Nutrition Profile-Qambar Shahdadkot
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

China-Pakistan Economic Corridor
U A Z T m B PEACEWA RKS u E JI Bulunkouxiang Dushanbe[ K [ D K IS ar IS TA TURKMENISTAN ya T N A N Tashkurgan CHINA Khunjerab - - ( ) Ind Gilgit us Sazin R. Raikot aikot l Kabul 1 tro Mansehra 972 Line of Con Herat PeshawarPeshawar Haripur Havelian ( ) Burhan IslamabadIslamabad Rawalpindi AFGHANISTAN ( Gujrat ) Dera Ismail Khan Lahore Kandahar Faisalabad Zhob Qila Saifullah Quetta Multan Dera Ghazi INDIA Khan PAKISTAN . Bahawalpur New Delhi s R du Dera In Surab Allahyar Basima Shahadadkot Shikarpur Existing highway IRAN Nag Rango Khuzdar THESukkur CHINA-PAKISTANOngoing highway project Priority highway project Panjgur ECONOMIC CORRIDORShort-term project Medium and long-term project BARRIERS ANDOther highway IMPACT Hyderabad Gwadar Sonmiani International boundary Bay . R Karachi s Provincial boundary u d n Arif Rafiq I e nal status of Jammu and Kashmir has not been agreed upon Arabian by India and Pakistan. Boundaries Sea and names shown on this map do 0 150 Miles not imply ocial endorsement or 0 200 Kilometers acceptance on the part of the United States Institute of Peace. , ABOUT THE REPORT This report clarifies what the China-Pakistan Economic Corridor actually is, identifies potential barriers to its implementation, and assesses its likely economic, socio- political, and strategic implications. Based on interviews with federal and provincial government officials in Pakistan, subject-matter experts, a diverse spectrum of civil society activists, politicians, and business community leaders, the report is supported by the Asia Center at the United States Institute of Peace (USIP). ABOUT THE AUTHOR Arif Rafiq is president of Vizier Consulting, LLC, a political risk analysis company specializing in the Middle East and South Asia. -

List of Dehs in Sindh
List of Dehs in Sindh S.No District Taluka Deh's 1 Badin Badin 1 Abri 2 Badin Badin 2 Achh 3 Badin Badin 3 Achhro 4 Badin Badin 4 Akro 5 Badin Badin 5 Aminariro 6 Badin Badin 6 Andhalo 7 Badin Badin 7 Angri 8 Badin Badin 8 Babralo-under sea 9 Badin Badin 9 Badin 10 Badin Badin 10 Baghar 11 Badin Badin 11 Bagreji 12 Badin Badin 12 Bakho Khudi 13 Badin Badin 13 Bandho 14 Badin Badin 14 Bano 15 Badin Badin 15 Behdmi 16 Badin Badin 16 Bhambhki 17 Badin Badin 17 Bhaneri 18 Badin Badin 18 Bidhadi 19 Badin Badin 19 Bijoriro 20 Badin Badin 20 Bokhi 21 Badin Badin 21 Booharki 22 Badin Badin 22 Borandi 23 Badin Badin 23 Buxa 24 Badin Badin 24 Chandhadi 25 Badin Badin 25 Chanesri 26 Badin Badin 26 Charo 27 Badin Badin 27 Cheerandi 28 Badin Badin 28 Chhel 29 Badin Badin 29 Chobandi 30 Badin Badin 30 Chorhadi 31 Badin Badin 31 Chorhalo 32 Badin Badin 32 Daleji 33 Badin Badin 33 Dandhi 34 Badin Badin 34 Daphri 35 Badin Badin 35 Dasti 36 Badin Badin 36 Dhandh 37 Badin Badin 37 Dharan 38 Badin Badin 38 Dheenghar 39 Badin Badin 39 Doonghadi 40 Badin Badin 40 Gabarlo 41 Badin Badin 41 Gad 42 Badin Badin 42 Gagro 43 Badin Badin 43 Ghurbi Page 1 of 142 List of Dehs in Sindh S.No District Taluka Deh's 44 Badin Badin 44 Githo 45 Badin Badin 45 Gujjo 46 Badin Badin 46 Gurho 47 Badin Badin 47 Jakhralo 48 Badin Badin 48 Jakhri 49 Badin Badin 49 janath 50 Badin Badin 50 Janjhli 51 Badin Badin 51 Janki 52 Badin Badin 52 Jhagri 53 Badin Badin 53 Jhalar 54 Badin Badin 54 Jhol khasi 55 Badin Badin 55 Jhurkandi 56 Badin Badin 56 Kadhan 57 Badin Badin 57 Kadi kazia -
Monograph No 43.Pmd
