Augmented Reality System for Medical Training and Simulation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
A Review About Augmented Reality Tools and Developing a Virtual Reality Application
Academic Journal of Science, CD-ROM. ISSN: 2165-6282 :: 03(02):139–146 (2014) $5(9,(:$%287$8*0(17('5($/,7<722/6$1' '(9(/23,1*$9,578$/5($/,7<$33/,&$7,21%$6('21 ('8&$7,21 0XVWDID8ODVDQG6DID0HUYH7DVFL )LUDW8QLYHULVLW\7XUNH\ Augmented Reality (AR) is a technology that gained popularity in recent years. It is defined as placement of virtual images over real view in real time. There are a lot of desktop applications which are using Augmented Reality. The rapid development of technology and easily portable mobile devices cause the increasing of the development of the applications on the mobile device. The elevation of the device technology leads to the applications and cause the generating of the new tools. There are a lot of AR Tool Kits. They differ in many ways such as used methods, Programming language, Used Operating Systems, etc. Firstly, a developer must find the most effective tool kits between them. This study is more of a guide to developers to find the best AR tool kit choice. The tool kit was examined under three main headings. The Parameters such as advantages, disadvantages, platform, and programming language were compared. In addition to the information is given about usage of them and a Virtual Reality application has developed which is based on Education. .H\ZRUGV Augmented reality, ARToolKit, Computer vision, Image processing. ,QWURGXFWLRQ Augmented reality is basically a snapshot of the real environment with virtual environment applications that are brought together. Basically it can be operated on every device which has a camera display and operation system. -

Augmented Reality & Virtual Reality Is Now a Reality for Enterprises
WHITE PAPER AUGMENTED REALITY & VIRTUAL REALITY IS NOW A REALITY FOR ENTERPRISES- THE FUTURE IS HERE! Abstract Innovation and next-generation technologies have completely changed the way we work, live and possibly even the way we think. AI, Augmented Reality (AR), Virtual Reality (VR), and Blockchain are just some of the technologies that have affected how we consume art, music, movies, and how we communicate, shop, and travel. We are in the midst of a complete digital revolution. This perspective paper illustrates a point of view on the use of mixed reality (MR) in today’s enterprise environment, and covers-- virtual reality and augmented reality, market trends, industry examples, and challenges within organizations that are adopting mixed reality. In short, it sheds light on what the future is expected to look like in the context of enterprise disruption with MR. Introduction Johnny Mnemonic, the Lawnmower Man, Minority Report, the Matrix, Minority Report, the Terminator 2, Ironman… Besides captivating audiences with their Everyone seems to know what VR headsets using special electronic equipment, such as stunning visual effects, these films all have are, and the popularity of Pokémon a helmet with an internal screen or gloves one thing in common - they showcase how Go almost allows omission of a basic fitted with sensors.” VR can digitally recreate MR technologies could be potentially used introduction to AR. Though they are often the environment around you, or give you in the future. used interchangeably, it is essential to clarify the impression you are somewhere entirely that AR and VR are not the same. -
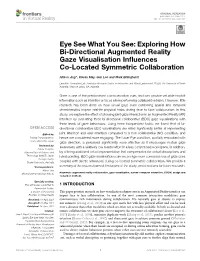
Exploring How Bi-Directional Augmented Reality Gaze Visualisation Influences Co-Located Symmetric Collaboration
ORIGINAL RESEARCH published: 14 June 2021 doi: 10.3389/frvir.2021.697367 Eye See What You See: Exploring How Bi-Directional Augmented Reality Gaze Visualisation Influences Co-Located Symmetric Collaboration Allison Jing*, Kieran May, Gun Lee and Mark Billinghurst Empathic Computing Lab, Australian Research Centre for Interactive and Virtual Environment, STEM, The University of South Australia, Mawson Lakes, SA, Australia Gaze is one of the predominant communication cues and can provide valuable implicit information such as intention or focus when performing collaborative tasks. However, little research has been done on how virtual gaze cues combining spatial and temporal characteristics impact real-life physical tasks during face to face collaboration. In this study, we explore the effect of showing joint gaze interaction in an Augmented Reality (AR) interface by evaluating three bi-directional collaborative (BDC) gaze visualisations with three levels of gaze behaviours. Using three independent tasks, we found that all bi- directional collaborative BDC visualisations are rated significantly better at representing Edited by: joint attention and user intention compared to a non-collaborative (NC) condition, and Parinya Punpongsanon, hence are considered more engaging. The Laser Eye condition, spatially embodied with Osaka University, Japan gaze direction, is perceived significantly more effective as it encourages mutual gaze Reviewed by: awareness with a relatively low mental effort in a less constrained workspace. In addition, Naoya Isoyama, Nara Institute of Science and by offering additional virtual representation that compensates for verbal descriptions and Technology (NAIST), Japan hand pointing, BDC gaze visualisations can encourage more conscious use of gaze cues Thuong Hoang, Deakin University, Australia coupled with deictic references during co-located symmetric collaboration. -

