Thursday 28 June 2018 the Committee Will
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Initial Template
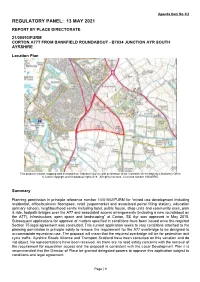
Agenda Item No 3/2 REGULATORY PANEL: 13 MAY 2021 REPORT BY PLACE DIRECTORATE 21/00093/FURM CORTON A77T FROM BANKFIELD ROUNDABOUT - B7034 JUNCTION AYR SOUTH AYRSHIRE Location Plan This product includes mapping data licensed from Ordnance Survey with permission of the Controller of Her Majesty’s Stationery Office. © Crown copyright and/or database right 2018. All rights reserved. Licenced number 100020765. Summary Planning permission in principle reference number 14/01552/FURM for “mixed use development including residential, office/business floorspace, retail (supermarket and associated petrol filling station), education (primary school), neighbourhood centre including hotel, public house, shop units and community uses, park & ride, footpath bridges over the A77 and associated access arrangements (including a new roundabout on the A77), infrastructure, open space and landscaping” at Corton, SE Ayr was approved in May 2015. Subsequent applications for approval of matters specified in conditions have been issued once the required Section 75 legal agreement was concluded. This current application seeks to vary conditions attached to the planning permission in principle solely to remove the requirement for the A77 overbridge to be designed to accommodate equestrian use. The proposal will mean that the required overbridge will be for pedestrian and cycle traffic. Ayrshire Roads Alliance and Transport Scotland have been consulted on this variation and do not object. No representations have been received. As there are no road safety concerns with the removal of the requirement for equestrian access and the proposal is consistent with the Local Development Plan it is recommended that the Director of Place be granted delegated powers to approve this application subject to conditions and legal agreement. -

Hotel for Sale
HOTEL FOR SALE HOTEL WITH RESIDENTIAL DEVELOPMENT POTENTIAL Royal Hotel, 57 King Street, Crosshill, KA19 7RE Attractive village setting close to Ayr and Turnberry Licensed hotel premises with 6 bedrooms, bar and function suite Planning permission for residential conversion 100% rates relief, subject to status Offers of £165,000 are invited Commercial Department 15 Miller Road, Ayr, KA7 2AX dmhall.co.uk 01292 268055 LOCATION Crosshill is an attractive rural village within the South Ayrshire region, located around 11 miles south of Ayr and 3 miles south east of Maybole where there is a railway station and connection on to the A77 road route, which extends north to Ayr and Glasgow (48 miles). Turnberry Golf Course is 10 miles distant with two further wedding venues nearby King Street is the main thoroughfare running through the village and an established residential area, with 57 King Street positioned on the west side of the street with a rural outlook to the rear. DESCRIPTION The ‘Royal Hotel’ is an end terraced, two-storey property dating from the 19th century that has been extended in the more recent past to form a now closed but licensed hotel with private car parking. The building is of traditional construction with stone outer walls and a slate roof to the main building and contains the following accommodation: Ground Floor Public Bar with servery and back store Dining Room Supper Room/Snug Function Suite Kitchen Cellar Male and Female Toilets First Floor 6 letting bedrooms Lounge 2 Bathrooms Kitchenette Planning permission was obtained in 2007 under reference 07/00507/COU and renewed in 2015 under reference 15/01109/ FUR for the conversion of the property to form a single residential dwelling. -

East Ayrshire Council Planning Committee: 23 June
EAST AYRSHIRE COUNCIL PLANNING COMMITTEE: 23 JUNE 2017 17/0139/PPP PROPOSED RESIDENTIAL DEVELOPMENT OF APPROXIMATELY 550 DWELLINGS AND ASSOCIATED WORKS APPLICATION BY MR JOHN GARDNER AT TREESBANK KILMARNOCK EAST AYRSHIRE KA1 5LP Report by Head of Planning and Economic Development Economy and Skills Click for Application Details: http://eplanning.eastayrshire.gov.uk/online/applicationDetails.do?activeTab=summary&k eyVal=OLU33QGFILC00 EXECUTIVE SUMMARY SHEET PURPOSE OF REPORT 1. The purpose of this report is to present for determination an application for planning permission in principle which is to be considered by the Planning Committee under the scheme of delegation as it a major development, in terms of the Town and Country Planning (Hierarchy of Development) (Scotland) Regulations 2009, which would also require to be determined by Planning Committee. RECOMMENDATION 2. It is recommended that the application be refused subject to the reasons listed on the attached sheet. CONTRARY DECISION NOTE 3 Should the Committee agree that the application be refused on principle of the development, contrary to the recommendation of the Head of Planning and Economic Development the application will require to be referred to the Council because that would represent a significant departure from the local development plan. However if Members agree that the application be refused for the reasons detailed in the report, the application will not require to be referred to the Council because that would not represent a significant departure from the local development plan. Michael Keane Head of Planning and Economic Development Note: This document combines key sections of the associated report for quick reference and should not in itself be considered as having been the basis for recommendation preparation or decision making by the Planning Authority. -