IDSA Monograph Series No. 43 January 2015 State versus Nations in Pakistan Sindhi, Baloch and Pakhtun Responses to Nation Building Ashok Behuria State versus Nations in Pakistan | 1 IDSA Monograph Series No. 43 January 2015 State versus Nations in Pakistan Sindhi, Baloch and Pakhtun Responses to Nation Building Ashok K Behuria 2 | Ashok K Behuria Institute for Defence Studies and Analyses, New Delhi. All rights reserved. No part of this publication may be reproduced, sorted in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photo-copying, recording or otherwise, without the prior permission of the Institute for Defence Studies and Analyses (IDSA). ISBN: 978-93-82169-49-9 Disclaimer: The views expressed in this Monograph are those of the author and do not necessarily reflect those of the Institute or the Government of India. First Published: January 2015 Price: Rs. 240/- Published by: Institute for Defence Studies and Analyses No.1, Development Enclave, Rao Tula Ram Marg, Delhi Cantt., New Delhi - 110 010 Tel. (91-11) 2671-7983 Fax.(91-11) 2615 4191 E-mail: [email protected] Website: http://www.idsa.in Layout & Cover by: Vaijayanti Patankar, Geeta Printed at: M/S A. M. Offsetters A-57, Sector-10, Noida-201 301 (U.P.) Mob: 09810888667 E-mail: [email protected] State versus Nations in Pakistan | 3 Contents List of Abbreviations .................................................................. 5 Preface .............................................................................................. -
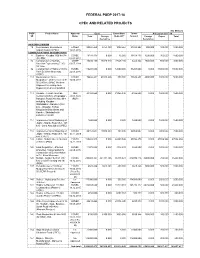
Federal Psdp 2017-18 Cpec and Related Projects
FEDERAL PSDP 2017-18 CPEC AND RELATED PROJECTS (Rs Million) PSDP Project Name Approval Cost Expenditure Throw- Allocation 2017-18 S# Status Total Foreign 30-06-2017 forward Foreign Rupee Total Assistance Assistance AVIATION DIVISION 10 New Gwadar International ECNEC 22247.450 2751.120 1023.567 21223.883 900.000 100.000 1000.000 Airport (NGIA) (CPEC) 12.01.2015 COMMUNICATIONS DIVISION (NHA) 77 Basima - Khuzdar (106 km) N- ECNEC 19188.435 0.000 10.000 19178.435 1200.000 300.000 1500.000 30 CPEC 07.03.2017 86 Construction of Burhan- CDWP 30494.150 25920.028 27045.286 3448.864 2500.000 500.000 3000.000 Havelian Expressway (E-35) 03.07.2014 59.1 Km 92 Construction of Hakla on M-I to ECNEC 110208.000 0.000 12000.000 98208.000 0.000 38000.000 38000.000 Yarik D.I.Khan Motorway 22.04.2016 (CPEC) 113 Dualization of Yarik - ECNEC 74486.231 63313.296 850.000 73636.231 4000.000 1000.000 5000.000 Mughalkot - Zhob section of N- 12.04.2017 50 (210 km) CPEC Western Alignment including Zhob Bypass and Land Acquisition 114 Gwadar - Turbat - Hoshab NHC 23168.660 0.000 31355.340 -8186.680 0.000 1500.000 1500.000 Section (200Km) of Gawadar - 25.03.1999 Ratodero Road (892 Km) M-8 (RUP) including Khuzdar - Shahdadkot - Ratodero (143 km) - (Gwadar, Turbat, Khuzdar in Balochistan and Kamber, Shahdadkot & Larkana in Sindh) 117 Improvement and Widening of 1500.000 0.000 0.000 1500.000 0.000 1500.000 1500.000 Jaglot - Skardu Road (S-1, 167 km) - Land Acquisition (CPEC) 118 Improvement and Widening of ECNEC 22154.037 19938.633 104.030 22050.007 0.000 7000.000 7000.000 Jaglot - Skardu Road (S-1, 167 03.11.2010 km) (CPEC) 124 Lahore-Abdul Hakeem Section ECNEC 150665.025 0.000 64880.546 85784.479 0.000 47006.984 47006.984 (230 km) (PKM) 14.11.2015 125 Land Acquisition , Affected ECNEC 11973.000 0.000 3342.941 8630.059 0.000 1000.000 1000.000 properties compensation for 22.04.2016 construction of Burhan-Hakla to D.I. -
PA00WFSG.Pdf