Evaluating Performance Benefits of Head Tracking in Modern Video
Evaluating Performance Benefits of Head Tracking in Modern Video Games Arun Kulshreshth Joseph J. LaViola Jr. Department of EECS Department of EECS University of Central Florida University of Central Florida 4000 Central Florida Blvd 4000 Central Florida Blvd Orlando, FL 32816, USA Orlando, FL 32816, USA [email protected] [email protected] ABSTRACT PlayStation Move, TrackIR 5) that support 3D spatial in- teraction have been implemented and made available to con- We present a study that investigates user performance ben- sumers. Head tracking is one example of an interaction tech- efits of using head tracking in modern video games. We nique, commonly used in the virtual and augmented reality explored four di↵erent carefully chosen commercial games communities [2, 7, 9], that has potential to be a useful ap- with tasks which can potentially benefit from head tracking. proach for controlling certain gaming tasks. Recent work on For each game, quantitative and qualitative measures were head tracking and video games has shown some potential taken to determine if users performed better and learned for this type of gaming interface. For example, Sko et al. faster in the experimental group (with head tracking) than [10] proposed a taxonomy of head gestures for first person in the control group (without head tracking). A game ex- shooter (FPS) games and showed that some of their tech- pertise pre-questionnaire was used to classify participants niques (peering, zooming, iron-sighting and spinning) are into casual and expert categories to analyze a possible im- useful in games. In addition, previous studies [13, 14] have pact on performance di↵erences. -
Virtual and Augmented Reality
Virtual and Augmented Reality Virtual and Augmented Reality: An Educational Handbook By Zeynep Tacgin Virtual and Augmented Reality: An Educational Handbook By Zeynep Tacgin This book first published 2020 Cambridge Scholars Publishing Lady Stephenson Library, Newcastle upon Tyne, NE6 2PA, UK British Library Cataloguing in Publication Data A catalogue record for this book is available from the British Library Copyright © 2020 by Zeynep Tacgin All rights for this book reserved. No part of this book may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission of the copyright owner. ISBN (10): 1-5275-4813-9 ISBN (13): 978-1-5275-4813-8 TABLE OF CONTENTS List of Illustrations ................................................................................... x List of Tables ......................................................................................... xiv Preface ..................................................................................................... xv What is this book about? .................................................... xv What is this book not about? ............................................ xvi Who is this book for? ........................................................ xvii How is this book used? .................................................. xviii The specific contribution of this book ............................. xix Acknowledgements ........................................................... -

Augmented Reality, Virtual Reality, & Health
University of Massachusetts Medical School eScholarship@UMMS National Network of Libraries of Medicine New National Network of Libraries of Medicine New England Region (NNLM NER) Repository England Region 2017-3 Augmented Reality, Virtual Reality, & Health Allison K. Herrera University of Massachusetts Medical School Et al. Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/ner Part of the Health Information Technology Commons, Library and Information Science Commons, and the Public Health Commons Repository Citation Herrera AK, Mathews FZ, Gugliucci MR, Bustillos C. (2017). Augmented Reality, Virtual Reality, & Health. National Network of Libraries of Medicine New England Region (NNLM NER) Repository. https://doi.org/ 10.13028/1pwx-hc92. Retrieved from https://escholarship.umassmed.edu/ner/42 Creative Commons License This work is licensed under a Creative Commons Attribution-Noncommercial-Share Alike 4.0 License. This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in National Network of Libraries of Medicine New England Region (NNLM NER) Repository by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. Augmented Reality, Virtual Reality, & Health Zeb Mathews University of Tennessee Corina Bustillos Texas Tech University Allison Herrera University of Massachusetts Medical School Marilyn Gugliucci University of New England Outline Learning Objectives Introduction & Overview Objectives: • Explore AR & VR technologies and Augmented Reality & Health their impact on health sciences, Virtual Reality & Health with examples of projects & research Technology Funding Opportunities • Know how to apply for funding for your own AR/VR health project University of New England • Learn about one VR project funded VR Project by the NNLM Augmented Reality and Virtual Reality (AR/VR) & Health What is AR and VR? F. -

