on management's current expectations and belief's which are subject to a number of risks, uncertainties and factors, including that the Company will not be able to successfully complete the development of, obtain regulatory approval for, or successfully manufacture and commercialize AT-GAA. In addition, all forward looking statements are subject to the other risks and uncertainties detailed in our Annual Report on Form 10-K for the year ended December 31, 2019 and Quarterly Report on 10-Q for the Quarter ended September 30, 2020. As a consequence, actual results may differ materially from those set forth in this press release. You are cautioned not to place undue reliance on these forward looking statements, which speak only of the date hereof. All forward looking statements are qualified in their entirety by this cautionary statement and we undertake no obligation to revise this press release to reflect events or circumstances after the date hereof. -

Myozyme, INN-Alglucosidase Alfa
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Myozyme 50 mg powder for concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION One vial contains 50 mg of alglucosidase alfa. After reconstitution, the solution contains 5 mg of alglucosidase alfa* per ml and after dilution, the concentration varies from 0.5 mg to 4 mg/ml. *Human acid α-glucosidase is produced in Chinese hamster ovary cells (CHO) by recombinant DNA technology. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Powder for concentrate for solution for infusion. White to off-white powder. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Myozyme is indicated for long-term enzyme replacement therapy (ERT) in patients with a confirmed diagnosis of Pompe disease (acid -glucosidase deficiency). Myozyme is indicated in adults and paediatric patients of all ages. 4.2 Posology and method of administration Myozyme treatment should be supervised by a physician experienced in the management of patients with Pompe disease or other inherited metabolic or neuromuscular diseases. Posology The recommended dose regimen of alglucosidase alfa is 20 mg/kg of body weight administered once every 2 weeks. Patient response to treatment should be routinely evaluated based on a comprehensive evaluation of all clinical manifestations of the disease. Paediatric and older people There is no evidence for special considerations when Myozyme is administered to paediatric patients of all ages or older people. Patients with renal and hepatic impairment The safety and efficacy of Myozyme in patients with renal or hepatic impairment have not been evaluated and no specific dose regimen can be recommended for these patients. -

Vivian Oh, Et Al. V. Genzyme Corporation, Et Al. OH-Class Action
UNITED STATES DISTRICT COURT DISTRICT OF MASSACHUSETTS VIVIAN OH, Individually and on Behalf of No. All Others Similarly Situated, Plaintiff, v. GENZYME CORPORATION and HENRI A. TERMEER, Defendants. CLASS ACTION COMPLAINT AND JURY TRIAL DEMAND Plaintiff Vivian Oh, by and through her attorneys, alleges the following upon information and belief, except as to those allegations concerning Plaintiff, which are alleged upon personal knowledge. Plaintiff's information and belief is based upon, among other things, her counsel’s investigation, which includes without limitation: (a) review and analysis of regulatory filings made by Genzyme Corporation (“Genzyme ” or the “Company”) with the United States Securities and Exchange Commission (“SEC”); (b) review and analysis of press releases and media reports issued by and disseminated by Genzyme ; and (c) review of other publicly available information concerning Genzyme . Plaintiff believes that substantial additional evidentiary support will exist for the allegations set forth herein after a reasonable opportunity for discovery. NATURE OF THE ACTION 1. This is a securities class action brought by Plaintiff Vivian Oh (“Plaintiff”) on behalf of all purchasers (the “Class”) of the common stock of Genzyme Corporation (“Genzyme” or the “Company”) between June 26, 2008 and July 21, 2009, inclusive (the “Class Period”) seeking to pursue remedies under the Securities Exchange Act of 1934 (the “Exchange Act”). 2. Defendant Genzyme is a leading biotechnology company based in Cambridge, Massachusetts. The Company -