1 Table of Contents Acronyms ....................................................................................................... 3 Executive Summary ....................................................................................... 4 Component 1: Improved classroom learning environment for reading ........... 8 COMPONENT 2: Improved Policies and Systems for Reading ....................... 30 Component 3: Improved Community -Based Support for Reading ............... 47 Gender ......................................................................................................... 53 Communications .......................................................................................... 60 Monitoring & Evaluation .............................................................................. 68 Issues and Challenges in FY2018-19 ............................................................. 80 Annexures: .................................................................................................. 81 2 ACRONYMS ADE Associate Degree in Education MBL Mobile Bus Library ASI Adam Smith International MT Master Trainer AAEO Assistant Agency Education Officer MRC Material Review Committee AEO Agency Education Officer NACTE National Accreditation Council of Teacher Education AFAQ Association for Academic Quality NCC National Curriculum Council AJK Azad Jammu & Kashmir NGOs Non-Governmental Organizations AOR Agreement Office Representative NEAS National Education Assessment System B.Ed. (Hons.) Bachelors of Education (Honors) NGO Non-Government -

Balochistan Review” ISSN: 1810-2174 Publication Of: Balochistan Study Centre, University of Balochistan, Quetta-Pakistan
- I - vISSN: 1810-2174 Balochistan Review Volume XL No. 1, 2019 Recognized by Higher Education Commission of Pakistan Editor: Abdul Qadir Mengal BALOCHISTAN STUDY CENTRE UNIVERSITY OF BALOCHISTAN, QUETTA-PAKISTAN - II - Bi-Annual Research Journal “Balochistan Review” ISSN: 1810-2174 Publication of: Balochistan Study Centre, University of Balochistan, Quetta-Pakistan. @ Balochistan Study Centre 2019-1 Subscription rate in Pakistan: Institutions: Rs. 300/- Individuals: Rs. 200/- For the other countries: Institutions: US$ 15 Individuals: US$ 12 For further information please Contact: Abdul Qadir Mengal Assistant Professor & Editor Balochistan Review Balochistan Study Centre, University of Balochistan, Quetta-Pakistan. Tel: (92) (081) 9211255 Facsimile: (92) (081) 9211255 E-mail: [email protected] Website: www.uob.edu.pk/journals/bsc.htm No responsibility for the views expressed by authors and reviewers in Balochistan Review is assumed by the Editor, Assistant Editor, and the Publisher. - III - Editorial Board Patron in Chief: Prof. Dr. Javeid Iqbal Vice Chancellor, University of Balochistan, Quetta-Pakistan. Patron Prof. Dr. Abdul Haleem Sadiq Director, Balochistan Study Centre, UoB, Quetta-Pakistan. Editor Abdul Qadir Mengal Asstt Professor, International Realation Department, UoB, Quetta-Pakistan. Assistant Editor Dr. Waheed Razzaq Assistant Professor, Brahui Department, UoB, Quetta-Pakistan. Members: Prof. Dr. Andriano V. Rossi Vice Chancellor & Head Dept of Asian Studies, Institute of Oriental Studies, Naples, Italy. Prof. Dr. Saad Abudeyha Chairman, Dept. of Political Science, University of Jordon, Amman, Jordon. Prof. Dr. Bertrand Bellon Professor of Int’l, Industrial Organization & Technology Policy, University de Paris Sud, France. Dr. Carina Jahani Inst. of Iranian & African Studies, Uppsala University, Sweden. Prof. Dr. Muhammad Ashraf Khan Director, Taxila Institute of Asian Civilizations, Quaid-i-Azam University Islamabad, Pakistan. -