THE A77 TRUNK ROAD THROUGH MAYBOLE South Ayrshire Council's
THE A77 TRUNK ROAD THROUGH MAYBOLE South Ayrshire Council’s Proposals March 2005 The Ordnance Survey mapping/map data included within this publication is provided by South Ayrshire Council under licence from the Ordnance Survey in order to fulfil its public function to publicise local transport proposals. Persons viewing this mapping should contact Ordnance Survey copyright for advice where they wish to licence Ordnance Survey mapping/map data for their own use. South Ayrshire Council 100020765, 2005. EXECUTIVE SUMMARY The A77 through Maybole High Street carries traffic flows of up to 13000 vehicles a day. The street itself is particularly unsuited for this level of traffic being narrow and having narrow footways. This is particularly evident when heavy traffic from the ferries passes through. The A77 through Maybole is the link from southern Ayrshire, Stranraer and Ireland to Glasgow International Airport and Glasgow Prestwick International Airport. It is considered that the current A77 between Ayr and Stranraer is not of the appropriate standard. It fails to reach this standard on the grounds of safety, contribution to the economy of South Ayrshire and contribution to the effectiveness of the ferry links between Scotland and Ireland. South Ayrshire Council considers that the provision of an A77 Maybole Bypass would be a vital part of the necessary improvements to the A77, and would be a vital contribution to the future of the North Channel Link to both Northern Ireland and the Republic of Ireland. South Ayrshire Council also considers that the provision of an A77 Maybole Bypass would address many issues relating to the health, safety and environment for the Maybole Community. -
Standards and Quality Report Minishant Primary School 2019-2020
Standards and Quality Report Minishant Primary School 2019-2020 Introduction The purpose of this report is to provide you with clear evidence of how well our school has performed in the academic year 2019-2020. The report provides a variety of information about how well our pupils are attaining, the many successes we have had, the wide variety of experiences children can expect at Minishant Primary School and how they will benefit from learning here. Minishant is a village in South Ayrshire situated on the A77 road from Ayr to Stranraer. It is a rural school serving Minishant and its surrounding district. Children come to school by car, taxi or walk. At present (Aug 2020) the school roll is 32, with 28% placing requests into the school and 22% of children receiving free school meal entitlement. We currently have two full time class teachers, a 0.5 Principal Teacher and a 0.5 Head Teacher (who is shared with Crosshill Primary School), two school assistants (27.5 hours each), one janitor/cleaner, one catering assistant and one clerical assistant with 27.5 hours. The school is very well supported by Lynn Crossan, Quality Improvement Officer for South Ayrshire. This session we received a total of £9,516 PEF funding. This was used to continue the running of our very successful free breakfast club for all pupils to attend. Our School Assistant received additional hours to implement the breakfast club 5 mornings a week over the school year. The Breakfast Club has helped to keep our attendance figures above the authority average of 95% and has reduced our late comings over the past three years. -

Representation Issue Summary – Housing
Representation Summary – Housing Issues Consideration Recommendation Issue GIR3- Further options should be considered for the use of this site. Any development must not adversely impact on the residential The site is proposed for housing and is located within a predominantly residential area. The redevelopment of the No proposed modification to Girvan Housing amenity of Wilson Avenue. Any redevelopment needs to remediate the site without negative impact on surrounding residential brownfield site for residential purposes could have positive impact on the visual and residential amenity of LDP. Site @ Henrietta area due to previous use as gasworks. surrounding area. The allocation of the site for housing contributes to the Plan’s housing requirement. The impact Street (GIR3) of any development on surrounding amenity, and dealing with remediation from previous uses, which may have contaminated the site, can be dealt with at planning application stage. Support for sites MAYB1, 2 and 3 for residential development proposed allocation for a master plan led development at Maybole. None. No proposed modification to Maybole Housing Since the Proposed Local Development Plan was released for consultation, the joint developers have been securing market interest, LDP. Site @ Crosshill preparing a site master plan, meeting with Maybole Community Council and preparing a Accessibility Appraisal Report Road (MAYB1) Support for sites MAYB1, 2 and 3 for residential development proposed allocation for a master plan led development at Maybole. No further consideration given to supportive comments. No proposed modification to Maybole Housing Since the Proposed Local Development Plan was released for consultation, the joint developers have been securing market interest, LDP. -

