Zimbabwe Assistance Program in Malaria Quarterly Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Ports of Entry and Routes) (Amendment) Order, 2020
Statutory Instrument 55 ofS.I. 2020. 55 of 2020 Customs and Excise (Ports of Entry and Routes) (Amendment) [CAP. 23:02 Order, 2020 (No. 20) Customs and Excise (Ports of Entry and Routes) (Amendment) “THIRTEENTH SCHEDULE Order, 2020 (No. 20) CUSTOMS DRY PORTS IT is hereby notifi ed that the Minister of Finance and Economic (a) Masvingo; Development has, in terms of sections 14 and 236 of the Customs (b) Bulawayo; and Excise Act [Chapter 23:02], made the following notice:— (c) Makuti; and 1. This notice may be cited as the Customs and Excise (Ports (d) Mutare. of Entry and Routes) (Amendment) Order, 2020 (No. 20). 2. Part I (Ports of Entry) of the Customs and Excise (Ports of Entry and Routes) Order, 2002, published in Statutory Instrument 14 of 2002, hereinafter called the Order, is amended as follows— (a) by the insertion of a new section 9A after section 9 to read as follows: “Customs dry ports 9A. (1) Customs dry ports are appointed at the places indicated in the Thirteenth Schedule for the collection of revenue, the report and clearance of goods imported or exported and matters incidental thereto and the general administration of the provisions of the Act. (2) The customs dry ports set up in terms of subsection (1) are also appointed as places where the Commissioner may establish bonded warehouses for the housing of uncleared goods. The bonded warehouses may be operated by persons authorised by the Commissioner in terms of the Act, and may store and also sell the bonded goods to the general public subject to the purchasers of the said goods paying the duty due and payable on the goods. -

Zimbabwe Rapid Response Drought 2015
Resident / Humanitarian Coordinator Report on the use of CERF funds RESIDENT / HUMANITARIAN COORDINATOR REPORT ON THE USE OF CERF FUNDS ZIMBABWE RAPID RESPONSE DROUGHT 2015 RESIDENT/HUMANITARIAN COORDINATOR Bishow Parajuli REPORTING PROCESS AND CONSULTATION SUMMARY a. Please indicate when the After Action Review (AAR) was conducted and who participated. The CERF After Action Review took place on 25 May 2016. The review brought together focal points from the following key sectors and agencies: Health and Nutrition: UNICEF and WHO, Agriculture: FAO, Food Security: WFP and WASH: UNICEF. Considering the importance of the lessons learnt element, some sectors which did not benefit from the funding did nevertheless participate in order to gain a better understanding of CERF priorities, requirements and implementation strategies. b. Please confirm that the Resident Coordinator and/or Humanitarian Coordinator (RC/HC) Report was discussed in the Humanitarian and/or UN Country Team and by cluster/sector coordinators as outlined in the guidelines. YES X NO Sector focal points were part of the CERF consultation from inception through to final reporting. In addition, a CERF update was a standing agenda item discussed during the monthly Humanitarian Country Team meetings. c. Was the final version of the RC/HC Report shared for review with in-country stakeholders as recommended in the guidelines (i.e. the CERF recipient agencies and their implementing partners, cluster/sector coordinators and members and relevant government counterparts)? YES X NO All -

Mashonaland Central Province Zimbabwe Vulnerability Assessment Committee (Zimvac) 2020 Rural Livelihoods Assessment Report Foreword
Mashonaland Central Province Zimbabwe Vulnerability Assessment Committee (ZimVAC) 2020 Rural Livelihoods Assessment Report Foreword The Zimbabwe Vulnerability Assessment Committee (ZimVAC) under the coordination of the Food and Nutrition Council, successfully undertook the 2020 Rural Livelihoods Assessment (RLA), the 20th since its inception. ZimVAC is a technical advisory committee comprised of representatives from Government, Development Partners, UN, NGOs, Technical Agencies and the Academia. In its endeavour to ‘promote and ensure adequate food and nutrition security for all people at all times’, the Government of Zimbabwe has continued to exhibit its commitment for reducing food and nutrition insecurity, poverty and improving livelihoods amongst the vulnerable populations in Zimbabwe through operationalization of Commitment 6 of the Food and Nutrition Security Policy (FNSP). As the country is grappling with the COVID-19 pandemic, this assessment was undertaken at an opportune time as there was an increasing need to urgently collect up to date food and nutrition security data to effectively support the planning and implementation of actions in a timely and responsive manner. The findings from the RLA will also go a long way in providing local insights into the full impact of the Corona virus on food and nutrition security in this country as the spread of the virus continues to evolve differently by continent and by country. In addition, the data will be of great use to Government, development partners, programme planners and communities in the recovery from the pandemic, providing timely information and helping monitor, prepare for, and respond to COVID-19 and any similar future pandemics. Thematic areas covered in this report include the following: education, food and income sources, income levels, expenditure patterns and food security, COVID-19 and gender based violence, among other issues. -

