International Narcotic Control Board (INCB) Annual Report 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Noscapine Suppresses Angiotensin Converting Enzyme Inhibitors-Induced Cough
Blackwell Science, LtdOxford, UKNEPNephrology1320-53582005 Asian Pacific Society of NephrologyAugust 2005104348350Original ArticleNoscapine suppresses ACEI-induced coughA Mooraki et al. NEPHROLOGY 2005; 10, 348–350 doi:10.1111/j.1440-1797.2005.00429.x Original Article Noscapine suppresses angiotensin converting enzyme inhibitors-induced cough AHMAD MOORAKI,1 ARIA JENABI,1 MOSADEGH JABBARI,1 MOHAMMAD I ZOLFAGHARI,2 SAHAR Z JAVANMARDI,2 MASOUD MAHMOUDIAN3 and BAHAR BASTANI4 1Division of Nephrology, Rasool Akram Medical Center and 3Razi Institute for Drug Research, Iran University of Medical Sciences and 2Department of Pharmacology, School of Pharmacy, Azad University, Iran and 4Division of Nephrology, Saint Louis University School of Medicine, Saint Louis, Missouri, USA SUMMARY: Background: Dry cough is a common side-effect of the angiotensin converting enzyme inhibitors (ACEI) and is a major limiting factor of their use. It has been suggested that ACEI cause this side-effect by potentiation of the bradykinin effect. Previous work in our laboratory has shown that noscapine, an antitussive drug, inhibits the effect of bradykinin. Methods: To investigate the effect of noscapine on ACEI-induced cough, 611 hypertensive patients who were being treated with ACEI were evaluated for the incidence of persistent dry cough. Results: A cough had developed in 65 (10.6%) patients, two (3.1%) of whom also had severe respiratory dis- tress that required hospitalisation and immediate discontinuation of the ACEI. Forty-two (64.6%) patients had developed a mild cough and 21 (32.3%) patients had developed a moderate to severe cough. The patients with moderate to severe cough received 15 mg of noscapine, orally three times daily, while they continued ACEI. -

Report of the International Narcotics Control Board for 2012
CHAPTER III. ANALYSIS OF THE WORLD SITUATION reported slight increases, however, while other acceding to the other two international drug control countries reported increases in injecting risk behaviour treaties. or low coverage of prevention services among injecting 803. However, the fact remains that nine States in drug users. Oceania have yet to become parties to all three of the international drug control treaties, and this continues to E. Oceania be a matter of grave concern for the Board, particularly in the light of increased reports of trafficking in and illicit 1. Major developments manufacture of drugs in the region. High prevalence rates for the abuse of cannabis and knowledge of illicit 800. The rates of abuse and illicit manufacture of methamphetamine manufacture in Oceania make it an amphetamine-type stimulants in Oceania are still among area particularly susceptible to organized crime. The the highest in the world. This trend is particularly well Board continues to urge all States concerned, namely the documented in Australia and New Zealand, although methamphetamine abuse is reported to be stable or Cook Islands, Kiribati, Nauru, Palau, Papua New Guinea, declining in those countries. While domestic illicit Samoa, Solomon Islands, Tuvalu and Vanuatu, to accede manufacture in Australia and New Zealand is widespread, without further delay to any of the three international the recent crackdown on precursor chemicals used in drug control treaties to which they are not yet parties. domestic manufacture has caused the price of Those States may easily become used by traffickers who amphetamine-type stimulants to rise, which has in turn want to supply the Australian and New Zealand markets. -

Federal Controlled Substances Checklist
Federal Controlled Substances Checklist Introduction By Norton Tooby & Joseph Justin Rollin We have reprinted here an alphabetical list of all controlled substances forbidden under federal drug laws, taken from the official website of the U.S. Department of Justice, Drug Enforcement Administration, Office of Diversion Control, at http://www.justice.gov/dea/pubs/scheduling.html. No copyright is asserted to this information. This list changes frequently. The official list is contained at 21 CFR § 1308, as supplemented by final rules published in the Federal Register. The attached checklist of controlled substances has been compiled into one list, and placed in alphabetical order, for ease of reference. If a controlled substance is listed in the federal drug schedules, it triggers deportation, INA § 237(a)(2)(B)(i), 8 U.S.C. § 1227(a)(2)(B)(i), and inadmissibility. INA § 212(a)(2)(A)(i)(II), 8 U.S.C. § 1182(a)(2)(A)(i)II). In addition, there is an aggravated felony defined as illicit trafficking in a controlled substance. INA § 101(a)(43)(B), 8 U.S.C. § 1101(a)(43)(B). The same controlled substance lists apply to this ground of deportation as well. If a drug is not listed on the federal controlled substances schedules, it does not trigger removal under these grounds. In addition, because the government has the burden of proof in deportation removal proceedings by clear and convincing evidence, if the record of conviction is ambiguous as to whether the specific substance involved in the particular case was listed on the federal schedules, the government cannot obtain a deportation removal order on this ground. -