Helenton View Symington
HELENTON VIEW SYMINGTON w w w . c o r u m p r o p e r t y . c o . u k T H E P R O P E R T Y 5 | B E D R O O M S 4 | B A T H R O O M S 3 | P U B L I C R O O M S A gorgeous bespoke family home surrounded by open countryside and presented to the market with an unrivalled level of luxury finishings and a remarkable amount of flexible modern living space. ‘Helenton View’ is a truly bespoke and stunning family home in an idyllic rural setting, with stylish, modern accommodation extending to approximately 320 square metres. The impressive architectual design utilises a contemporary amount of glass throughout to perfectly frame the views across rolling Ayrshire countryside and harness the natural light. The level of fixtures and fittings is luxurious, including sanitary ware by ‘Porcelanosa’, a custom kitchen with integrated appliances and extensive use of solid oak, including the doors, surrounds and a large part of the downstairs flooring. The peaceful setting is just seconds from the recently upgraded A77 road network, which links directly into Ayr, Prestwick and Glasgow City Centre via the M77. In more detail, the internal accommodation extends to a welcoming reception hallway, a lounge with a vaulted ceiling, a picture window, bi-folding doors out to the gardens and a feature double-sided fireplace, also through to the dining kitchen with a centre island and a separate utility room. There is a family bathroom suite, three large double bedrooms, two of which have en suite facilities and built-in wardrobes, and an irresistable master bedroom suite, with fitted wardrobes, a vaulted ceiling, a picture window and a large en suite shower room. -

1 to 1636 Approved-Traffic-Signs-1.Pdf
No. Date Council Subject Title 1 06/01/1987 Civic pride signs – Coldstream Berwickshire 2 19/01/1987 District and Regional boundary signs 3 19/01/1987 Twining signs for Ettrick – Lauderdale District 4 21/01/1987 Textured pavements at pedestrian crossings 5 19/06/1987 Traffic signal installation traffic signs, Dundee 6 09/02/1987 Warning signs for Deaf People Crossing 7 12/02/1987 Local Service signs for Gatehouse of fleet 8 24/02/1987 Signs for buses stopping on A74 Carlisle to Glasgow Trunk road Roadworks signing for M74 Hamilton / Motherwell / (Junction 6) to 9 26/02/1987 Lanark (Junction 7) 10 27/02/1987 Roadworks signing for Glasgow – Port Glasgow Trunk Road (M8) 11 17/03/1987 Roadworks signing on A74 (southbound) at Glengonnar 12 19/03/1987 Roadworks signing for A74 (Parkhall crossing to Maidengill crossing) 13 31/03/1987 Local Services signs for Blair Atholl – Bruar 14 31/03/1987 Revised signing for Kinross Service Area 15 06/04/1987 Pedestrian Symbol ( to be included in AM Direction signing 16 10/04/1987 Local Services sign for Moffat 17 10/04/1987 Emergency telephone and layby signposting on outer city bypass 18 06/05/1987 Roadworks signing on A74 19 22/04/1987 Roadworks signing on A74 trunk road at Paddy’s Rickle Vehicle excise checkpoint signs ( to be used in connection with 20 27/04/1987 Departments campaign against vehicle excise duty evaders) (Lothian) Vehicle excise checkpoint signs ( to be used in connection with 21 27/04/1987 Departments campaign against vehicle excise duty evaders) (Borders) 22 24/04/1987 Paved chevron -

Whithorn Way – Maybole to Girvan Route Directions
Whithorn Way – Maybole to Girvan Route Directions Grid Reference Directional Instructions Description NS 29938 10036 Starting from the Carrick Centre – Head west NS 29885 10011 Turn R onto Culzean Road (B7023) Pass Maybole Station on right. NS 29609 09959 Turn L into Whitefaulds Avenue NS 29420 09624 Left onto footpath and Right onto A77 footpath Walk west on the north side of the A77 to Crossraguel Abbey NS 27552 08400 Cross A77 with care and enter into car park Crossraguel Abbey, worth stopping for a tour. After visit return to above point and resume the walk in a SW direction alongside the A77 NS 27183 08376 “Y” junction, turn left off A77 onto minor road NS 26754 08091 “T” junction, straight ahead NS 26217 07828 Cross roads, straight ahead Near to Auchenblane and Middleridge NS 25390 07784 “Z” bend on minor road, remaining on the same minor road Blanefield buildings are on the south side NS 25092 07782 “T” junction, keeping straight ahead and heading SW NS 24659 07601 Minor road crosses ford. NS 24625 07600 “T” junction and turn R NS 24618 17641 Turn L off roadway onto track heading W NS 24541 07627 Joint the A77 and proceed on pavement WSW Walking into Kirkoswald NS 23880 07473 Left off A77 and head up Kirkbrae Kirkoswald Kirk and graveyard on the right. NS 23911 07355 Remain on Kirkbrae unless stopping at Church Kirkoswald Parish church and gardens off to left. NS 23992 07281 Kirkbrae now turns into country track heading SE NS 24093 07170 Cross over the Milton Burn remaining on the track NS 24394 06602 Track reaches minor road, turn right and west Junction of track and road close to Keekafar NS 23276 06718 Junction, turn left heading SW. -