Assessment of the Zimbabwe Assistance Program in Malaria April 2020
Assessment of the Zimbabwe Assistance Program in Malaria April 2020 Assessment of the Zimbabwe Assistance Program in Malaria April 2020 This publication was produced with the support of the United States Agency for International Development (USAID) under the terms of the Data for Impact Data for Impact (D4I) associate award University of North Carolina at Chapel Hill 7200AA18LA00008, which is implemented by 123 West Franklin Street, Suite 330 the Carolina Population Center at the Chapel Hill, NC 27516 USA University of North Carolina at Chapel Hill, in Phone: 919-445-9350 | Fax: 919-445-9353 [email protected] partnership with Palladium International, LLC; http://www.data4impactproject.org ICF Macro, Inc.; John Snow, Inc.; and Tulane University. The views expressed in this publication do not necessarily reflect the views of USAID or the United States government. TRE-20-29 D4I ISBN 978-1-64232 -258 -3 Assessment of the Zimbabwe Assistance Program in Malaria 2 Acknowledgments This assessment was undertaken by Data for Impact (D4I), funded by the United States Agency for International Development (USAID), in collaboration with the Zimbabwe National Malaria Control Program (NMCP) and the U.S. President’s Malaria Initiative (PMI)/Zimbabwe. The following people were involved in the assessment: Agneta Mbithi, Yazoumé Yé, Andrew Andrada, Cristina de la Torre, Logan Stuck, Joshua Yukich, Erin Luben, and Jessica Fehringer (D4I); and Brian Maguranyanga and Jaqueline Kabongo (M-Consulting Group). The assessment team thanks the people who generously shared their time, experiences, and ideas for the assessment, including the NMCP, led by its director, Dr. Joseph Mberikunashe; the provincial, district, and facility teams; the Zimbabwe Assistance Program in Malaria team; malaria implementing partners (IPs); and the outpatient and antenatal care patients at the health facilities visited. -

PLAAS RR46 Smeadzim 1.Pdf
Chrispen Sukume, Blasio Mavedzenge, Felix Murimbarima and Ian Scoones Faculty of Economic and Management Sciences Research Report 46 Space, Markets and Employment in Agricultural Development: Zimbabwe Country Report Chrispen Sukume, Blasio Mavedzenge, Felix Murimbarima and Ian Scoones Published by the Institute for Poverty, Land and Agrarian Studies, Faculty of Economic and Management Sciences, University of the Western Cape, Private Bag X17, Bellville 7535, Cape Town, South Africa Tel: +27 21 959 3733 Fax: +27 21 959 3732 Email: [email protected] Institute for Poverty, Land and Agrarian Studies Research Report no. 46 June 2015 All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means without prior permission from the publisher or the authors. Copy Editor: Vaun Cornell Series Editor: Rebecca Pointer Photographs: Pamela Ngwenya Typeset in Frutiger Thanks to the UK’s Department for International Development (DfID) and the Economic and Social Research Council’s (ESRC) Growth Research Programme Contents List of tables ................................................................................................................ ii List of figures .............................................................................................................. iii Acronyms and abbreviations ...................................................................................... v 1 Introduction ........................................................................................................ -