I I I I I I I I I I I I I
t t National Highway Authority I (Procurement and Contract Administration Section) 28 Mauve Area, Sector G'911, Islamabad (Pakistan| I Phone: +92-5L-9O32727, Fax: +92-5 L'926O4L9 I I I FRi[no"v*i$r.,.,Avs I DOCUMENTS FOR SUBMISSION t TO I PUBLIC PROCUREMENT REGULATORY I AUTHORITY I FOR I CoTvSULTANCYSPNVTCES FOR FPESTBILITY Stupv AND Dpterupn Dpstclv F'oR I COnUSTRUCTIONOF ItrOSHAts-AWARAN- I KnuzpAR SEcrIoN oF M-S (4OO KMI {2- Lnups Roen! I I Augqst,,2O2O I t I I I t ATTACHMENT- I (See regulation 2) PUBLICPROGUREMENT REGULATORY AUTHORITY (PPRA) I GONTRACTAWARD PROFORMA . I To Be FilledAnd Uploadedon PPRAWebsite in Respectof All PublicContracts of Works, I Services& GoodsWorth FiftvMillion or more NAMEOF THE ORGANIZATION/DEPTT. National Highway Authority I FEOEMUPROVINCIALGOVT. FederalGovt (Autonomous Body) TITLEOF CONTRACT Consultancy Services for Feasibility Study and Detailed Design for Construction of Hoshab-Awaran-Khuzdar Sectionof M-8 (400 Km) (2-Lanes I Road) TENDERNUMBER 6(4s1) BRIEFDESCRIPTION OF THE CONTMCT Gwadar Ratoder Road project (M-8) located in Baluchistan & Sindh provinces. I The sections of M-8 from Gwadar to Hoshab and Ratoder to Khuzdar have been constructed. However, the section from Hoshab-Awaran-Khuzdar (400 km) is still required to be constructed.The existing track from Hoshab to Awaran (100km),is being maintainedby provincialB&R department.The width of track is about 4 to 6m. The existing alignment runs through flat terrain having I ground. natural undulation in the The existing route from Awaran to Khuzdar (300 km) comprises shingle and kacha track. The road alignment passes through valleys and along parallel to Mashkai river after crossing the river, road moves toward Khuzdar. -

Kamber Shahdadkot 25
Kamber Shahdadkot - Risk Analysis Map July, 2014 Legend J h a l J a f f a r a b a d J a c o b a b a d Settlements at risk J h a l Jamali 7: Risk Assessment Map Jamali Branch Canals M a g s i SHAHDAD M a g s i Canals Saifullah Magsi Branch KOT Shahdad Kot Branch Qubo Aitbar Indus River Saeed Khan S h i k a r p h u r Roads Khan Hazar Chandio SIJAWAL Railway Wah JUNEJO Dhingano BALOCHISTAN Mahesar Hazar Shahdadkot 03 Maximum Flood Risk (2010-12) Bagodero Sijawal Ratodero Branch Wah Hazar Tharo Province boundary Bagodero QUBO Wah Wadho SAEED District boundary Karira War Taluka boundary KHAN hori Bra ah Branch K h u z d a r Khabar Ch nch MIRO Chousul UC boundary Bahram K Mirokhan KHAN oo r D a t Noor Wah o Dost Ali B B S ra ra h | n nc a S h a h d a d ch h h H KAMBAR a mir Bran Kalar Kamber-3 ch ALI KHAN Ghar Bra K o t Jian nch Abro Map Doc Name: iMMAP_PAK_K-ShahdadKot Risk Analysis Map_v02_071414 Buhar Ber Creation Date: July 14, 2014 a Projection/Datum: WGS84 Na r Br n ch Gaibidero Khandu si Web Resources: http://www.immap.org Laloo L a r k a n a DISTRICT KAMBERSHAHDADKOT Wagan er Rounak Ganhw Bra SINDH nch 0 5 10 20 Kilometers h c Warah Abad n a r B Map data source(s): Chillo Rice Canal Alhassan Systems Private Limited : Admin boundaries WARAH Dera Logistic Cluster-World Food Program: Roads Mirpur National Geospatial Agency: Settlements Gaji Sindh Irrigation and Drainage Authority (SIDA) : Rivers, Lakhu Muradi Canals, Branch Khunawar MODIS: Maximum Flood Extent NASIRABAD ASTER G-DEM: Digital Elevation Model Miandad Disclaimers: rao Branch Chinjini The designations employed and the presentation of material Dham on this map do not imply the expression of any opinion whatsoever on the part of the iMMAP, Alhasan Systems, or h Ga c USAID concerning the legal status of any country, territory, njrot Bra n h city or area or of its authorities, or concerning the delimitation Ra c Indus River j Wah Branch an of its frontiers or boundaries. -