Natural Interaction in Augmented Reality Context
Natural Interaction in Augmented Reality Context John Aliprantis1, Markos Konstantakis1, Rozalia Nikopoulou2, Phivos Mylonas2 and George Caridakis1 1 University of the Aegean, 81100 Mytilene, Greece {jalip, mkonstadakis, gcari}@aegean.gr 2 Ionian University 49100 Corfu, Greece [email protected], [email protected] Abstract. In recent years, immersive technologies like Virtual and Augmented Reality have been accelerating at an incredible pace, building innovative experiences and developing new interaction paradigms. Current research has widely explored gesture interaction with Augmented Reality interfaces, but usually requires users to manipulate input devices that could be cumbersome and obtrusive, thus preventing them from interacting efficiently with the 3D environment. Therefore, Natural User Interfaces and freehand gesture interaction are becoming more and more popular, improving the user’s engagement and sense of presence, providing more stimulating, user-friendly and non-obtrusive interaction methods. However, researchers argue about the impact of the interaction fidelity in usability and user satisfaction, questioning the level of naturalness that should characterize the interaction metaphors. Current paper proposes different gesture recognition techniques for three basic interaction categories (translation, rotation and scaling) in a Leap Motion Controller - Augmented Reality framework. A prototype is implemented in order to evaluate efficiency and usability of the proposed architecture. Finally, experimental results are discussed. Keywords: Natural interactionAugmented realityLeap motion controller Gesture recognition. 1 Introduction Over the last few years, Augmented Reality (AR) has developed into a cutting edge technology, providing new ways to interact with computer – generated information. By removing the boundaries between physical and virtual, AR has been able to create more engaging experiences, enhancing user’s enjoyment and satisfaction. -

The Growing Demand for AR/VR in the Workplace
The Growing Demand for AR/VR in the Workplace AR and VR applications in the workplace are benefiting businesses By Daniel Newman, Principal Analyst of Futurum Research Sponsored by Dell It started with Pokémon GO—a simple, yet ingenious app that enabled anyone to catch and train Pokémon in the "real" world—or at least the augmented reality (AR) world. Pokémon fans and nonfans alike scrambled to catch Pokémon, visiting local retailers and landmarks as they hunted. While Pokémon GO was by no means the world's first glance at AR, it brought AR to real, practical use. The app marked the rise of the AR app in the mainstream, and left users hungry for more. Now, increased demand for AR and virtual reality (VR) applications in the workplace is giving life to new ways to leverage this immersive technology to benefit businesses. Track the Move from Mobile to Goggle Just as we techies tracked the shift from desktop to mobile—mobile finally tipped the scale in 2014—we are also tracking the rate of "goggle" adoption. We've already witnessed an impressive move from desktop screen to goggles, headsets, and accessories in 2016—and new tools are burgeoning on the horizon. Virtualization engineers and designers are making the hardware more wearable in 2017 and beyond. Major brands such as Google, Microsoft, Facebook, Samsung, and GoPro are pouring funds into VR and AR applications (Apple, IBM, and Amazon projects are also in development), proving that virtualization isn't a passing trend or tech fad—it's here to stay. That's not to say goggles will replace mobile, or even replace the desktop. -

Augmented Reality for Unity: the Artoolkit Package JM Vezien Jan
Augmented reality for Unity: the ARToolkit package JM Vezien Jan 2016 ARToolkit provides an easy way to develop AR applications in Unity via the ARTookit package for Unity, available for download at: http://artoolkit.org/documentation/doku.php?id=6_Unity:unity_about The installation is covered in: http://artoolkit.org/documentation/doku.php?id=6_Unity:unity_getting_started Basically, you import the package via Assets--> Import Package--> custom Package Current version is 5.3.1 Once imported, the package provides assets in the ARToolkit5-Unity hierarchy. There is also an additional ARToolkit entry in the general menu of unity. A bunch of example scenes are available for trials in ARToolkit5-Unity-->Example scenes. The simplest is SimpleScene.unity, where a red cube is attached to a "Hiro" pattern, like the simpleTest example in the original ARToolkit tutorials. The way ARToolkit for Unity organises information is simple: • The mandatory component for ARToolkit is called a ARController. Aside from managing the camera parameters (for example, selecting the video input), it also records the complete list of markers your application will use, via ARMarker scripts (one per marker). • A "Scene Root" will contain everything you need to AR display. It is a standard (usually empty) object with a AR Origin script. the rest of the scene will be children of it. • The standard camera remains basically the same, but is now driven by a specific ARCamera script. By default, the camera is a video see-through (like a webcam). • Objects to be tracked are usually "empty" geomeries (GameObject--> Create empty) to which one attaches a special AR Tracked Object script. -
Advanced Assistive Maintenance Based on Augmented Reality and 5G Networking
sensors Article Advanced Assistive Maintenance Based on Augmented Reality and 5G Networking Sebastiano Verde 1 , Marco Marcon 2,* , Simone Milani 1 and Stefano Tubaro 2 1 Department of Information Engineering, University of Padova, 35131 Padua, Italy; [email protected] (S.V.); [email protected] (S.M.) 2 Dipartimento di Elettronica, Informazione e Bioingegneria, Politecnico di Milano, 20133 Milan, Italy; [email protected] * Correspondence: [email protected] Received: 13 November 2020; Accepted: 9 December 2020; Published: 14 December 2020 Abstract: Internet of Things (IoT) applications play a relevant role in today’s industry in sharing diagnostic data with off-site service teams, as well as in enabling reliable predictive maintenance systems. Several interventions scenarios, however, require the physical presence of a human operator: Augmented Reality (AR), together with a broad-band connection, represents a major opportunity to integrate diagnostic data with real-time in-situ acquisitions. Diagnostic information can be shared with remote specialists that are able to monitor and guide maintenance operations from a control room as if they were in place. Furthermore, integrating heterogeneous sensors with AR visualization displays could largely improve operators’ safety in complex and dangerous industrial plants. In this paper, we present a complete setup for a remote assistive maintenance intervention based on 5G networking and tested at a Vodafone Base Transceiver Station (BTS) within the Vodafone 5G Program. Technicians’ safety was improved by means of a lightweight AR Head-Mounted Display (HDM) equipped with a thermal camera and a depth sensor to foresee possible collisions with hot surfaces and dangerous objects, by leveraging the processing power of remote computing paired with the low latency of 5G connection. -