Promotion of Climate-Resilient Lifestyles Among Rural Families in Gutu
Promotion of climate-resilient lifestyles among rural families in Gutu (Masvingo Province), Mutasa (Manicaland Province) and Shamva (Mashonaland Central Province) Districts | Zimbabwe Sahara and Sahel Observatory 26 November 2019 Promotion of climate-resilient lifestyles among rural families in Gutu Project/Programme title: (Masvingo Province), Mutasa (Manicaland Province) and Shamva (Mashonaland Central Province) Districts Country(ies): Zimbabwe National Designated Climate Change Management Department, Ministry of Authority(ies) (NDA): Environment, Water and Climate Development Aid from People to People in Zimbabwe (DAPP Executing Entities: Zimbabwe) Accredited Entity(ies) (AE): Sahara and Sahel Observatory Date of first submission/ 7/19/2019 V.1 version number: Date of current submission/ 11/26/2019 V.2 version number A. Project / Programme Information (max. 1 page) ☒ Project ☒ Public sector A.2. Public or A.1. Project or programme A.3 RFP Not applicable private sector ☐ Programme ☐ Private sector Mitigation: Reduced emissions from: ☐ Energy access and power generation: 0% ☐ Low emission transport: 0% ☐ Buildings, cities and industries and appliances: 0% A.4. Indicate the result ☒ Forestry and land use: 25% areas for the project/programme Adaptation: Increased resilience of: ☒ Most vulnerable people and communities: 25% ☒ Health and well-being, and food and water security: 25% ☐ Infrastructure and built environment: 0% ☒ Ecosystem and ecosystem services: 25% A.5.1. Estimated mitigation impact 399,223 tCO2eq (tCO2eq over project lifespan) A.5.2. Estimated adaptation impact 12,000 direct beneficiaries (number of direct beneficiaries) A.5. Impact potential A.5.3. Estimated adaptation impact 40,000 indirect beneficiaries (number of indirect beneficiaries) A.5.4. Estimated adaptation impact 0.28% of the country’s total population (% of total population) A.6. -

Gender in Rural Travel and Transport in Zimbabwe
GENDER IN RURAL TRAVEL AND TRANSPORT IN ZIMBABWE Clinic Grinding mill Firewood Fields Water Market School Work Written for the World Bank (Harare) By Wilfred N Tichagwa Harare December 2000 ii ACKNOWLEDGEMENTS While I take full responsibility for the final views presented herein, I would like to express my gratitude to all those who in one way or another contributed to the production of this report. The report would not have been possible without the support of those who gave of their precious time to grant interviews for information for this report. I greatly appreciate their co-operation. Special thanks go to Dr. George Banjo of the World Bank (Harare) and Ms Petronella Maramba for their comments on the first draft of the report. I also thank the Gender Forum co-ordinated by Unifem (Harare) for their comments on the first draft. Many thanks go also to the numerous participants at the Workshop on Gender in RTT in Zimbabwe, held on the 6-7th November 2000 at the Mandel Training Centre, Marlborough, Harare. I greatly appreciate their inputs in the analysis of gender issues in RTT interventions in Zimbabwe. I am also grateful for the logistical and other support by Mwengo in the production of the report and in preparations for the above-mentioned workshop. I also thank Mwengo and the World Bank for giving me the opportunity to do this study. I sincerely hope that the report will contribute towards strengthening the gender component of the RTT interventions in Zimbabwe. Wilfred N. Tichagwa iii TABLE OF CONTENTS Acknowledgement II Table of -
Fire Report 2014
ANNUAL FIRE REPORT 2014 FIRE Hay bailing along the Victoria Falls- Kazungula Road to reduce road side fires Page 1 of 24 ANNUAL FIRE REPORT 2014 Table of Contents 1.0 Introduction ......................................................................................................................................... 3 2.0 Fire Prediction Modelling ..................................................................................................................... 3 3.0 Fire Monitoring .................................................................................................................................... 7 4.0 Environmental Education and Training ................................................................................................ 8 5.0 EMA/ZRP Fire Management Awards ................................................................................................. 14 6.0 Law enforcement ............................................................................................................................... 17 7.0 Impacts of Fires .................................................................................................................................. 18 7.0 Conclusion .......................................................................................................................................... 21 8.0 Recommendations ............................................................................................................................. 22 Annex 1: Pictures .................................................................................................................................... -
LAN Installation Sites Coordinates
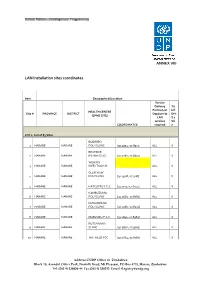
ANNEX VIII LAN Installation sites coordinates Item Geographical/Location Service Delivery Tic Points (List k if HEALTH CENTRE Site # PROVINCE DISTRICT Dept/umits DHI (EPMS SITE) LAN S 2 services Sit COORDINATES required e LOT 1: List of 83 Sites BUDIRIRO 1 HARARE HARARE POLYCLINIC [30.9354,-17.8912] ALL X BEATRICE 2 HARARE HARARE RD.INFECTIO [31.0282,-17.8601] ALL X WILKINS 3 HARARE HARARE INFECTIOUS H ALL X GLEN VIEW 4 HARARE HARARE POLYCLINIC [30.9508,-17.908] ALL X 5 HARARE HARARE HATCLIFFE P.C.C. [31.1075,-17.6974] ALL X KAMBUZUMA 6 HARARE HARARE POLYCLINIC [30.9683,-17.8581] ALL X KUWADZANA 7 HARARE HARARE POLYCLINIC [30.9285,-17.8323] ALL X 8 HARARE HARARE MABVUKU P.C.C. [31.1841,-17.8389] ALL X RUTSANANA 9 HARARE HARARE CLINIC [30.9861,-17.9065] ALL X 10 HARARE HARARE HATFIELD PCC [31.0864,-17.8787] ALL X Address UNDP Office in Zimbabwe Block 10, Arundel Office Park, Norfolk Road, Mt Pleasant, PO Box 4775, Harare, Zimbabwe Tel: (263 4) 338836-44 Fax:(263 4) 338292 Email: [email protected] NEWLANDS 11 HARARE HARARE CLINIC ALL X SEKE SOUTH 12 HARARE CHITUNGWIZA CLINIC [31.0763,-18.0314] ALL X SEKE NORTH 13 HARARE CHITUNGWIZA CLINIC [31.0943,-18.0152] ALL X 14 HARARE CHITUNGWIZA ST.MARYS CLINIC [31.0427,-17.9947] ALL X 15 HARARE CHITUNGWIZA ZENGEZA CLINIC [31.0582,-18.0066] ALL X CHITUNGWIZA CENTRAL 16 HARARE CHITUNGWIZA HOSPITAL [31.0628,-18.0176] ALL X HARARE CENTRAL 17 HARARE HARARE HOSPITAL [31.0128,-17.8609] ALL X PARIRENYATWA CENTRAL 18 HARARE HARARE HOSPITAL [30.0433,-17.8122] ALL X MURAMBINDA [31.65555953980,- 19 MANICALAND -