Recommended Methods for the Identification and Analysis of Fentanyl and Its Analogues in Biological Specimens
Recommended methods for the Identification and Analysis of Fentanyl and its Analogues in Biological Specimens MANUAL FOR USE BY NATIONAL DRUG ANALYSIS LABORATORIES Laboratory and Scientific Section UNITED NATIONS OFFICE ON DRUGS AND CRIME Vienna Recommended Methods for the Identification and Analysis of Fentanyl and its Analogues in Biological Specimens MANUAL FOR USE BY NATIONAL DRUG ANALYSIS LABORATORIES UNITED NATIONS Vienna, 2017 Note Operating and experimental conditions are reproduced from the original reference materials, including unpublished methods, validated and used in selected national laboratories as per the list of references. A number of alternative conditions and substitution of named commercial products may provide comparable results in many cases. However, any modification has to be validated before it is integrated into laboratory routines. ST/NAR/53 Original language: English © United Nations, November 2017. All rights reserved. The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations concerning the legal status of any country, territory, city or area, or of its authorities, or concerning the delimitation of its frontiers or boundaries. Mention of names of firms and commercial products does not imply the endorse- ment of the United Nations. This publication has not been formally edited. Publishing production: English, Publishing and Library Section, United Nations Office at Vienna. Acknowledgements The Laboratory and Scientific Section of the UNODC (LSS, headed by Dr. Justice Tettey) wishes to express its appreciation and thanks to Dr. Barry Logan, Center for Forensic Science Research and Education, at the Fredric Rieders Family Founda- tion and NMS Labs, United States; Amanda L.A. -

DEMAND REDUCTION a Glossary of Terms
UNITED NATIONS PUBLICATION Sales No. E.00.XI.9 ISBN: 92-1-148129-5 ACKNOWLEDGEMENTS This document was prepared by the: United Nations International Drug Control Programme (UNDCP), Vienna, Austria, in consultation with the Commonwealth of Health and Aged Care, Australia, and the informal international reference group. ii Contents Page Foreword . xi Demand reduction: A glossary of terms . 1 Abstinence . 1 Abuse . 1 Abuse liability . 2 Action research . 2 Addiction, addict . 2 Administration (method of) . 3 Adverse drug reaction . 4 Advice services . 4 Advocacy . 4 Agonist . 4 AIDS . 5 Al-Anon . 5 Alcohol . 5 Alcoholics Anonymous (AA) . 6 Alternatives to drug use . 6 Amfetamine . 6 Amotivational syndrome . 6 Amphetamine . 6 Amyl nitrate . 8 Analgesic . 8 iii Page Antagonist . 8 Anti-anxiety drug . 8 Antidepressant . 8 Backloading . 9 Bad trip . 9 Barbiturate . 9 Benzodiazepine . 10 Blood-borne virus . 10 Brief intervention . 11 Buprenorphine . 11 Caffeine . 12 Cannabis . 12 Chasing . 13 Cocaine . 13 Coca leaves . 14 Coca paste . 14 Cold turkey . 14 Community empowerment . 15 Co-morbidity . 15 Comprehensive Multidisciplinary Outline of Future Activities in Drug Abuse Control (CMO) . 15 Controlled substance . 15 Counselling and psychotherapy . 16 Court diversion . 16 Crash . 16 Cross-dependence . 17 Cross-tolerance . 17 Custody diversion . 17 Dance drug . 18 Decriminalization or depenalization . 18 Demand . 18 iv Page Demand reduction . 19 Dependence, dependence syndrome . 19 Dependence liability . 20 Depressant . 20 Designer drug . 20 Detoxification . 20 Diacetylmorphine/Diamorphine . 21 Diuretic . 21 Drug . 21 Drug abuse . 22 Drug abuse-related harm . 22 Drug abuse-related problem . 22 Drug policy . 23 Drug seeking . 23 Drug substitution . 23 Drug testing . 24 Drug use . -