Towards Augmented Reality User Interfaces in 3D Media Production
Towards Augmented Reality User Interfaces in 3D Media Production Max Krichenbauer∗ Goshiro Yamamoto† Takafumi Taketomi‡ Christian Sandor§ Hirokazu Kato¶ Interactive Media Design Laboratory Nara Institute of Science and Technology Figure 1: Our goal is to establish Augmented Reality as a user interface for professional media production. Our approach consists of three steps: We conducted an online survey with 3D media professionals from all around the world (a). Based on their responses, we derived requirements and designed a user interface (b). We then implemented a prototype (c) and evaluated it with media professionals in a pilot study. ABSTRACT 1 INTRODUCTION The idea of using Augmented Reality (AR) user interfaces (UIs) to Even before the advent of AR, the idea of creating an immersive create 3D media content, such as 3D models for movies and games 3D modeling application for creating 3D content was proposed by has been repeatedly suggested over the last decade. Even though Clark [7]. However, even though AR has been shown to be excel- the concept is intuitively compelling and recent technological ad- lent for 3D tasks thanks to correct spatial alignment [24, 26], there vances have made such an application increasingly feasible, very is, to our knowledge, no fully functioning immersive 3D UI avail- little progress has been made towards an actual real-world appli- able for professional 3D content creation, including film, TV, or cation of AR in professional media production. To this day, no games. A number of AR CAD applications were created and tested immersive 3D UI has been commonly used by professionals for 3D by researchers, but none of them was based on a requirements anal- computer graphics (CG) content creation. -

Using Smart Glasses and Augmented Reality Head-Mounted Displays To
Using smart glasses and augmented reality head-mounted displays to drive supply chain innovation A series exploring Industry 4.0 technologies and their potential impact for enabling digital supply networks in manufacturing Using smart glasses and augmented reality head-mounted displays to drive supply chain innovation Contents What are smart glasses and augmented reality HMDs? 4 Benefits of smart glasses and AR in the supply chain 6 Criteria for evaluation and adoption 8 Key applications for smart glasses in your supply chain 10 Getting started with smart glasses and augmented reality devices 11 Key Deloitte contacts in smart glasses and augmented reality 12 02 Using smart glasses and augmented reality head-mounted displays to drive supply chain innovation Do you need smart glasses in your supply chain? Smart glasses are already being used to improve quality, standardize workflows, accelerate decision making, and enhance communication in logistics, manufacturing, and maintenance operations throughout the supply chain. Of interest because: A trend in more universal, data-driven decision making is evolving just as leaps in hardware and software capability have led to smaller, more ergonomic devices. Could improve your supply chain by: Boosting labor effectiveness and productivity; reducing quality defects and rework; improving workflow standardization; enhancing workforce collaboration; improving safety. Why not? The technology is still rapidly evolving and has not yet reached operational maturity. Companies will have to understand how they will leverage data for critical use cases and should expect difficult integration challenges. Deloitte recommends: Evaluate the business case for smart glasses and augmented reality in your supply chain and pilot on a small number of critical use cases.