Status of Telecommunications Sector in Zimbabwe
TELECOMMUNICATIONS STATUS IN ZIMBABWE Sirewu Baxton [email protected] Background • Postal and Telecommunications Regulatory Authority of Zimbabwe (POTRAZ) o Established by the Postal and Telecommunications Act of 2000. o Started its operations in March 2001 o POTRAZ situated at Emerald Business Park, No. 30 The Chase Harare • Legislation brought about a new institutional framework for telecommunications: o Liberalized the sector o Introduced distinct roles of government, regulator, operators, and consumers. POTRAZ MANDATE • Ensuring provision of sufficient domestic and international telecommunication services • Ensuring provision of services at rates consistent with the provision of an efficient and continuous service • Promote the development of the sector services in accordance with: o Practicable recognised international standards o Public demand POTRAZ MANDATE cont’d • Furthers the advancement of technology • Represents Zimbabwe internationally in matters relating to the sector • Establishes, approves or controls the National Numbering plan • Manages the Radio Frequency Resource • Advises the Government on all matters relating to the telecommunication services General Country Background Location Southern Africa Area 390 590 square Km Population 12.6 Million Population Distribution 38% Urban: 62% Rural • Telecommunication service usage is mainly in urban areas. MARKET STRUCTURE FIXED • One fixed public operator (TelOne.) • Offers local, regional and international voice telephone services. • Has 337 881 subscribers (Lines) • The fixed teledensity is 2.68%. • Of these, 61 % are in the capital Harare. • 53% are residential lines. • 84 % of the lines are connected to the digital exchange. • 17 % of the lines are in rural areas. MARKET STRUCTURE MOBILE • There are three mobile operators: Econet, Net One and Telecel • The current subscriber base as at 30 June 2011 for the operators: Econet 5,521,000 Telecel 1,297,000 Net One 1,349,000 • Mobile teledensity stands at 64.85 %. -