Control Substance List
Drugs DrugID SubstanceName DEANumbScheNarco OtherNames 1 1-(1-Phenylcyclohexyl)pyrrolidine 7458 I N PCPy, PHP, rolicyclidine 2 1-(2-Phenylethyl)-4-phenyl-4-acetoxypiperidine 9663 I Y PEPAP, synthetic heroin 3 1-[1-(2-Thienyl)cyclohexyl]piperidine 7470 I N TCP, tenocyclidine 4 1-[1-(2-Thienyl)cyclohexyl]pyrrolidine 7473 I N TCPy 5 13Beta-ethyl-17beta-hydroxygon-4-en-3-one 4000 III N 6 17Alpha-methyl-3alpha,17beta-dihydroxy-5alpha-androstane 4000 III N 7 17Alpha-methyl-3beta,17beta-dihydroxy-5alpha-androstane 4000 III N 8 17Alpha-methyl-3beta,17beta-dihydroxyandrost-4-ene 4000 III N 9 17Alpha-methyl-4-hydroxynandrolone (17alpha-methyl-4-hyd 4000 III N 10 17Alpha-methyl-delta1-dihydrotestosterone (17beta-hydroxy- 4000 III N 17-Alpha-methyl-1-testosterone 11 19-Nor-4-androstenediol (3beta,17beta-dihydroxyestr-4-ene; 4000 III N 12 19-Nor-4-androstenedione (estr-4-en-3,17-dione) 4000 III N 13 19-Nor-5-androstenediol (3beta,17beta-dihydroxyestr-5-ene; 4000 III N 14 19-Nor-5-androstenedione (estr-5-en-3,17-dione) 4000 III N 15 1-Androstenediol (3beta,17beta-dihydroxy-5alpha-androst-1- 4000 III N 16 1-Androstenedione (5alpha-androst-1-en-3,17-dione) 4000 III N 17 1-Methyl-4-phenyl-4-propionoxypiperidine 9661 I Y MPPP, synthetic heroin 18 1-Phenylcyclohexylamine 7460 II N PCP precursor 19 1-Piperidinocyclohexanecarbonitrile 8603 II N PCC, PCP precursor 20 2,5-Dimethoxy-4-(n)-propylthiophenethylamine 7348 I N 2C-T-7 21 2,5-Dimethoxy-4-ethylamphetamine 7399 I N DOET 22 2,5-Dimethoxyamphetamine 7396 I N DMA, 2,5-DMA 23 3,4,5-Trimethoxyamphetamine -

Drugs of Abuseon September Archived 13-10048 No
U.S. DEPARTMENT OF JUSTICE DRUG ENFORCEMENT ADMINISTRATION WWW.DEA.GOV 9, 2014 on September archived 13-10048 No. v. Stewart, in U.S. cited Drugs of2011 Abuse EDITION A DEA RESOURCE GUIDE V. Narcotics WHAT ARE NARCOTICS? Also known as “opioids,” the term "narcotic" comes from the Greek word for “stupor” and originally referred to a variety of substances that dulled the senses and relieved pain. Though some people still refer to all drugs as “narcot- ics,” today “narcotic” refers to opium, opium derivatives, and their semi-synthetic substitutes. A more current term for these drugs, with less uncertainty regarding its meaning, is “opioid.” Examples include the illicit drug heroin and pharmaceutical drugs like OxyContin®, Vicodin®, codeine, morphine, methadone and fentanyl. WHAT IS THEIR ORIGIN? The poppy papaver somniferum is the source for all natural opioids, whereas synthetic opioids are made entirely in a lab and include meperidine, fentanyl, and methadone. Semi-synthetic opioids are synthesized from naturally occurring opium products, such as morphine and codeine, and include heroin, oxycodone, hydrocodone, and hydromorphone. Teens can obtain narcotics from friends, family members, medicine cabinets, pharmacies, nursing 2014 homes, hospitals, hospices, doctors, and the Internet. 9, on September archived 13-10048 No. v. Stewart, in U.S. cited What are common street names? Street names for various narcotics/opioids include: ➔ Hillbilly Heroin, Lean or Purple Drank, OC, Ox, Oxy, Oxycotton, Sippin Syrup What are their forms? Narcotics/opioids come in various forms including: ➔ T ablets, capsules, skin patches, powder, chunks in varying colors (from white to shades of brown and black), liquid form for oral use and injection, syrups, suppositories, lollipops How are they abused? ➔ Narcotics/opioids can be swallowed, smoked, sniffed, or injected. -