Enzyme Replacement LSD Combined Policy
MEDICAL POLICY STATEMENT Original Effective Date Next Annual Review Date Last Review / Revision Date 06/15/2011 02/15/2016 11/17/2015 Policy Name Policy Number Enzyme Replacement Therapy and Agents SRx-0019 Medical Policy Statements prepared by CSMG Co. and its affiliates (including CareSource) are derived from literature based on and supported by clinical guidelines, nationally recognized utilization and technology assessment guidelines, other medical management industry standards, and published MCO clinical policy guidelines. Medically necessary services include, but are not limited to, those health care services or supplies that are proper and necessary for the diagnosis or treatment of disease, illness, or injury and without which the patient can be expected to suffer prolonged, increased or new morbidity, impairment of function, dysfunction of a body organ or part, or significant pain and discomfort. These services meet the standards of good medical practice in the local area, are the lowest cost alternative, and are not provided mainly for the convenience of the member or provider. Medically necessary services also include those services defined in any Evidence of Coverage documents, Medical Policy Statements, Provider Manuals, Member Handbooks, and/or other policies and procedures. Medical Policy Statements prepared by CSMG Co. and its affiliates (including CareSource) do not ensure an authorization or payment of services. Please refer to the plan contract (often referred to as the Evidence of Coverage) for the service(s) referenced in the Medical Policy Statement. If there is a conflict between the Medical Policy Statement and the plan contract (i.e., Evidence of Coverage), then the plan contract (i.e., Evidence of Coverage) will be the controlling document used to make the determination. -

Estonian Statistics on Medicines 2016 1/41
Estonian Statistics on Medicines 2016 ATC code ATC group / Active substance (rout of admin.) Quantity sold Unit DDD Unit DDD/1000/ day A ALIMENTARY TRACT AND METABOLISM 167,8985 A01 STOMATOLOGICAL PREPARATIONS 0,0738 A01A STOMATOLOGICAL PREPARATIONS 0,0738 A01AB Antiinfectives and antiseptics for local oral treatment 0,0738 A01AB09 Miconazole (O) 7088 g 0,2 g 0,0738 A01AB12 Hexetidine (O) 1951200 ml A01AB81 Neomycin+ Benzocaine (dental) 30200 pieces A01AB82 Demeclocycline+ Triamcinolone (dental) 680 g A01AC Corticosteroids for local oral treatment A01AC81 Dexamethasone+ Thymol (dental) 3094 ml A01AD Other agents for local oral treatment A01AD80 Lidocaine+ Cetylpyridinium chloride (gingival) 227150 g A01AD81 Lidocaine+ Cetrimide (O) 30900 g A01AD82 Choline salicylate (O) 864720 pieces A01AD83 Lidocaine+ Chamomille extract (O) 370080 g A01AD90 Lidocaine+ Paraformaldehyde (dental) 405 g A02 DRUGS FOR ACID RELATED DISORDERS 47,1312 A02A ANTACIDS 1,0133 Combinations and complexes of aluminium, calcium and A02AD 1,0133 magnesium compounds A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 811120 pieces 10 pieces 0,1689 A02AD81 Aluminium hydroxide+ Magnesium hydroxide (O) 3101974 ml 50 ml 0,1292 A02AD83 Calcium carbonate+ Magnesium carbonate (O) 3434232 pieces 10 pieces 0,7152 DRUGS FOR PEPTIC ULCER AND GASTRO- A02B 46,1179 OESOPHAGEAL REFLUX DISEASE (GORD) A02BA H2-receptor antagonists 2,3855 A02BA02 Ranitidine (O) 340327,5 g 0,3 g 2,3624 A02BA02 Ranitidine (P) 3318,25 g 0,3 g 0,0230 A02BC Proton pump inhibitors 43,7324 A02BC01 Omeprazole -

Treatment Protocol – Information for Healthcare Professionals
Early Access to Medicines Scheme – Treatment protocol – Information for healthcare professionals Introduction The aim of the Early Access to Medicines Scheme (EAMS) is to provide earlier availability of promising new unlicensed medicines and medicines used outside their licence, to UK patients that have a high unmet clinical need. The medicinal products included in the scheme are those that are intended to treat, diagnose or prevent seriously debilitating or life- threatening conditions where there are no adequate treatment options. More information about the scheme can be found here: http://www.mhra.gov.uk/Howweregulate/Innovation/EarlyaccesstomedicinesschemeEAMS/in dex.htm This information is intended for healthcare professionals and is provided by the pharmaceutical company that manufactures the EAMS medicine. This medicine does not yet have a licence (marketing authorisation) and is to be used in combination with (an)other medicine(s) prescribed outside their licence. The information is provided to assist physicians in prescribing unlicensed medicines. Guidance on prescribing unlicensed medicines can be found on the GMC webpage: https://www.gmc-uk.org/guidance/ethical_guidance/14327.asp The scientific opinion is based on assessment of the information supplied to the MHRA on the benefits and risks of this promising new medicine used in combination therapy. As such, this is a scientific opinion and should not be regarded as a medicine licensed by the MHRA or a future commitment by the MHRA to license such a medicine, nor should it be regarded as an authorisation to sell or supply such a medicine. A positive scientific opinion is not a recommendation for use of the medicine and should not be interpreted as such. -