NATIONAL DRAINAGE PROGRAM (NDP) PROJECT Sindh Province 35° 35° N.W.F.P
65° UZBEK. 70° 75° TAJIKISTAN CHINA TAJIK. PAKISTAN TURKMENISTAN NATIONAL DRAINAGE PROGRAM (NDP) PROJECT Sindh Province 35° 35° N.W.F.P. Approx. Line Peshawar of Control AFGHANISTAN CULTURAL SITES MENTIONED IN REQUEST JAMMU SELECTED BASIN BOUNDARIES ISLAMABAD AND KASHMIR DHANDS AND LAGOONS MENTIONED IN REQUEST DESERTS/HILLS WEIRS/BARRAGES MENTIONED IN REQUEST SELECTED TOWNS Lahore CANALS MENTIONED IN REQUEST MAJOR CITIES PUNJAB Quetta DRAINS MENTIONED IN REQUEST TEHSIL HEADQUARTERS 30° 30° NSDS (shown in SAR but no longer proposed under NDP Project) DISTRICT HEADQUARTERS Area of map PROVINCE HEADQUARTERS BALOCHISTAN RIVERS OR STREAMS PROVINCE BOUNDARIES ISLAMIC REP. OF INDIA IRAN CANALS INTERNATIONAL BOUNDARIES DRAINS SINDH 25 BRANCH/DISTRIBUTARY CANALS 25° Karachi ° AREA WATER BOARDS Arabian Sea BARRAGES 65° 70° 75° 67° 68° 69° 70° 71° This map was produced by the Map Design Unit of The World Bank. The boundaries, colors, denominations and any other information shown Kashmor Guddu Barrage on this map do not imply, on the part of The World Bank Group, any PUNJAB judgment on the legal status of any territory, or any endorsement or Murad acceptance of such boundaries. Unihar Kandh Kot Jacobabad Dil N.W. Canal Hazaro Begari Canal Canal Canal Dy. Feeder Ubauro Begari 28° Khirthar Garhi Khaio Choi Branch Feeder 28° Faizabad Dy. Shikarpur Khanpur Sindh Daharki Ghotki Shahdadkot Garhi Yasin Ghotki Mirpur Mathelo Nujpur Dy. Mithri Dy. Shahdadkot Branch Lakhi Pano Aqil Ratodero Sukkur RBOD (Right Bank Outfall Drain) Miro Khan Branch Sukkur Barrage -

2013-2014 Development Budget
1 SC22051(051) DEVELOPMENT (REVENUE) Rs Charged: ______________ Voted: 33,098,087,000 ______________ Total: 33,098,087,000 ______________ ____________________________________________________________________________________________ AGRICULTURE DEPARTMENT ____________________________________________________________________________________________ AGRICULTURE RESEARCH ____________________________________________________________________________________________ P./ADP DDO Functional-Cum-Object Classification & Budget NO. NO. Particular Of Scheme Estimates 2013 - 2014 ____________________________________________________________________________________________ Rs 04 ECONOMIC AFFAIRS 042 AGRI,FOOD,IRRIGATION,FORESTRY & FISHING 0421 AGRICULTURE 042103 AGRICULTURAL RESEARCH & EXTENSION SERVIC HD9337 DIRECTOR GENERAL AGRICULTURE RESEARCH SINDH. ADP No : 0001 HD09100137 Development and Promotion of Quality Seed through Public 134,896,000 Private Partnership in Sindh A03970 Others 134,896,000 TA9384 DY.DIRECTOR RICE RESEARCH STATION THATTA ADP No : 0002 TA12131410 Rehabilitation of Rice & Cotton Research Station Thatta 34,826,000 A03970 Others 34,826,000 KR9613 SECRETARY AGRICULTURE ADP No : 0003 HD12138010 Establishment of Agriculture Services Complex and Advisory 10,520,000 Centers in Sindh A03970 Others 10,520,000 HD9337 DIRECTOR GENERAL AGRICULTURE RESEARCH SINDH. ADP No : 0004 KA11120007 Development of Bio - Pesticide for mangement of vegetable 9,414,000 pests. A03970 Others 9,414,000 LA9404 DIRECTOR QUAID-E-AWAM ARI LARKANA ADP No : 0005 LA11120008 -