New Zealand's Emergent Opioid Trends
New Zealand’s emergent opioid trends - the influences and impacts: Consumer and clinician understanding of New Zealand’s changing patterns of opioid use, availability and impacts Klare Braye A thesis submitted in partial fulfilment of the requirements for the degree of Master of Health Sciences Department of Psychological Medicine University of Otago, Christchurch New Zealand 2014 “Among the remedies which it has pleased Almighty God to give to man to relieve his sufferings, none is so universal and so efficacious as opium”. (Sir Thomas Sydenham, 1680) ~ iii ~ Abstract This thesis explores opioid users and addiction service providers’ understandings of the changing patterns, availability and impacts of opioids and opioid use in New Zealand with a particular focus on the last two decades. Throughout history, the availability of substances of abuse have waxed and waned. Their emergence and availability is influenced by social, legislative and political circumstances. Extensive literature exists related to the use of opioids such as morphine and methadone in New Zealand, and heroin overseas. However, few studies have examined the emerging trends of opioids that are often used as adjunctively to these substances; examples of which in recent years include poppy seed tea (PST), over-the- counter codeine-containing analgesics and most recently some prescribed pain medications. Information regarding the use, availability and impacts of these adjunct opioids from the consumers who use them, and the clinicians who work with these consumers could usefully inform service provision and public policy. This qualitative study, adopting a Husserlian phenomenological philosophy was used, to gain an understanding of the use, access to and implications of these emergent opioid trends. -
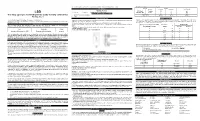
(LSD) Test Dip Card (Urine) • Specimen Collection Container % Agreement 98.8% 99
frozen and stored below -20°C. Frozen specimens should be thawed and mixed before testing. GC/MS. The following results were tabulated: Method GC/MS MATERIALS Total Results Results Positive Negative Materials Provided LSD Rapid Positive 79 1 80 LSD • Test device • Desiccants • Package insert • Urine cups Test Dip card Negative 1 99 100 Materials Required But Not Provided Total Results 80 100 180 One Step Lysergic acid diethylamide (LSD) Test Dip card (Urine) • Specimen collection container % Agreement 98.8% 99. % 98.9% • Timer Package Insert DIRECTIONS FOR USE Analytical Sensitivity This Instruction Sheet is for testing of Lysergic acid diethylamide. Allow the test device, and urine specimen to come to room temperature [15-30°C (59-86°F)] prior to testing. A drug-free urine pool was spiked with LSD at the following concentrations: 0 ng/mL, -50%cutoff, -25%cutoff, cutoff, A rapid, one step test for the qualitative detection of Lysergic acid diethylamide and its metabolites in human urine. 1) Remove the test device from the foil pouch. +25%cutoff and +50%cutoff. The result demonstrates >99% accuracy at 50% above and 50% below the cut-off For forensic use only. 2) Remove the cap from the test device. Label the device with patient or control identifications. concentration. The data are summarized below: INTENDED USE 3) Immerse the absorbent tip into the urine sample for 10-15 seconds. Urine sample should not touch the plastic Lysergic acid diethylamide (LSD) Percent of Visual Result The One Step Lysergic acid diethylamide (LSD) Test Dip card (Urine) is a lateral flow chromatographic device. -

Recent Trends in Illegal Drug Use in New Zealand, 2005-2007
RECENT TRENDS IN ILLEGAL DRUG USE IN NEW ZEALAND, 2005-2007 Findings from the 2005, 2006 and 2007 Illicit Drug Monitoring System (IDMS) C.Wilkins M. Girling P. Sweetsur Centre for Social and Health Outcomes Research and Evaluation Massey University, P O Box 6137, Wellesley St February 2008 © Centre for Social and Health Outcomes Research and Evaluation ISBN 1 877428 07 8 Table of Contents Acknowledgements............................................................................................................................. 8 Executive Summary ............................................................................................................................ 9 Summary ........................................................................................................................................... 11 Introduction....................................................................................................................................11 Method ...........................................................................................................................................11 Demographic characteristics of the frequent drug users................................................................12 Drug use patterns of the frequent methamphetamine users ...........................................................13 Drug use patterns of the frequent ecstasy users .............................................................................14 Drug use patterns of the frequent injecting drug users ..................................................................14 -