Lists of Medicinal Products for Rare Diseases in Europe*
March 2021 Lists of medicinal products for rare diseases in Europe* the www.orpha.net www.orphadata.org General Table of contents PART 1: List of orphan medicinal products in Europe with European orphan designation and European marketing authorization 3 Table of contents 3 Methodology 3 Classification by tradename 5 Annex 1: Orphan medicinal products withdrawn from the European Community Register of orphan medicinal products 22 Annex 2: Orphan medicinal products withdrawn from use in the European Union 31 Classification by date of MA in descending order 33 Classification by ATC category 34 Classification by MA holder 35 PART 2 : 37 List of medicinal products intended for rare diseases in Europe with European marketing authorization without an orphan designation in Europe 37 Table of contents 37 Methodology 37 Classification by tradename 38 Classification by date of MA in descending order 104 Classification by ATC category 106 Classification by MA holder 108 For any questions or comments, please contact us: [email protected] Orphanet Report Series - Lists of medicinal products for rare diseases in Europe. March 2021 http://www.orpha.net/orphacom/cahiers/docs/GB/list_of_orphan_drugs_in_europe.pdf 2 PART 1: List of orphan medicinal products in Europe with European orphan designation and European marketing authorization* Table of contents List of orphan medicinal products in Europe with European orphan designation and European marketing authorisation* 3 Methodology 3 Classification by tradename 5 Annex 1: Orphan medicinal products removed or withdrawn from the European Community Register of orphan medicinal products 22 Annex 2: Orphan medicinal products withdrawn from use in the European Union 31 Classification by date of MA in descending order 33 Classification by ATC category 34 Classification by MA holder 35 Methodology This part of the document provides the list of all orphan with the list of medicinal products that have been granted a medicinal products that have received a European Marketing marketing authorization (http://ec.europa. -

May2013 CPG Updates
New Drugs May 2013 (Original New Drug Applications: FDA) Generic Name Trade Name Indication(s) CPG Action/Date January 2013 Icosapent Ethyl Vascepa Cardiovascular Agents: 5/20/13 Antihyperlipidemic Agents. CTP holder may Indicated as an adjunct prescribe. to diet to reduce triglyceride levels in adult patients with severe (500mg/dL or more) Formulary Pg. 12 hypertriglyceridemia. Linaclotide Linzess Gastrointestinal Agents: 5/20/13 Linaclotide. Indicated for the CTP holder may treatment of chronic prescribe. idiopathic constipation in adults and for the treatment of irritable bowel syndrome with Formulary Pg. 21 constipation in adults. Teriflunomide Aubagio Biologic/ Immunologic 5/20/13 Agents: Immunologic Agents: Physician Initiated/ Immunomodulators. Physician Consult Indicated for the treatment of patients with relapsing forms of Formulary Pg. 24 multiple sclerosis. February 2013 Vitamin A Palmitate Aquasol Nutrients & Nutritional 5/20/13 Injection Agents: Vitamins. Indicated for the CTP holder may treatment of vitamin A prescribe. Formulary Pg. 5 deficiency. Perampanel Fycompa Central Nervous System 5/20/13 Agents: Anticonvulsants: Adjuvant Physician Initiated/ Anticonvulsants. Physician Consult Indicated as an adjunctive therapy for the treatment of partial- onset seizures with or without secondarily Formulary Pg. 19 generalized seizures in 1 CPG Updates May 2013 patients with epilepsy who are 12 years and older. Regorafenib Stivarga Antineoplastic Agents: 5/20/13 Kinase Inhibitors. Indicated for the CTP holder May treatment of patients NOT prescribe. with metastatic colorectal cancer who have been previously treated with fluoropyrimidine-, oxaliplatin-, and irinotecan-based chemotherapy, an antivascular endothelial growth factor (VEGF) therapy, and, if KRAS wild type, an antiepidermal growth factor receptor (EGFR) Formulary Pg.