CHINA PAKISTAN ECONOMIC CORRIDOR - PAKISTAN DEVELOPMENT & DISASTER RISK Managementkashi PERSPECTIVE
65°0'0"E 70°0'0"E 75°0'0"E CHINA PAKISTAN ECONOMIC CORRIDOR - PAKISTAN DEVELOPMENT & DISASTER RISK MANAGEMENTKashi PERSPECTIVE NORWAY Baltic Pakistan Major Roads Network July, 2015 ESTONIA Sno Road Name Length (Km) Sno Road Name Length (Km) Sea NORTHERN CORRIDOR SWEDEN 1 Canal Road (Link N-120 Hyderabad) 9 29 N-155 (Larkana - Moenjo Daro) 28 North 2 Chaman Bypass 6 30 N-25 (Karachi - Kalat - Quetta - Chaman) 810 K ii z ii ll s u LATVIA CHINA GLOBAL ECONOMIC CORRIDOR PLAN Sea 3 Dalbandin Basima 154 31 N-255 (Larkana - Nasirabad) 34 K ii r g h ii z DENMARK Moscow 4 E-3 (Kot Sarwar - Hafizabad - Wazirabad) 104 32 N-30 (Basima - Khuzdar) 106 G31 4 LITHUANIA Chelyabinsk ¨§ 5 E-5 (Khanewal - Lodhran) 91 33 N-305 (Sakrand - Shaheed Banazirabad) 22 6 Guddu Barrage Road 41 34 N-35 (Hassanabdal - Thakot - Khunjrab) 807 ISLE EUROPE OF MAN 7 Gwadar Port Road 13 35 N-40 (Lakpass - Dalbandin - Taftan) 610 BELARUS RUSSIA IRELAND UNITED 8 Hyderabad Bypass 13 36 N-45 (Nowshera - Dir - Chitral) 327 KINGDOM Berlin 9 Dual Carriage Road Mirpur Khas 8 37 N-455 (Larkana - Kamber - Shahdadkot) 50 NETHERLANDS GERMANY POLAND CENTRAL ASIA 10 Islamabad Expressway 23 38 N-5 (Karachi - Lahore - Peshawar - Torkham) 1819 Calais Rotterdam C H I N A BELG IUM 11 M-1 (Islamabad - Peshawar) 155 39 N-50 (Kuchlack - Zhob -DI Khan) 508 CZECH 12 M-10 (Karachi Northern Bypass) 60 40 N-55 (Kotri - Larkana - DG Khan - DI Khan - Peshawar) 1220 LUXEMBOURG REPUBLIC 13 M-2 (Islamabad - Lahore) 370 41 N-65 (Sukkur - Sibi - Quetta) 381 JERSEY Paris UKRAINE SLOVAKIA KAZAKHSTAN 14 M-3 -
PESA-DP-Umerkot-Sindh.Pdf
Umarkot Fort District Umarkot, Sindh “Disaster risk reduction has been a part of USAID’s work for decades. ……..we strive to do so in ways that better assess the threat of hazards, reduce losses, and ultimately protect and save more people during the next disaster.” Kasey Channell, Acting Director of the Disaster Response and Mitigation Division of USAID’s Office of U.S. Foreign Disas ter Ass istance (OFDA) PAKISTAN EMERGENCY SITUATIONAL ANALYSIS District Umerkot June 2014 “Disasters can be seen as often as predictable events, requiring forward planning which is integrated in to broader de velopment programs.” Helen Clark, UNDP Administrator, Bureau of Crisis Preven on and Recovery. Annual Report 2011 Disclaimer iMMAP Pakistan is pleased to publish this district profile. The purpose of this profile is to promote public awareness, welfare, and safety while providing community and other related stakeholders, access to vital information for enhancing their disaster mitigation and response efforts. While iMMAP team has tried its best to provide proper source of information and ensure consistency in analyses within the given time limits; iMMAP shall not be held responsible for any inaccuracies that may be encountered. In any situation where the Official Public Records differs from the information provided in this district profile, the Official Public Records should take as precedence. iMMAP disclaims any responsibility and makes no representations or warranties as to the quality, accuracy, content, or completeness of any information contained in this report. Final assessment of accuracy and reliability of information is the responsibility of the user. iMMAP shall not be liable for damages of any nature whatsoever resulting from the use or misuse of information contained in this report.