Dextropropoxyphene/Diacerein 41 Precautions the Elderly
Dextropropoxyphene/Diacerein 41 Precautions The elderly. The elimination half-lives of dextropropoxyphene 3. Haigh S. 12 Years on: co-proxamol revisited. Lancet 1996; 347: As for Opioid Analgesics in general, p.103. and its metabolite nordextropropoxyphene were prolonged in 1840–1. Correction. ibid.; 348: 346. healthy elderly subjects when compared with young controls.1 4. Sykes JV, et al. Coproxamol revisited. Lancet 1996; 348: 408. Abuse. There have been reports1 of the abuse of dextropropox- After multiple dosing median half-lives of dextropropoxyphene 5. Li Wan Po A, Zhang WY. Systematic overview of co-proxamol 2 to assess analgesic effects of addition of dextropropoxyphene to yphene, and some considered that the ready availability of dex- and nordextropropoxyphene were 36.8 and 41.8 hours, respec- paracetamol. BMJ 1997; 315: 1565–71. Correction ibid. 1998; tropropoxyphene made it liable to abuse although it was a rela- tively in the elderly compared with 22.0 and 22.1 hours in the 316: 116 and 656. tively weak opioid analgesic. However, others3 thought there young subjects. In this study1 there was a strong correlation be- 6. Anonymous. Co-proxamol or paracetamol for acute pain? Drug was no evidence that dextropropoxyphene was frequently asso- tween half-life of nordextropropoxyphene and estimated creati- Ther Bull 1998; 36: 80. ciated with abuse, or concluded that, although there was abuse nine clearance. 7. MHRA. Withdrawal of co-proxamol products and interim updat- ed prescribing information. Message from Professor G Duff, potential, it was of relatively low importance in terms of the com- 1. Flanagan RJ, et al. -

Supplement 1: Additional Tables and Figures
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) BMJ Global Health Supplement 1: Additional tables and figures Box S1: Substances included and excluded from the International Narcotic Control Board (INCB) data on narcotic consumption, in alphabetical order. Opioids included in the opioid consumption calculation: 1. (+)-cis-3-methylfental 35. Bezitramide 2. 3-Acetylmorphine 36. Butyrfentanyl 3. 3-Methylfentanyl 37. Carfentanil 4. 3-Methylthiofentanyl 38. Carfentanyl 5. 3-Monoacetylmorphine 39. Clonitazene 6. 4-Fluoroisobutyrfentanyl 40. Codeine 7. 6-Acetylmorphine 41. Codeine-6GLUC 8. 6-Monoacetylmorphine 42. Codeine-6-glucuronide 9. Acetorphine 43. Codeine-Methyl 10. Acetyl-alpha-methylfentanyl 44. Codeine-N-oxide 11. Acetyldihydrocodeine 45. Codoxime 12. Acetylfentanyl 46. Conc. of poppy straw (C) ACA 13. Acetylmethadol 47. Conc. of poppy straw (C) AMA 14. Acetylmorphine 48. Conc. of poppy straw (C) AOA 15. Acrylfentanyl 49. Conc. of poppy straw (C) ATA 16. AH-7921 50. Conc. of poppy straw (C) GW 17. Alfentanil 51. Conc. of poppy straw (M) ACA 18. Allylprodine 52. Conc. of poppy straw (M) AMA 19. Alphacetylmethadol 53. Conc. of poppy straw (M) AOA 20. Alphameprodine 54. Conc. of poppy straw (M) ATA 21. Alphamethadol 55. Conc. of poppy straw (M) GW 22. alpha-Methylfentanyl 56. Conc. of poppy straw (N) GW 23. alpha-Methylthiofentanyl 57. Conc. of poppy straw (O) 24. Alphaprodine 58. Conc. of poppy straw (O) ACA 25. Anileridine 59. Conc. of poppy straw (O) AMA 26. Benzethidine 60. Conc. of poppy straw (O) AOA 27.