A77 Symington and Bogend Toll Environmental Statement, January 2007 (ES)
A77 Symington and Bogend Toll Environmental Statement - Addendum 1. Introduction .......................................................................1 2. A77 Symington and Bogend Toll Scheme Description .2 2.1 Background to the Scheme ....................................................2 2.2 Purpose of the Environmental Statement .............................3 3. Scheme Changes ..............................................................5 4. Additional Assessment ....................................................8 5. Cumulative Impact ..........................................................11 APPENDICES.........................................................................12 Scott Wilson September 2008 A77 Symington and Bogend Toll Environmental Statement - Addendum 1. INTRODUCTION Scott Wilson was commissioned by Transport Scotland to prepare an Environmental Statement (ES) in accordance with the Environmental Impact Assessment (Scotland) Regulations 1999. This was published in January 2007 and is referred to as the A77 Symington and Bogend Toll Environmental Statement, January 2007 (ES). The main aims of the EIA process are: • To ensure that there will be a full consideration of the likely environmental effects of the Scheme in a way that enables both the importance of the environmental effects and the scope for mitigating these to be properly evaluated; and • To allow the public, statutory agencies and other bodies to comment on the proposals, taking account of their environmental concerns. Following ongoing consultation -

FOR SALE TOWN CENTRE PUB & OWNERS ACCOMMODATION ‘Cassillis Hotel’, 49-51 Cassillis Road, Maybole, KA19 7HF
LICENSED FOR SALE TOWN CENTRE PUB & OWNERS ACCOMMODATION ‘Cassillis Hotel’, 49-51 Cassillis Road, Maybole, KA19 7HF Highly visible position within Maybole Town Centre Licensed public house premises with rear function room Two vacant upper floors and owners accommodation Potential for development and alternative use, subject to consent Gross Internal Area 471 sq.m (5,095 sq.ft) 100% rates relief, subject to status Offers over £110,000 are invited Commercial Department 15 Miller Road, Ayr, KA7 2AX dmhall.co.uk 01292 268055 LOCATION The public house fronts on to Cassillis Road and Cassillis Road is the main road running through is broadly rectangular in shape and well-presented Maybole and forms part of the A77 road route, which comprising of a main bar, a games area and a timber extends north to Ayr (8 miles), Kilmarnock (23 miles) built bar servery with gantry. There is a hatch access to and beyond to Glasgow (44 miles). The surrounding the basement beer cellar and store. The rear function area is mixed commercial and residential in its nature suite has independent access off St Cuthbert Street with the subjects occupying aprominent corner position together with an internal linking corridor and is also well at the junction of Cassillis Road and St Cuthbert Street. presented having its own bar servery. The ground floor contains male and female toilets in addition to a kitchen Maybole has a population of around 4,700 persons with area. limited amenities. The railway station serving the town has services to Ayr, Glasgow and Stranraer. The former hotel consists of four former letting bedrooms and bathroom at first floor level and a further two bedrooms at attic floor level. -

7. Landscape Effects
Project Name: A77 Maybole Bypass Document Title: Environmental Statement: Volume 1 - Statement 7. Landscape Effects 7.1. Introduction 7.1.1. This section of the report outlines the assessment undertaken of the potential impacts on the landscape of the study area and on the visual impacts of the Scheme. 7.1.2. The objective of this section is to identify the potential impacts of the scheme on the character and individual elements of the landscape within the route corridor, and on the quality of the views. It will also assess the visual impacts on identified “receptors” – mainly residents in this case. 7.1.3. The technique of landscape and visual impact assessment (LVIA) is used to assess the impact of change on the landscape. It is used to help locate and integrate the proposed scheme, such that negative landscape impacts are avoided, reduced or offset. The two aspects of the assessment - landscape and visual impacts - are independent but related. 7.2. Methodology 7.2.1. The assessment of landscape impact was carried out in accordance with Design Manual for Roads and Bridges (DMRB) (Volume 11, Section 3, Part 5) – Landscape Effects13. However, additional reference was also made to the Guidelines for Landscape and Visual Impact Assessment (2013)14 (GLVIA). Determination of landscape and visual sensitivity, magnitude of impact and impact significance was assessed in accordance with Tables 1 - 6 within Appendix E1. 7.2.2. Landscape assessment in relation to road proposals consists initially of the collection of baseline data relating to the components, and quality of the landscape of the study area, followed by an assessment of the likely impact of the proposals and of the significance of these impacts.