Government Gazette
ZIMBABWEAN, GOVERNMENT GAZETTE Published by Authority f Vol. LX, No. 33 I4th MAY, 1982 Price 30c General Notice 443 of1982. “ts RESERVE BANK OF ZIMBABWE ACT [CHAPTER 173}. Statement of Assets and Liabilities of the Reserve Bank of Zimbabwe :5 . ey = IN termsofsection 20 of the Réserve Bank of Zimbabwe Act [Chapter 173], a statementofthe assets andliabilities of the Reserve Bank of Zimbabweas at the 30th April, 1982, is published in the Schedule. ' 14-5-82. B. WALTERS, : me ‘ - Secretaryto the ‘Treasury. oo SCHEDULE *s , | oS STATEMENT OF ASSETS AND LIABILITIES AS AT THE 307ra APRIL, 1982 Liabilities . Assets> : Capital ee ee _ 2000 000 Gold and foreign assets : General 156 429 939 Reserve Fund... jr5-200 000 ° Loans and advances , 42 105 000 Currency in circulation. 2 . 2... 39 389 892 Tnternal investments— . core o e 4 6 ) 276.227 845 Deposits and other liabilities to the public . 9 012 Governmentstock . Other . 110342 535 liabilities ee eee 112 230 527 | Other. 165 885 310 \ Other assets °° 164 606 647 $639 369 431 $639 369 431 . , General Notice 444of 1982. LIQUOR ACT [CHAPTER 289] Liquor Licensing Board: Annual Meeting: Mtoko District PURSUANT to the'provisions of subsection (1) of section 47 of the Liquor Act [Chapter 289), notice is hereby given that the annual meeting of the Liquor Licensing Board for the district of Mtoko will be held at the Administrative Court, Chaplin Buildings, Samora Machel Avenue Central, Harare, commencing at 9 a.m. on Monday the 7th day of June, 1982, to consider the following matters: . y ; APPLICATIONS FOR NEW LIQUOR LICENCES, ; ® ~ BOTTLE LIQUOR LICENCES Trading name Situation ofpremises Applicant Proposedmanager Gurupjra General Dealer and Bottle Lease site T.T. -

Grant Assistance for Grassroots Human Projects in Zimbabwe
Grant Assistance for Grassroots Human Projects in Zimbabwe Amount Amount No Year Project Title Implementing Organisation District (US) (yen) 1 1989 Mbungu Primary School Development Project Mbungu Primary School Gokwe 16,807 2,067,261 2 1989 Sewing and Knitting Project Rutowa Young Women's Club Gutu 5,434 668,382 3 1990 Children's Agricultural Project Save the Children USA Nyangombe 8,659 1,177,624 Mbungo Uniform Clothing Tailoring Workshop 4 1990 Mbungo Women's Club Masvingo 14,767 2,008,312 Project Construction of Gardening Facilities in 5 1991 Cold Comfort Farm Trust Harare 42,103 5,431,287 Support of Small-Scale Farmers 6 1991 Pre-School Project Kwayedza Cooperative Gweru 33,226 4,286,154 Committee for the Rural Technical 7 1992 Rural Technical Training Project Murehwa 38,266 4,936,314 Training Project 8 1992 Mukotosi Schools Project Mukotosi Project Committee Chivi 20,912 2,697,648 9 1992 Bvute Dam Project Bvute Dam Project Committee Chivi 3,558 458,982 10 1992 Uranda Clinic Project Uranda Clinic Project Committee Chivi 1,309 168,861 11 1992 Utete Dam Project Utete Dam Project Committee Chivi 8,051 1,038,579 Drilling of Ten Boreholes for Water and 12 1993 Irrigation in the Inyathi and Tsholotsho Help Age Zimbabwe Tsholotsho 41,574 5,072,028 PromotionDistricts of ofSocialForestry Matabeleland andManagement Zimbabwe National Conservation 13 1993 Buhera 46,682 5,695,204 ofWoodlands inCommunalAreas ofZimbabwe Trust Expansion of St. Mary's Gavhunga Primary St. Mary's Gavhunga Primary 14 1994 Kadoma 29,916 3,171,096 School School Tsitshatshawa